Sat, Jul 18, 2026
[Archive]
Volume 3, Issue 3 (Summer 2017 -- 2017)
JCCNC 2017, 3(3): 223-230 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Hasanpour S E, Rouhi Rahim Begloo E, Jafarian H, Aliyari M, Shariati Moghadam A M, Haghani H et al . The Effect of Aromatherapy Using Lavender Essential Oil on Anxiety in Candidate Patients of Upper Limb Reconstruction Surgery: A Non-Randomized Controlled Clinical Trial. JCCNC 2017; 3 (3) :223-230
URL: http://jccnc.iums.ac.ir/article-1-148-en.html
URL: http://jccnc.iums.ac.ir/article-1-148-en.html
Seyed Esmael Hasanpour1 
 , Elaheh Rouhi Rahim Begloo *2 , Hanieh Jafarian3 , Mansour Aliyari4 , Ali Mohammad Shariati Moghadam5 , Hamid Haghani6 , Hamid Reza Alizadeh Otaghvar1
, Elaheh Rouhi Rahim Begloo *2 , Hanieh Jafarian3 , Mansour Aliyari4 , Ali Mohammad Shariati Moghadam5 , Hamid Haghani6 , Hamid Reza Alizadeh Otaghvar1
, Elaheh Rouhi Rahim Begloo *2 , Hanieh Jafarian3 , Mansour Aliyari4 , Ali Mohammad Shariati Moghadam5 , Hamid Haghani6 , Hamid Reza Alizadeh Otaghvar1
1- Department of Plastic, Reconstructive and Burn Surgery, School of Medicine, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
2- Department of Nursing, School of Nursing & Midwifery, Tehran University of Medical Sciences, Tehran, Iran. ,elahehrouhi032@gmail.com
3- Department of Medical Education, School of Medical Education Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
4- Department of Nursing, School of Nursing and Midwifery, Hamedan University of Medical Sciences, Hamedan, Iran.
5- Department of Intensive Care Nursing, School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran.
6- Department of Biostatistics, School of Public Health, Iran University of Medical Sciences, Tehran, Iran.
2- Department of Nursing, School of Nursing & Midwifery, Tehran University of Medical Sciences, Tehran, Iran. ,
3- Department of Medical Education, School of Medical Education Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
4- Department of Nursing, School of Nursing and Midwifery, Hamedan University of Medical Sciences, Hamedan, Iran.
5- Department of Intensive Care Nursing, School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran.
6- Department of Biostatistics, School of Public Health, Iran University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 547 kb]
(2559 Downloads)
| Abstract (HTML) (6740 Views)
Full-Text: (2144 Views)
1. Background
Surgery is a deliberate change in the anatomical structure of the body in order to facilitate, relieve or eliminate the pathological processes of the body and reconstruct the traumatic injuries (Ni et al. 2013). Reconstructive surgery is one of the important branches of plastic surgery, which is not related to cosmetic surgery and is performed on an abnormal structure in the body; thus, a reconstructive surgical procedure helps to correct the abnormal defects in the body. The defects may be congenital or due to growth anomalies, trauma or large ulcers, infections, tumors, or illness (Gurtner & Neligan 2017).
Preoperative anxiety is a challenging concept in preoperative care. When expecting surgery, most patients experience anxiety, and this response has been accepted as an expectable response (Jawaid et al. 2007). Increased preoperative anxiety is associated with physiological responses such as high blood pressure and irregular heartbeat, which can delay patients’ surgery (Nigussie, Belachew & Wolancho 2014). Complications of anxiety before surgery include increasing the mechanical ventilation time, increasing the incidence of hemodynamic disorders, increasing postoperative pain, taking more analgesics, and requiring more numbness during and immediately after surgery. It has also been shown that an increase in preoperative anxiety levels is associated with neuroendocrine responses released in the post-operative period (Hernández et al. 2015). Research by Nigussie, Belachew & Wolancho (2014) suggests that high preoperative anxiety can prevent post-operative healing (Cho et al. 2013).
In general, two types of pharmacological and non-pharmacological methods are used to reduce anxiety in patients. Many of the non-pharmacological methods that are used today are in the complementary treatment categories. One of these therapies is aromatherapy. Non-pharmacological treatments that are classified as complementary therapies are safe and have fewer side effects compared to pharmacological treatments. Aromatherapy is a complementary treatment, which has grown considerably in recent years (Boehm, Büssing & Ostermann 2012). One of the medicinal herbs used for its aroma essence is lavender (Henry Johannes 2012). Antibacterial, anti-fungal, anti-inflammatory, muscular relaxation, analgesia, somnolence and soothing of lavender have been long known. Due to this, lavender is used in aroma therapy and can have its sedative, analgesic and anti-contraction effects through the neurological system (Soltani et al. 2013). Linalool and Linalyl acetate in this plant can also stimulate the parasympathetic system; Linalyl acetate also has narcotic properties, and the Linalool acts as a sedative (Sköld, Hagvall & Karlberg 2007).
Several studies have been carried out on the effects of aromatherapy on various aspects of the life of patients, including Cho et al. (2013), which found that lavender aromatherapy is effective when used to reduce the anxiety of patients undergoing coronary intervention through the skin (Cho et al. 2013). A reviewed study also suggested that the aromatherapy can be used as a complementary therapy to reduce the symptoms of anxiety, but more studies are needed to demonstrate the biological mechanisms and clinical effects (Lee et al. 2011). A systematic review also showed that in most clinical trials, there is little evidence for lavender’s efficacy, but there are many reports about its safety (Perry et al. 2012).
Considering the importance of decreasing preoperative anxiety in patients, effect of complications due to anxiety on patient’s improvement process and the complementary therapeutic interventions carried out by nurses, this type of treatment represents the art of nursing; and besides knowledge, it should provide more effective care for the patients. Therefore, the researchers tried to study the effect of the aromatherapy on the severity of anxiety among patients undergoing upper limb reconstruction surgery at 15-Khordad Medical & Educational Center in 2016.
2. Materials and Methods
This study is a clinical, one-blind trial with randomized assignment including two groups of aromatherapy and placebo. The study population consisted of patients undergoing upper limb reconstruction surgery who were admitted to the 15-Khordad Plastic and Reconstructive Surgery Hospital in 2017. To determine the required sample size at a confidence level of 95 % and a test power of 80%, and assuming that the size of the effect of aromatherapy on the anxiety score compared with the placebo group is at least d = 0.26 (according to similar studies) in order to consider it statistically significant, after formulating the “sample size formula for comparing the mean of the two populations,” the required sample size was estimated at each group as n = 50, and considering that two groups were needed for this study the total number of samples included 100 subjects (Braden, Reichow & Halm 2009). Samples were selected through convenience sampling method.
