Tue, Jul 1, 2025
[Archive]
Volume 4, Issue 4 (Autumn 2018)
JCCNC 2018, 4(4): 223-230 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Lashgarizad K, Salehi T, Ashghali Farahani M, Haghani H. Investigating Knowledge of Patients Undergoing Total Knee Replacement. JCCNC 2018; 4 (4) :223-230
URL: http://jccnc.iums.ac.ir/article-1-195-en.html
URL: http://jccnc.iums.ac.ir/article-1-195-en.html



1- Department of Nursing, Faculty of Nursing and Midwifery, Iran University of Medical Sciences, Tehran, Iran.
2- Department of Nursing, Faculty of Nursing and Midwifery, Iran University of Medical Sciences, Tehran, Iran. ,salehi.t@iums.ac.ir
2- Department of Nursing, Faculty of Nursing and Midwifery, Iran University of Medical Sciences, Tehran, Iran. ,
Full-Text [PDF 547 kb]
(1192 Downloads)
| Abstract (HTML) (2783 Views)
● The knowledge of patients undergoing total knee replacement is poor.
● Patients got the highest score in the financial dimension and the lowest score in the ethical dimension.
● Managers and nursing staff can help to promote the level of knowledge in such patients by planning and executing regular educational programs.
Plain Language Summary
Patients received the highest knowledge after TKP surgery in the financial dimension and the lowest knowledge in the ethical dimension. It means they needed more training. Nursing managers and nursing staff can help to improve the level of knowledge in such patients by planning and executing regular educational programs and consequently providing the opportunities to improve self-care in the patients.
● Patients got the highest score in the financial dimension and the lowest score in the ethical dimension.
● Managers and nursing staff can help to promote the level of knowledge in such patients by planning and executing regular educational programs.
Plain Language Summary
Patients received the highest knowledge after TKP surgery in the financial dimension and the lowest knowledge in the ethical dimension. It means they needed more training. Nursing managers and nursing staff can help to improve the level of knowledge in such patients by planning and executing regular educational programs and consequently providing the opportunities to improve self-care in the patients.
Full-Text: (992 Views)
Plain Language Summary
Patients received the highest knowledge after TKP surgery in the financial dimension and the lowest knowledge in the ethical dimension. It means they needed more training. Nursing managers and nursing staff can help to improve the level of knowledge in such patients by planning and executing regular educational programs and consequently providing the opportunities to improve self-care in the patients..
1. Background
Osteoarthritis is a common and very devastating disease that affects one or both knees. In the United States, more than 4.5 million people live with knee osteoarthritis (Tehrani‐Banihashemi et al. 2014) and its prevalence in Iran is estimated 19.34%, which shows its growth in the country (Tehrani‐Banihashemi et al. 2014). According to the World Health Organization, the disease will be the fourth cause of physical disability in the world by 2020 (Jalali et al. 2015).
There is no well-known treatment for arthritis, and therapies are designed to reduce pain and movement limitations. When medication and non-invasive treatments are not helpful, Total Knee Replacement (TKR) is the treatment of choice that can reduce pain and improve quality of life in patients with degenerative knee joint diseases (Bonnin et al. 2010). Demand for TKR is rising since it increases life expectancy, and public expectations for wellbeing and delays the disease progression (Jafari et al. 2017).
Compared to other therapeutic methods, TKR has significant advantages due to its cost-effectiveness and its impact on the patient’s quality of life (Motififard & Mir Amirkhani 2012). Released statistics indicate that about 300,000 patients underwent TKR surgery in the United States annually, which is expected to increase by 6.1% by 2030 (Ghaeeni & Amirkhani 2015).
Such patients expect to be considered by health care providers (Farahani et al. 2013) and receive adequate information and knowledge (Lewis et al. 2014). Therefore, patients undergoing TKR surgery need nursing care and education in all fields, including infection prevention, pain management, prevention of deep vein thrombosis, leaving the bed, rehabilitation, and daily activities. As the quality of care and education improves, the level of knowledge increases, which in turn leads to the improvement of knee performance and reduction of postoperative complications (Thomsen et al. 2016).