The sample size formula for comparing the mean of two populations:
The criteria for entering the study included: having more than 18 years of age, earning a score higher than 20 after responding to the Spielberger questionnaire (minimum score is 20, and scores above 20 can indicate the impact of the intervention); the ability to understand and speak Persian, have reading and writing skills, lack of olfactory disorder, lack of mental illness. The exclusion criteria included acute pain at the time of completion of the questionnaire, the use of benzodiazepines, tranquilizers and psychiatric drugs, the history of eczema and allergy to plants, allergic rhinitis and asthma, history of migraine and chronic headaches, drug addiction (alcohol and cigarette) and unwillingness to participate and willingness of the patient to leave the study. The purpose of the study and its method of implementation were explained to each person briefly, and a written informed consent was obtained from them.
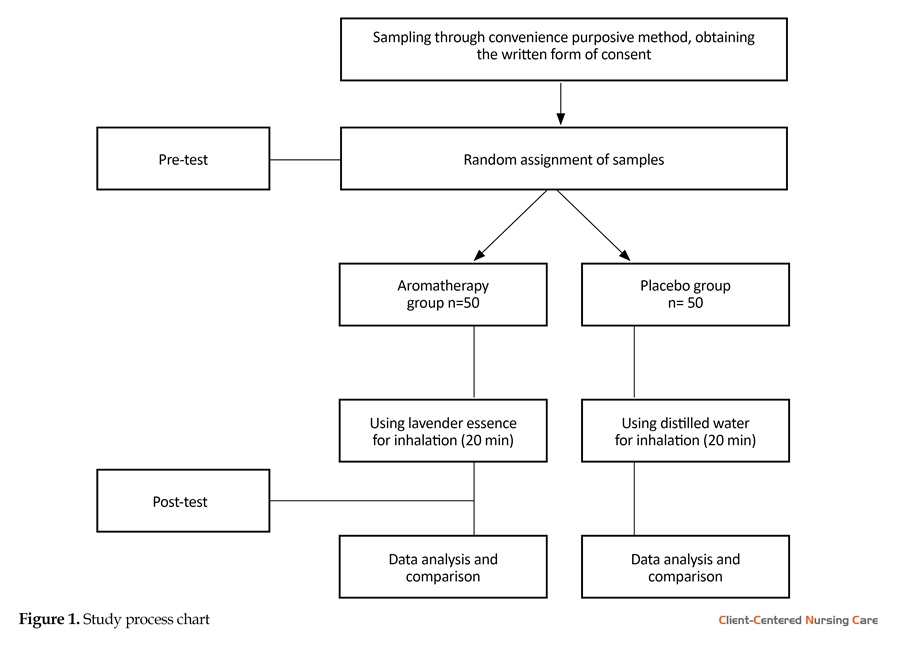
In this research, sampling was done through convenience purposive method, and qualified subjects were randomly assigned to one of the two groups of aromatherapy or placebo. The random allocation method was done by throwing a coin, so if it was head on the coin, the patient was in the aromatherapy group, and if it was tails, the patient was placed in the placebo group. This process continued until the sample size was completed for each group.
The data collection tool was a four-part questionnaire, ALPK2 blood pressure device, and Biomed pulse oximeter device. The first part of questionnaire included demographic information (age, body mass index, marital status, number of children, financial status, educational level, occupation type, insurance coverage and place of residence), the second part included information about the disease (history of hospitalization, history of surgery, preoperative waiting time and surgery area). These two parts were developed according to previous studies and resources. The third part is related to insertion of vital signs, and the fourth part of the questionnaire included the Spielberger State–Trait Anxiety Inventory (STAI).
The questionnaire was interpreted and classified by giving points to positive questions (10 items) such as very low (4), low (3), high (2), and very high (1) points. However, the negative questions (questions 1- 2-5-8-10-11-15-16-19 and 20) were scored in reverse order, i.e., very low (1), low (2), high (3), and very high (4). The total score could be between 20 and 80, which were ranked qualitatively (Bastani, Rouhi Rahim Begloo & Haghani 2015), considered as mild anxiety (20-39), moderate anxiety (40-60) and severe anxiety (60-80) (Pazandeh et al. 2017). Since the research population in the current study had no acute psychological disorders and are selected among the general population, the mean scores were used to assess and compare the state anxiety of the groups. Spielberger test has been used in numerous studies not only in Iran but across the world, and it has acquired validity and reliability (Horwitz 1986).
This research was conducted after receiving a written agreement from the Research Deputy and Ethics Committee of Shahid Beheshti University of Medical Sciences, in the department of Microscopic Surgery of men at the 15 Khordad Medical & Educational Center. The methodology was that after the initial selection of the samples (according to the inclusion criteria), the researcher was introduced to the patient and attracted his or her satisfaction; and then measured their anxiety levels using the Spielberger State Anxiety Inventory, and if the score was more than 20 points, the demographic form and the information on history of disease and the patient’s vital signs were completed by the researcher. After determining the patient’s group and placement in the group, the intervention was performed as follows:
In the aromatherapy group (Muzzarelli, Force & Sebold 2016), the lavender essence (manufactured by Kandelos Co.) was poured onto a non-sterile 2 × 2 gauze, and the patient was asked to breathe in for 20 minutes. In the placebo group, three drops of distilled water were drained by a dropper on a non-sterile gauze of 2 × 2 and inhaled by the patient for 20 minutes (Mirzaei et al. 2015). Five minutes after the intervention period, the vital signs of pulse, blood pressure and respiration were again measured by the researcher and the Spielberger State Anxiety Inventory was completed by the patient (if the patient was not able to complete the questionnaire due to injured hands, every question was read by the researcher for the patient and the patient responded and the researcher recorded in the questionnaire). The intervention was performed on all patients on the day of surgery and by two researchers who were present in the morning shift. It should be noted that the intervention time was between 9:30-11:30 A.M, which was selected based on the patient’s care plan and the rest time. The sampling of this study lasted for 9 months (2016).
To measure the vital signs (blood pressure, pulse and respiration), the ALPK2 pressure device made in Japan was used. Measuring the number of breaths was done by observing the patient’s chest movements, and the number of pulses was recorded with Biomed pulse oximeter made in Germany. The blood pressure and pulse rate of all patients were measured in a lying state and from the healthy hand; the blood pressure unit was mmHg.
This research has been approved by the Ethics Committee of Shahid Beheshti University of Medical Sciences. In order to observe the ethical considerations, a written informed consent was obtained after providing sufficient and clear explanations of the goals and methods of the research in person. This study was registered at Iran’s Clinical Trials (IRCT) with the number IRCT2016060826136N1.
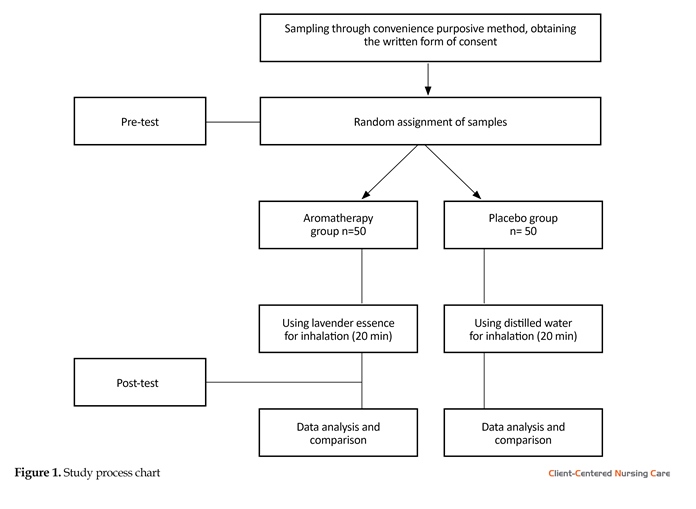
After entering the data in SPSS V.16, the descriptive statistics of frequency, mean and standard deviation were calculated and to evaluate the natural distribution of quantitative variables in each group Kolmogorov-Smirnov test was used. Chi-square test was used to assess the consistency of demographic variables and disease information, and to compare the mean of anxiety severity in the two groups, independent t-test and paired t-test were used. The chart of the study process is shown in Figure 1.
3. Results
The sample of this study was comprised of 100 patients who were candidates for reconstructive surgical operation of the upper limb in two homogenous groups of control and experiment.
In this study, the two groups were homogenous in terms of History of hospitalization (P = 0.77), History of operation (P = 0.14), Waiting time (P = 0.61), Waiting time (P = 0.3), Marital status (P = 0.78), Level of education (P = 0.4), Employment status (P = 0.58), Economic status (P = 0.29).
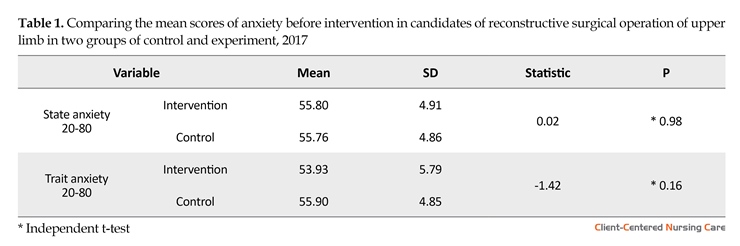
According to the Table 1, the mean of state and trait anxiety in the intervention group before the intervention were (56.88 ± 4.91), (53.93 ± 5.79) and in control group (55.76 ± 4.86), (55.90 ± 4.85), respectively. The results of independent t-test showed that the hypothesis of equality of state and trait anxiety scores between two groups were not significant at 5% error level (t = 0.02, P > 0.05), (t = -1.42, P > 0.05). In other words, before the intervention, there was no difference between the two groups in terms of the level of state and trait anxiety.
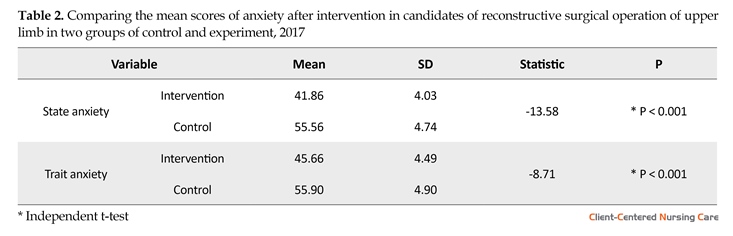
According to the Table 2, the mean of state and trait anxiety group after lavender aromatherapy intervention
Surgery is a deliberate change in the anatomical structure of the body in order to facilitate, relieve or eliminate the pathological processes of the body and reconstruct the traumatic injuries (Ni et al. 2013). Reconstructive surgery is one of the important branches of plastic surgery, which is not related to cosmetic surgery and is performed on an abnormal structure in the body; thus, a reconstructive surgical procedure helps to correct the abnormal defects in the body. The defects may be congenital or due to growth anomalies, trauma or large ulcers, infections, tumors, or illness (Gurtner & Neligan 2017).
Preoperative anxiety is a challenging concept in preoperative care. When expecting surgery, most patients experience anxiety, and this response has been accepted as an expectable response (Jawaid et al. 2007). Increased preoperative anxiety is associated with physiological responses such as high blood pressure and irregular heartbeat, which can delay patients’ surgery (Nigussie, Belachew & Wolancho 2014). Complications of anxiety before surgery include increasing the mechanical ventilation time, increasing the incidence of hemodynamic disorders, increasing postoperative pain, taking more analgesics, and requiring more numbness during and immediately after surgery. It has also been shown that an increase in preoperative anxiety levels is associated with neuroendocrine responses released in the post-operative period (Hernández et al. 2015). Research by Nigussie, Belachew & Wolancho (2014) suggests that high preoperative anxiety can prevent post-operative healing (Cho et al. 2013).
In general, two types of pharmacological and non-pharmacological methods are used to reduce anxiety in patients. Many of the non-pharmacological methods that are used today are in the complementary treatment categories. One of these therapies is aromatherapy. Non-pharmacological treatments that are classified as complementary therapies are safe and have fewer side effects compared to pharmacological treatments. Aromatherapy is a complementary treatment, which has grown considerably in recent years (Boehm, Büssing & Ostermann 2012). One of the medicinal herbs used for its aroma essence is lavender (Henry Johannes 2012). Antibacterial, anti-fungal, anti-inflammatory, muscular relaxation, analgesia, somnolence and soothing of lavender have been long known. Due to this, lavender is used in aroma therapy and can have its sedative, analgesic and anti-contraction effects through the neurological system (Soltani et al. 2013). Linalool and Linalyl acetate in this plant can also stimulate the parasympathetic system; Linalyl acetate also has narcotic properties, and the Linalool acts as a sedative (Sköld, Hagvall & Karlberg 2007).
Several studies have been carried out on the effects of aromatherapy on various aspects of the life of patients, including Cho et al. (2013), which found that lavender aromatherapy is effective when used to reduce the anxiety of patients undergoing coronary intervention through the skin (Cho et al. 2013). A reviewed study also suggested that the aromatherapy can be used as a complementary therapy to reduce the symptoms of anxiety, but more studies are needed to demonstrate the biological mechanisms and clinical effects (Lee et al. 2011). A systematic review also showed that in most clinical trials, there is little evidence for lavender’s efficacy, but there are many reports about its safety (Perry et al. 2012).