However, in Iran, the time to educate patients is very limited (Farahani et al. 2013). Patient education is considered as an important task and one of the quality standards of nursing care, and it is necessary to be implemented and evaluated like other nursing interventions (Tahery et al. 2011). Orthopedic patients’ education is also an important part of nursing care process leading to a more positive effect of care and treatment. On the other hand, there is a close relationship between the knowledge received and the quality of life in such patients (Montin et al. 2010).
Patients should be able to restore muscle strength and joint function in both legs after surgery; but many of such patients are not able to do so due to lack of sufficient knowledge about the process of knee performance improvement . More than 76,000 cases of knee replacement surgeries are performed annually in the UK, and 5% of them require another surgery for up to 10 years. Among the causes of repeated surgeries is inadequate knowledge about care, which leads to poor knee performance, knee stiffness, and persistence of pain (Khan et al. 2016).
Studies show that only 26% of individuals have an effective and planned physical activity after discharge (Pozzi et al. 2013). Some researches of the health centers in Iran also stated that patient education is not good and the patient and his/her family and also the society should face the consequent problems (Tahery et al. 2011).
Experiences of the researchers working in the orthopedic departments for many years indicate the frequent visits and contacts of patients after surgery to ask questions about their care. It seems that they have not received the essential education. Also, the growth of TKA in recent years, the importance of knowledge of patients after surgery, and conduction no studies to meet the needs in Iran so far, indicate the need for more studies on this issue. Accordingly, the current study aimed at determining the knowledge of patients undergoing total knee replacement referring to selected hospitals in Tehran/Iran.
2. Materials and Methods
Sample
The current descriptive cross-sectional study was conducted on 140 patients under TKR referring to selected hospitals of Iran University of Medical Sciences; the subjects were recruited by convenience sampling method. The inclusion criteria were: undergoing TKA minimum two weeks and maximum 28 weeks before the study, age range of 18-65 years (Huber et al. 2013), lack of known psychological illnesses according to the patient, lack of any type of disease affecting the muscle strength and balance, lack of complications associated with surgery such as infection of the surgery site based on the clinician’s diagnosis, and lack of previous knee replacement.
The researcher completed the questionnaires by interview after taking approval from the ethics committee of Iran University of Medical Sciences. The interviews were carried out in the orthopedic clinic of the hospitals, and each took 20 minutes.
Instrument and data collection
The data were collected by two structured questionnaires. The first questionnaire included demographic information such as age, gender, marital status, and level of education. The second one was the Received Knowledge of Hospital Patients (RKHP), first designed in 1994 by Leino-kilpi & Vuorenhemio, and included 40 items in six dimensions. Biophysiological (eight items: knowledge about symptoms, examinations, treatment, and complications), functional (eight items: knowledge about daily life, rest, mobility, nutrition, body hygiene, elimination, equipment, and aids), experimental (three items: knowledge about emotions, earlier health, and hospital experiences), ethical (nine items: Knowledge about decision-making, patient’s rights, duties, confidentiality), social (six items: knowledge about social support from relatives, significant others, and patients support groups, etc.), and financial (six items: Knowledge about costs related to rehabilitation, insurance, continuity of care and medication).
The patients were asked to rank each item based on a Likert scale (1=completely agree, 4=completely disagree); a fifth option was also included (0=“Does not apply”) (Montin et al. 2010). The lowest score (40), indicated more received knowledge, and the highest score (160) indicated the lowest knowledge that the patient received.
The reliability of RKHP questionnaire in the study by Klemetti (2014) was estimated 0.89-0.95. In the present study, Cronbach's α coefficient (0.807) was obtained, which was an acceptable and appropriate reliability coefficient. Validity was achieved through content validation by ten qualified professors. The collected data were analyzed by SPSS V. 19 using descriptive and inferential statistical tests such as mean, standard deviation, and minimum and maximum.