Considering the importance of decreasing preoperative anxiety in patients, effect of complications due to anxiety on patient’s improvement process and the complementary therapeutic interventions carried out by nurses, this type of treatment represents the art of nursing; and besides knowledge, it should provide more effective care for the patients. Therefore, the researchers tried to study the effect of the aromatherapy on the severity of anxiety among patients undergoing upper limb reconstruction surgery at 15-Khordad Medical & Educational Center in 2016.
2. Materials and Methods
This study is a clinical, one-blind trial with randomized assignment including two groups of aromatherapy and placebo. The study population consisted of patients undergoing upper limb reconstruction surgery who were admitted to the 15-Khordad Plastic and Reconstructive Surgery Hospital in 2017. To determine the required sample size at a confidence level of 95 % and a test power of 80%, and assuming that the size of the effect of aromatherapy on the anxiety score compared with the placebo group is at least d = 0.26 (according to similar studies) in order to consider it statistically significant, after formulating the “sample size formula for comparing the mean of the two populations,” the required sample size was estimated at each group as n = 50, and considering that two groups were needed for this study the total number of samples included 100 subjects (Braden, Reichow & Halm 2009). Samples were selected through convenience sampling method.
The sample size formula for comparing the mean of two populations:
The criteria for entering the study included: having more than 18 years of age, earning a score higher than 20 after responding to the Spielberger questionnaire (minimum score is 20, and scores above 20 can indicate the impact of the intervention); the ability to understand and speak Persian, have reading and writing skills, lack of olfactory disorder, lack of mental illness. The exclusion criteria included acute pain at the time of completion of the questionnaire, the use of benzodiazepines, tranquilizers and psychiatric drugs, the history of eczema and allergy to plants, allergic rhinitis and asthma, history of migraine and chronic headaches, drug addiction (alcohol and cigarette) and unwillingness to participate and willingness of the patient to leave the study. The purpose of the study and its method of implementation were explained to each person briefly, and a written informed consent was obtained from them.
In this research, sampling was done through convenience purposive method, and qualified subjects were randomly assigned to one of the two groups of aromatherapy or placebo. The random allocation method was done by throwing a coin, so if it was head on the coin, the patient was in the aromatherapy group, and if it was tails, the patient was placed in the placebo group. This process continued until the sample size was completed for each group.
The data collection tool was a four-part questionnaire, ALPK2 blood pressure device, and Biomed pulse oximeter device. The first part of questionnaire included demographic information (age, body mass index, marital status, number of children, financial status, educational level, occupation type, insurance coverage and place of residence), the second part included information about the disease (history of hospitalization, history of surgery, preoperative waiting time and surgery area). These two parts were developed according to previous studies and resources. The third part is related to insertion of vital signs, and the fourth part of the questionnaire included the Spielberger State–Trait Anxiety Inventory (STAI).
The questionnaire was interpreted and classified by giving points to positive questions (10 items) such as very low (4), low (3), high (2), and very high (1) points. However, the negative questions (questions 1- 2-5-8-10-11-15-16-19 and 20) were scored in reverse order, i.e., very low (1), low (2), high (3), and very high (4). The total score could be between 20 and 80, which were ranked qualitatively (Bastani, Rouhi Rahim Begloo & Haghani 2015), considered as mild anxiety (20-39), moderate anxiety (40-60) and severe anxiety (60-80) (Pazandeh et al. 2017). Since the research population in the current study had no acute psychological disorders and are selected among the general population, the mean scores were used to assess and compare the state anxiety of the groups. Spielberger test has been used in numerous studies not only in Iran but across the world, and it has acquired validity and reliability (Horwitz 1986).
This research was conducted after receiving a written agreement from the Research Deputy and Ethics Committee of Shahid Beheshti University of Medical Sciences, in the department of Microscopic Surgery of men at the 15 Khordad Medical & Educational Center. The methodology was that after the initial selection of the samples (according to the inclusion criteria), the researcher was introduced to the patient and attracted his or her satisfaction; and then measured their anxiety levels using the Spielberger State Anxiety Inventory, and if the score was more than 20 points, the demographic form and the information on history of disease and the patient’s vital signs were completed by the researcher. After determining the patient’s group and placement in the group, the intervention was performed as follows:
In the aromatherapy group (Muzzarelli, Force & Sebold 2016), the lavender essence (manufactured by Kandelos Co.) was poured onto a non-sterile 2 × 2 gauze, and the patient was asked to breathe in for 20 minutes. In the placebo group, three drops of distilled water were drained by a dropper on a non-sterile gauze of 2 × 2 and inhaled by the patient for 20 minutes (Mirzaei et al. 2015). Five minutes after the intervention period, the vital signs of pulse, blood pressure and respiration were again measured by the researcher and the Spielberger State Anxiety Inventory was completed by the patient (if the patient was not able to complete the questionnaire due to injured hands, every question was read by the researcher for the patient and the patient responded and the researcher recorded in the questionnaire). The intervention was performed on all patients on the day of surgery and by two researchers who were present in the morning shift. It should be noted that the intervention time was between 9:30-11:30 A.M, which was selected based on the patient’s care plan and the rest time. The sampling of this study lasted for 9 months (2016).
To measure the vital signs (blood pressure, pulse and respiration), the ALPK2 pressure device made in Japan was used. Measuring the number of breaths was done by observing the patient’s chest movements, and the number of pulses was recorded with Biomed pulse oximeter made in Germany. The blood pressure and pulse rate of all patients were measured in a lying state and from the healthy hand; the blood pressure unit was mmHg.
This research has been approved by the Ethics Committee of Shahid Beheshti University of Medical Sciences. In order to observe the ethical considerations, a written informed consent was obtained after providing sufficient and clear explanations of the goals and methods of the research in person. This study was registered at Iran’s Clinical Trials (IRCT) with the number IRCT2016060826136N1.
After entering the data in SPSS V.16, the descriptive statistics of frequency, mean and standard deviation were calculated and to evaluate the natural distribution of quantitative variables in each group Kolmogorov-Smirnov test was used. Chi-square test was used to assess the consistency of demographic variables and disease information, and to compare the mean of anxiety severity in the two groups, independent t-test and paired t-test were used. The chart of the study process is shown in Figure 1.
3. Results
The sample of this study was comprised of 100 patients who were candidates for reconstructive surgical operation of the upper limb in two homogenous groups of control and experiment.
In this study, the two groups were homogenous in terms of History of hospitalization (P = 0.77), History of operation (P = 0.14), Waiting time (P = 0.61), Waiting time (P = 0.3), Marital status (P = 0.78), Level of education (P = 0.4), Employment status (P = 0.58), Economic status (P = 0.29).
According to the Table 1, the mean of state and trait anxiety in the intervention group before the intervention were (56.88 ± 4.91), (53.93 ± 5.79) and in control group (55.76 ± 4.86), (55.90 ± 4.85), respectively. The results of independent t-test showed that the hypothesis of equality of state and trait anxiety scores between two groups were not significant at 5% error level (t = 0.02, P > 0.05), (t = -1.42, P > 0.05). In other words, before the intervention, there was no difference between the two groups in terms of the level of state and trait anxiety.
According to the Table 2, the mean of state and trait anxiety group after lavender aromatherapy intervention


was (41.86 ± 4.03), (45.66 ± 4.49) in intervention and (55.56 ± 4.74), (55.90 ± 4.90) in the control group. After the intervention was ended, independent t-test showed a statistically significant difference in state anxiety levels (t = -13.58, P < 0.001) and the trait anxiety (t = -8.71, P < 0.001) between the two intervention and control groups, which means that the lavender aromatherapy intervention has been able to reduce the level and state and trait anxiety in the intervention group.
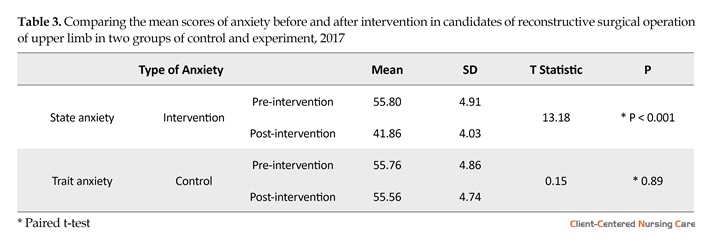
According to the Table 3, the mean score of state and trait anxiety in the intervention group before and after the intervention were (55.80 ± 4.91), (53.93 ± 5.79), and after the intervention (41.86 ± 4.03), (45.66 ± 4.49). The results of paired t-test showed a significant difference in the state and trait anxiety levels before and after the intervention (P < 0.001), which means that this intervention has been able to reduce the state and trait anxiety in the intervention group. In the control group, the state and trait anxiety levels were respectively (55.76 ± 4.86), (55.90 ± 4.85) before the intervention, and (55.56 ± 4.74), (55.97 ± 4.90) after intervention; thus, according to the results of the paired t-test, there was no statistical difference.
4. Discussion
Aromatherapy refers to the use of volatile oils or aromas extracted from aromatic herbs for therapeutic purposes. This treatment is the second most commonly used therapy in the clinical setting by nurses. Today, this treatment is introduced by the US State Boards of Nursing, as
According to the Table 3, the mean score of state and trait anxiety in the intervention group before and after the intervention were (55.80 ± 4.91), (53.93 ± 5.79), and after the intervention (41.86 ± 4.03), (45.66 ± 4.49). The results of paired t-test showed a significant difference in the state and trait anxiety levels before and after the intervention (P < 0.001), which means that this intervention has been able to reduce the state and trait anxiety in the intervention group. In the control group, the state and trait anxiety levels were respectively (55.76 ± 4.86), (55.90 ± 4.85) before the intervention, and (55.56 ± 4.74), (55.97 ± 4.90) after intervention; thus, according to the results of the paired t-test, there was no statistical difference.
4. Discussion
Aromatherapy refers to the use of volatile oils or aromas extracted from aromatic herbs for therapeutic purposes. This treatment is the second most commonly used therapy in the clinical setting by nurses. Today, this treatment is introduced by the US State Boards of Nursing, as

a part of the Holistic Nursing. The nervous system plays a major role in the homeostasis of the body and responses to mental stress and acts both directly and indirectly.
The main objective of this study was to determine the effect of aromatherapy with lavender on the anxiety of patients undergoing upper limb reconstruction surgery. The results of this study indicate that the level of inhaled anxiety in the people who inhaled the aromatherapy with lavender was significantly decreased compared to the previous intervention. The results of this study showed that aromatherapy with lavender essential oil reduced the (obvious) state anxiety of patients, and the results were statistically significant. In a study conducted by Firouzeh Mirzaiee et al (Mirzaei et al. 2015). Which was conducted to determine the effect of lavender on the concentration of cortisol, serotonin, anxiety and hemodynamic changes in pregnant women, it has been found that aroma reduces anxiety, which is consistent with the results of this study. In the study of Muzzarelli, Force and Sebold (2006), which examined the effect of lavender aroma on anxiety, before endoscopy and colonoscopy tests, the Wilcoxon test did not show a significant difference between the level of anxiety before and after the intervention, while in the study of Lehrner et al (Heidari et al. 2013; Muzzarelli, Force & Sebold 2006). on the effect of lavender and orange fragrance on the level of anxiety, mood, level of consciousness and comfort in dentistry patients, it was found that lavender fragrance contributed to lower anxiety, more relaxation and less pain in dentistry patients, which is consistent with the results of the present study.
According to previous studies of the researchers and the effect of variables such as age, sex, level of education, marital status, history of hospitalization, history of surgery and pre-operative waiting time or pre-operative anxiety were examined in both groups. However, both groups were homogeneous before intervention regarding these variables and the level of anxiety.
The results of present study show the significant effect of aromatherapy on reducing the anxiety level of patients undergoing surgical reconstruction of the upper limb. Over the past few years, the lavender essential oil has gained attention in aromatherapy though its effect on reducing the anxiety of patients has been controversial in various studies. For supporting the results of this study, a number of researches showed that inhalation aromatherapy using lavender essential oil can reduce the anxiety level before angiography and coronary stenting, hemodialysis and dentistry, which is consistent with the results of the present study. The effects of aromatherapy are both psychological and physiological. Scientific studies have shown that vegetable oils contain chemical components that have special effects on the mind and body. These compounds can enter the body through the skin or the olfactory system, stimulating the olfactory receptors and transmitting messages through the olfactory nerves, from the receptor cells in the upper nasal region to the olfactory bulb in the vicinity of the limbic system called the amygdala cell and the hippocampus, as a result of which the spirit and feelings, emotions and memory of an individual is affected.
The results of Grunebaum et al. (2011), which showed that lavender essential oil has no effect on the anxiety of patients who are candidates for aesthetic surgery, is not consistent with the results of the present study. The reason for this can be attributed to several factors: 1. The study subjects were patients undergoing a cosmetic surgery; 2. Their different method, in which the gauze was impregnated with 3 drops of essential oil and 60 ml of water for the intervention; and the control group only 60 ml of water; which inhaled the gauze for 60 seconds. Perhaps this dilution and short duration of inhalation prevent the anti-anxiety effects of lavender essential oil.
Due to the different method of study of Muzzarelli et al. the result of present study is not consistent with it. In Muzzarelli study, subjects inhaled 3 drops of lavender essential oil diluted with grape’s seed oil for 5 minutes, but in our study, the intervention group inhaled 3 drops of pure essential oil for 20 minutes. According to the results of this study, the lavender aroma reduces the level of anxiety in the intervention group. Therefore, it is suggested to use lavender essential oil in similar clinical situations to control surgical anxiety. Also, according to the results of this study, essential oil of lavender has no side effects to anyone.