3. Results
Characteristics of the Sample
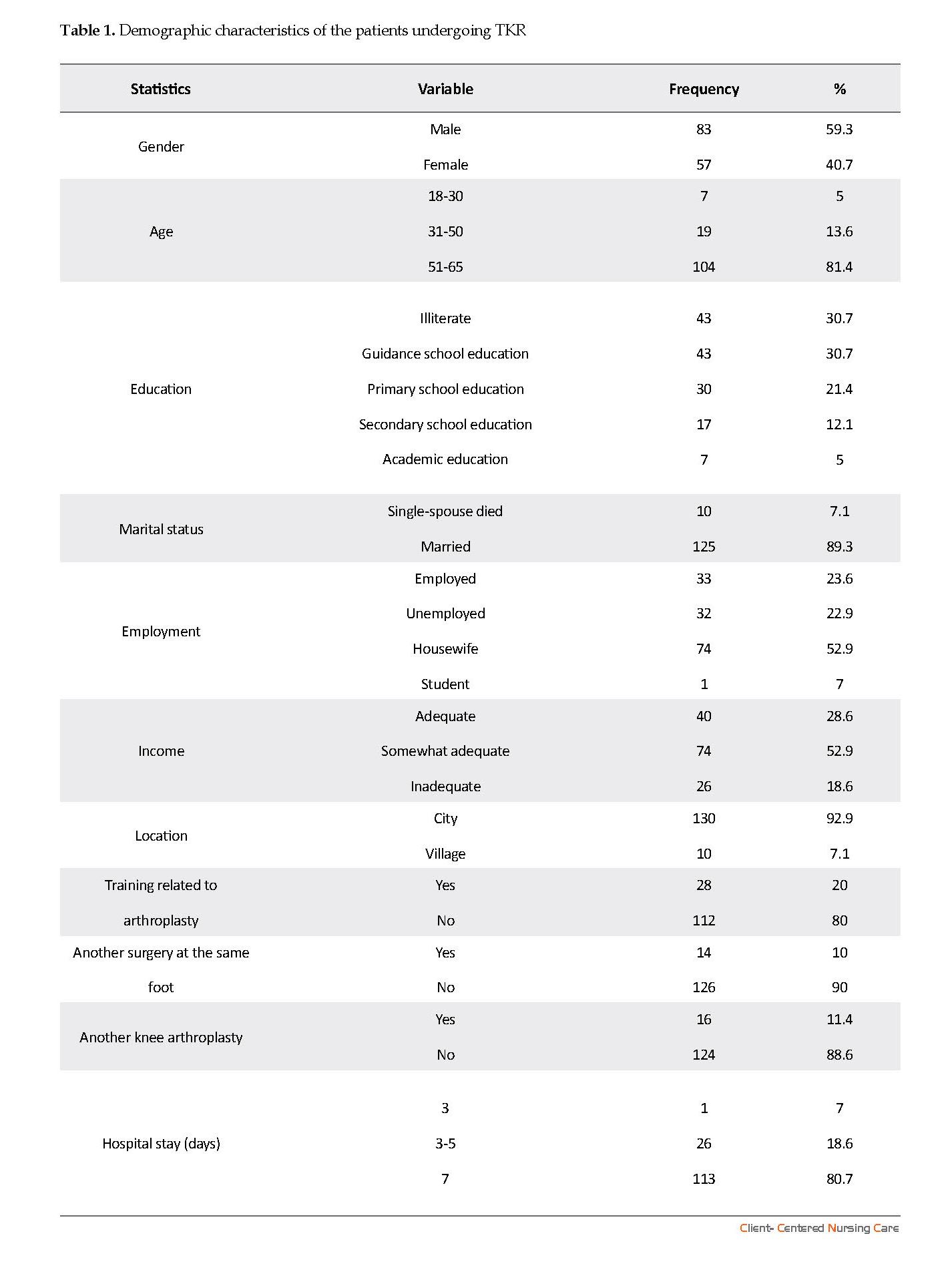
The demographic characteristics of the patients (Table 1) indicated that most of the subjects were in the age range of 51-65 (81.4%), female (59.3%), housewives (52.9%), married (89.3%), urban residents (92.9%), and with sufficient income and secondary education level and illiterate (43%). The majority of participants in the study were not educated about arthroplasty (80%), had no history of another surgical procedure on the same foot (90%), had no history of other knee arthroplasty (86.6%), and the length of their stay at the hospital was 5-7 days (80.7%).