Acknowledgments
The current research has been conducted based on a research project approved by the Ethics Committee of Shahid Beheshti University of Medical Sciences with the code of 177 dated 03/07/2016 and the code of IRCT2016060826136N1 in the Iranian Registry of Clinical Trials. The researchers express their gratitude to counselors and Specialists of Clinical Research Development Unit, 15 Khordad educational Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Conflict of Interest
The authors declared no conflicts of interest.
References
Bastani, F., Rouhi Rahim Begloo, E. & Haghani, H., 2015. Effect of Foot Reflexology on Anxiety of Mothers of High Risk Neonates undergone Cesarean Section: a Non Randomized Controlled Trial. Journal of Hayat, 21(2), pp. 81-94.
Boehm, K., Büssing, A. & Ostermann, T., 2012. Aromatherapy as an adjuvant treatment in cancer care: A descriptive systematic review. African Journal of Traditional, Complementary and Alternative Medicines, 9(4), pp. 503-18. doi: 10.4314/ajtcam.v9i4.7
Braden, R., Reichow, S. & Halm, M. A., 2009. The use of the essential oil lavandin to reduce preoperative anxiety in surgical patients. Journal of PeriAnesthesia Nursing, 24(6), pp. 348–55. doi: 10.1016/j.jopan.2009.10.002
Cho, M. Y. et al., 2013. Effects of aromatherapy on the anxiety, vital signs, and sleep quality of percutaneous coronary intervention patients in intensive care units. Evidence-Based Complementary and Alternative Medicine, 2013, pp. 1–6. doi: 10.1155/2013/381381
Grunebaum, L. D. et al., 2011. Effects of lavender olfactory input on cosmetic procedures. Journal of Cosmetic Dermatology, 10(2), pp. 89–93. doi: 10.1111/j.1473-2165.2011.00554.x
Gurtner, G. C. & Neligan, P. C., 2017. Plastic surgery E-Book; Volume 1: Principles. Amsterdam: Elsevier Health Sciences.
Heidari, A., et al., 2013. The effect of lavender oil inhalation on anxiety and some physiological parameters of open-heart surgery patients. Journal of Research Development in Nursing and Midwifery, 10(2), pp. 1-6.
Henry Johannes, T. E., 2012. Medicinal and aromatic plant research in the 21st century. Medicinal & Aromatic Plants, 1(2), p. e110. doi: 10.4172/2167-0412.1000e110
Hernandez, P. J., et al., 2015. Visual analogue scale for anxiety and Amsterdam preoperative anxiety scale provide a simple and reliable measurement of preoperative anxiety in patients undergoing cardiac surgery. International Cardiovascular Research Journal, 9, pp. 1-6.
Horwitz, E. K., 1986. Preliminary evidence for the reliability and validity of a foreign language anxiety scale. TESOL Quarterly, 20(3), pp. 559-62. doi: 10.2307/3586302
Jawaid, M., et al., 2007. Preoperative anxiety before elective surgery. Neurosciences, 12(2), pp. 145-8.
Lee, Y. L. et al., 2011. A systematic review on the anxiolytic effects of aromatherapy in people with anxiety symptoms. The Journal of Alternative and Complementary Medicine, 17(2), pp. 101–8. doi: 10.1089/acm.2009.0277
Mirzaei, F., et al., 2015. The effect of lavender essence smelling during labor on cortisol and serotonin plasma levels and anxiety reduction in nulliparous women. Journal of Kerman University of Medical Sciences, 16, pp. 245-54.
Muzzarelli, L., Force, M. & Sebold, M., 2006. Aromatherapy and reducing preprocedural anxiety. Gastroenterology Nursing, 29(6), pp. 466–71. doi: 10.1097/00001610-200611000-00005
Ni, C. H. et al., 2013. The anxiolytic effect of aromatherapy on patients awaiting ambulatory surgery: A randomized controlled trial. Evidence-Based Complementary and Alternative Medicine, 2013, pp. 1–5. doi: 10.1155/2013/927419
Nigussie, S., Belachew, T. & Wolancho, W., 2014. Predictors of preoperative anxiety among surgical patients in Jimma University Specialized Teaching Hospital, South Western Ethiopia. BMC Surgery, 14(1), p. 67. doi: 10.1186/1471-2482-14-67
Pazandeh, F., et al., 2017. Anxiety level of pregnant women from Ahwaz exposed to domestic violence. International Journal of Medical Toxicology and Forensic Medicine, 6(4), pp. 217-24.
Perry, R. et al., 2012. Is lavender an anxiolytic drug? A systematic review of randomised clinical trials. Phytomedicine, 19(8-9), pp. 825–35. doi: 10.1016/j.phymed.2012.02.013
Sköld, M., Hagvall, L. & Karlberg, A. T., 2007. Autoxidation of linalyl acetate, the main component of lavender oil, creates potent contact allergens. Contact Dermatitis, 58(1), pp. 9–14. doi: 10.1111/j.1600-0536.2007.01262.x
Soltani, R. et al., 2013. Evaluation of the effect of aromatherapy with lavender essential oil on post-tonsillectomy pain in pediatric patients: A randomized controlled trial. International Journal of Pediatric Otorhinolaryngology, 77(9), pp. 1579–81. doi: 10.1016/j.ijporl.2013.07.014
The main objective of this study was to determine the effect of aromatherapy with lavender on the anxiety of patients undergoing upper limb reconstruction surgery. The results of this study indicate that the level of inhaled anxiety in the people who inhaled the aromatherapy with lavender was significantly decreased compared to the previous intervention. The results of this study showed that aromatherapy with lavender essential oil reduced the (obvious) state anxiety of patients, and the results were statistically significant. In a study conducted by Firouzeh Mirzaiee et al (Mirzaei et al. 2015). Which was conducted to determine the effect of lavender on the concentration of cortisol, serotonin, anxiety and hemodynamic changes in pregnant women, it has been found that aroma reduces anxiety, which is consistent with the results of this study. In the study of Muzzarelli, Force and Sebold (2006), which examined the effect of lavender aroma on anxiety, before endoscopy and colonoscopy tests, the Wilcoxon test did not show a significant difference between the level of anxiety before and after the intervention, while in the study of Lehrner et al (Heidari et al. 2013; Muzzarelli, Force & Sebold 2006). on the effect of lavender and orange fragrance on the level of anxiety, mood, level of consciousness and comfort in dentistry patients, it was found that lavender fragrance contributed to lower anxiety, more relaxation and less pain in dentistry patients, which is consistent with the results of the present study.
According to previous studies of the researchers and the effect of variables such as age, sex, level of education, marital status, history of hospitalization, history of surgery and pre-operative waiting time or pre-operative anxiety were examined in both groups. However, both groups were homogeneous before intervention regarding these variables and the level of anxiety.
The results of present study show the significant effect of aromatherapy on reducing the anxiety level of patients undergoing surgical reconstruction of the upper limb. Over the past few years, the lavender essential oil has gained attention in aromatherapy though its effect on reducing the anxiety of patients has been controversial in various studies. For supporting the results of this study, a number of researches showed that inhalation aromatherapy using lavender essential oil can reduce the anxiety level before angiography and coronary stenting, hemodialysis and dentistry, which is consistent with the results of the present study. The effects of aromatherapy are both psychological and physiological. Scientific studies have shown that vegetable oils contain chemical components that have special effects on the mind and body. These compounds can enter the body through the skin or the olfactory system, stimulating the olfactory receptors and transmitting messages through the olfactory nerves, from the receptor cells in the upper nasal region to the olfactory bulb in the vicinity of the limbic system called the amygdala cell and the hippocampus, as a result of which the spirit and feelings, emotions and memory of an individual is affected.
The results of Grunebaum et al. (2011), which showed that lavender essential oil has no effect on the anxiety of patients who are candidates for aesthetic surgery, is not consistent with the results of the present study. The reason for this can be attributed to several factors: 1. The study subjects were patients undergoing a cosmetic surgery; 2. Their different method, in which the gauze was impregnated with 3 drops of essential oil and 60 ml of water for the intervention; and the control group only 60 ml of water; which inhaled the gauze for 60 seconds. Perhaps this dilution and short duration of inhalation prevent the anti-anxiety effects of lavender essential oil.
Due to the different method of study of Muzzarelli et al. the result of present study is not consistent with it. In Muzzarelli study, subjects inhaled 3 drops of lavender essential oil diluted with grape’s seed oil for 5 minutes, but in our study, the intervention group inhaled 3 drops of pure essential oil for 20 minutes. According to the results of this study, the lavender aroma reduces the level of anxiety in the intervention group. Therefore, it is suggested to use lavender essential oil in similar clinical situations to control surgical anxiety. Also, according to the results of this study, essential oil of lavender has no side effects to anyone.
Acknowledgments
The current research has been conducted based on a research project approved by the Ethics Committee of Shahid Beheshti University of Medical Sciences with the code of 177 dated 03/07/2016 and the code of IRCT2016060826136N1 in the Iranian Registry of Clinical Trials. The researchers express their gratitude to counselors and Specialists of Clinical Research Development Unit, 15 Khordad educational Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Conflict of Interest
The authors declared no conflicts of interest.
References
Bastani, F., Rouhi Rahim Begloo, E. & Haghani, H., 2015. Effect of Foot Reflexology on Anxiety of Mothers of High Risk Neonates undergone Cesarean Section: a Non Randomized Controlled Trial. Journal of Hayat, 21(2), pp. 81-94.
Boehm, K., Büssing, A. & Ostermann, T., 2012. Aromatherapy as an adjuvant treatment in cancer care: A descriptive systematic review. African Journal of Traditional, Complementary and Alternative Medicines, 9(4), pp. 503-18. doi: 10.4314/ajtcam.v9i4.7
Braden, R., Reichow, S. & Halm, M. A., 2009. The use of the essential oil lavandin to reduce preoperative anxiety in surgical patients. Journal of PeriAnesthesia Nursing, 24(6), pp. 348–55. doi: 10.1016/j.jopan.2009.10.002
Cho, M. Y. et al., 2013. Effects of aromatherapy on the anxiety, vital signs, and sleep quality of percutaneous coronary intervention patients in intensive care units. Evidence-Based Complementary and Alternative Medicine, 2013, pp. 1–6. doi: 10.1155/2013/381381
Grunebaum, L. D. et al., 2011. Effects of lavender olfactory input on cosmetic procedures. Journal of Cosmetic Dermatology, 10(2), pp. 89–93. doi: 10.1111/j.1473-2165.2011.00554.x
Gurtner, G. C. & Neligan, P. C., 2017. Plastic surgery E-Book; Volume 1: Principles. Amsterdam: Elsevier Health Sciences.
Heidari, A., et al., 2013. The effect of lavender oil inhalation on anxiety and some physiological parameters of open-heart surgery patients. Journal of Research Development in Nursing and Midwifery, 10(2), pp. 1-6.
Henry Johannes, T. E., 2012. Medicinal and aromatic plant research in the 21st century. Medicinal & Aromatic Plants, 1(2), p. e110. doi: 10.4172/2167-0412.1000e110
Hernandez, P. J., et al., 2015. Visual analogue scale for anxiety and Amsterdam preoperative anxiety scale provide a simple and reliable measurement of preoperative anxiety in patients undergoing cardiac surgery. International Cardiovascular Research Journal, 9, pp. 1-6.
Horwitz, E. K., 1986. Preliminary evidence for the reliability and validity of a foreign language anxiety scale. TESOL Quarterly, 20(3), pp. 559-62. doi: 10.2307/3586302
Jawaid, M., et al., 2007. Preoperative anxiety before elective surgery. Neurosciences, 12(2), pp. 145-8.
Lee, Y. L. et al., 2011. A systematic review on the anxiolytic effects of aromatherapy in people with anxiety symptoms. The Journal of Alternative and Complementary Medicine, 17(2), pp. 101–8. doi: 10.1089/acm.2009.0277
Mirzaei, F., et al., 2015. The effect of lavender essence smelling during labor on cortisol and serotonin plasma levels and anxiety reduction in nulliparous women. Journal of Kerman University of Medical Sciences, 16, pp. 245-54.
Muzzarelli, L., Force, M. & Sebold, M., 2006. Aromatherapy and reducing preprocedural anxiety. Gastroenterology Nursing, 29(6), pp. 466–71. doi: 10.1097/00001610-200611000-00005
Ni, C. H. et al., 2013. The anxiolytic effect of aromatherapy on patients awaiting ambulatory surgery: A randomized controlled trial. Evidence-Based Complementary and Alternative Medicine, 2013, pp. 1–5. doi: 10.1155/2013/927419
Nigussie, S., Belachew, T. & Wolancho, W., 2014. Predictors of preoperative anxiety among surgical patients in Jimma University Specialized Teaching Hospital, South Western Ethiopia. BMC Surgery, 14(1), p. 67. doi: 10.1186/1471-2482-14-67
Pazandeh, F., et al., 2017. Anxiety level of pregnant women from Ahwaz exposed to domestic violence. International Journal of Medical Toxicology and Forensic Medicine, 6(4), pp. 217-24.
Perry, R. et al., 2012. Is lavender an anxiolytic drug? A systematic review of randomised clinical trials. Phytomedicine, 19(8-9), pp. 825–35. doi: 10.1016/j.phymed.2012.02.013
Sköld, M., Hagvall, L. & Karlberg, A. T., 2007. Autoxidation of linalyl acetate, the main component of lavender oil, creates potent contact allergens. Contact Dermatitis, 58(1), pp. 9–14. doi: 10.1111/j.1600-0536.2007.01262.x
Soltani, R. et al., 2013. Evaluation of the effect of aromatherapy with lavender essential oil on post-tonsillectomy pain in pediatric patients: A randomized controlled trial. International Journal of Pediatric Otorhinolaryngology, 77(9), pp. 1579–81. doi: 10.1016/j.ijporl.2013.07.014
Type of Study: Applicable |
Subject:
Special
Received: 2017/01/16 | Accepted: 2017/05/23 | Published: 2017/08/1
Received: 2017/01/16 | Accepted: 2017/05/23 | Published: 2017/08/1
References
1. Bastani, F., Rouhi Rahim Begloo, E. & Haghani, H., 2015. Effect of Foot Reflexology on Anxiety of Mothers of High Risk Neonates undergone Cesarean Section: a Non Randomized Controlled Trial. Journal of Hayat, 21(2), pp. 81-94.
2. Boehm, K., Büssing, A. & Ostermann, T., 2012. Aromatherapy as an adjuvant treatment in cancer care: A descriptive systematic review. African Journal of Traditional, Complementary and Alternative Medicines, 9(4), pp. 503-18. doi: 10.4314/ajtcam.v9i4.7 [DOI:10.4314/ajtcam.v9i4.7]
3. Braden, R., Reichow, S. & Halm, M. A., 2009. The use of the essential oil lavandin to reduce preoperative anxiety in surgical patients. Journal of PeriAnesthesia Nursing, 24(6), pp. 348–55. doi: 10.1016/j.jopan.2009.10.002 [DOI:10.1016/j.jopan.2009.10.002]
4. Cho, M. Y. et al., 2013. Effects of aromatherapy on the anxiety, vital signs, and sleep quality of percutaneous coronary intervention patients in intensive care units. Evidence-Based Complementary and Alternative Medicine, 2013, pp. 1–6. doi: 10.1155/2013/381381 [DOI:10.1155/2013/381381]
5. Grunebaum, L. D. et al., 2011. Effects of lavender olfactory input on cosmetic procedures. Journal of Cosmetic Dermatology, 10(2), pp. 89–93. doi: 10.1111/j.1473-2165.2011.00554.x [DOI:10.1111/j.1473-2165.2011.00554.x]
6. Gurtner, G. C. & Neligan, P. C., 2017. Plastic surgery E-Book; Volume 1: Principles. Amsterdam: Elsevier Health Sciences.
7. Heidari, A., et al., 2013. The effect of lavender oil inhalation on anxiety and some physiological parameters of open-heart surgery patients. Journal of Research Development in Nursing and Midwifery, 10(2), pp. 1-6.
8. Henry Johannes, T. E., 2012. Medicinal and aromatic plant research in the 21st century. Medicinal & Aromatic Plants, 1(2), p. e110. doi: 10.4172/2167-0412.1000e110 [DOI:10.4172/2167-0412.1000e110]
9. Hernandez, P. J., et al., 2015. Visual analogue scale for anxiety and Amsterdam preoperative anxiety scale provide a simple and reliable measurement of preoperative anxiety in patients undergoing cardiac surgery. International Cardiovascular Research Journal, 9, pp. 1-6.
10. Horwitz, E. K., 1986. Preliminary evidence for the reliability and validity of a foreign language anxiety scale. TESOL Quarterly, 20(3), pp. 559-62. doi: 10.2307/3586302 [DOI:10.2307/3586302]
11. Jawaid, M., et al., 2007. Preoperative anxiety before elective surgery. Neurosciences, 12(2), pp. 145-8. [PMID]
12. Lee, Y. L. et al., 2011. A systematic review on the anxiolytic effects of aromatherapy in people with anxiety symptoms. The Journal of Alternative and Complementary Medicine, 17(2), pp. 101–8. doi: 10.1089/acm.2009.0277 [DOI:10.1089/acm.2009.0277]
13. Mirzaei, F., et al., 2015. The effect of lavender essence smelling during labor on cortisol and serotonin plasma levels and anxiety reduction in nulliparous women. Journal of Kerman University of Medical Sciences, 16, pp. 245-54.
14. Muzzarelli, L., Force, M. & Sebold, M., 2006. Aromatherapy and reducing preprocedural anxiety. Gastroenterology Nursing, 29(6), pp. 466–71. doi: 10.1097/00001610-200611000-00005 [DOI:10.1097/00001610-200611000-00005]
15. Ni, C. H. et al., 2013. The anxiolytic effect of aromatherapy on patients awaiting ambulatory surgery: A randomized controlled trial. Evidence-Based Complementary and Alternative Medicine, 2013, pp. 1–5. doi: 10.1155/2013/927419 [DOI:10.1155/2013/927419]
16. Nigussie, S., Belachew, T. & Wolancho, W., 2014. Predictors of preoperative anxiety among surgical patients in Jimma University Specialized Teaching Hospital, South Western Ethiopia. BMC Surgery, 14(1), p. 67. doi: 10.1186/1471-2482-14-67 [DOI:10.1186/1471-2482-14-67]
17. Pazandeh, F., et al., 2017. Anxiety level of pregnant women from Ahwaz exposed to domestic violence. International Journal of Medical Toxicology and Forensic Medicine, 6(4), pp. 217-24.
18. Perry, R. et al., 2012. Is lavender an anxiolytic drug? A systematic review of randomised clinical trials. Phytomedicine, 19(8-9), pp. 825–35. doi: 10.1016/j.phymed.2012.02.013 [DOI:10.1016/j.phymed.2012.02.013]
19. Sköld, M., Hagvall, L. & Karlberg, A. T., 2007. Autoxidation of linalyl acetate, the main component of lavender oil, creates potent contact allergens. Contact Dermatitis, 58(1), pp. 9–14. doi: 10.1111/j.1600-0536.2007.01262.x [DOI:10.1111/j.1600-0536.2007.01262.x]
20. Soltani, R. et al., 2013. Evaluation of the effect of aromatherapy with lavender essential oil on post-tonsillectomy pain in pediatric patients: A randomized controlled trial. International Journal of Pediatric Otorhinolaryngology, 77(9), pp. 1579–81. doi: 10.1016/j.ijporl.2013.07.014 [DOI:10.1016/j.ijporl.2013.07.014]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