Knowledge score in six Dimensions
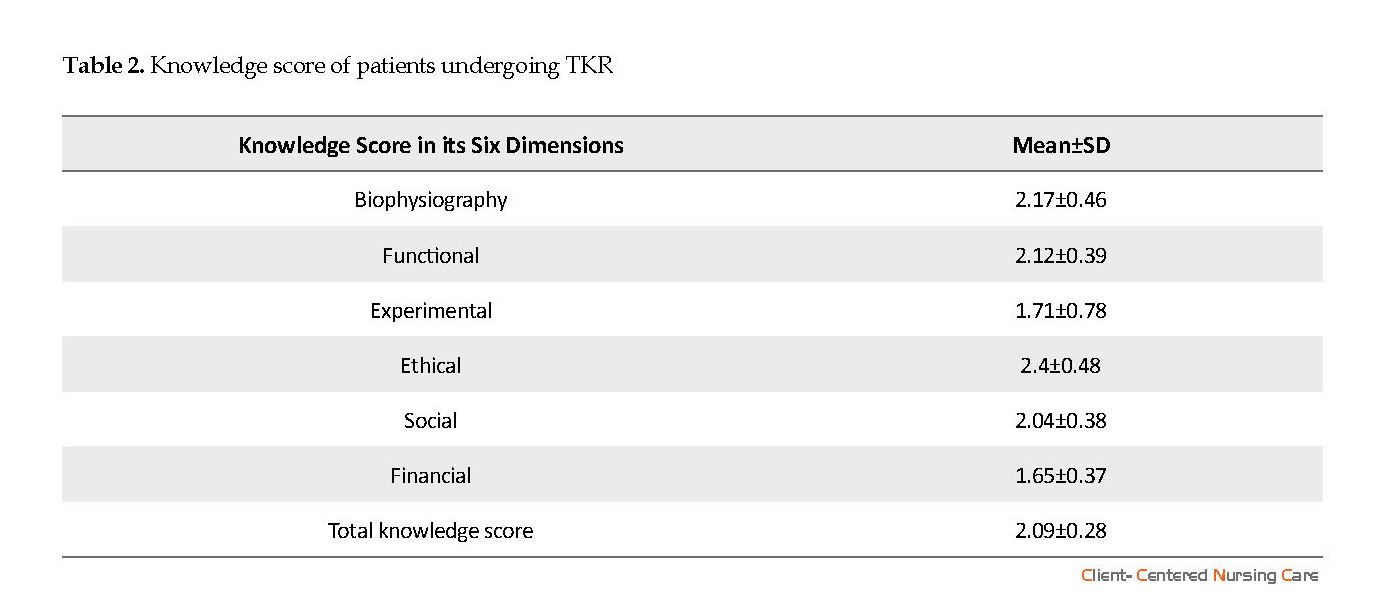
The mean score of total knowledge was (2.09) with SD=0.28. This score was higher than the average score (2) of knowledge, which indicated that the level of knowledge was unacceptable and suggested that patients needed to receive more information. Also, the highest mean (2.46) was in the ethical dimension, which indicated that the knowledge of patients was less in this dimension than the other dimensions, and the lowest mean was in the economic dimension (1.65), which indicated that the knowledge of patients was more in this dimension than the other dimensions (Table 2).
4. Discussion
Research on knowledge of patients undergoing TKR is very limited in Iran and such a study is not conducted so far. In terms of knowledge score and its six dimensions, the knowledge score in the present study was higher than the average, which indicated an inadequate level of knowledge of patients. Patients received the highest score in the financial aspect, and the lowest score in the ethical dimension.
Patients received the highest knowledge after TKP surgery in the financial dimension and the lowest knowledge in the ethical dimension. It means they needed more training. Nursing managers and nursing staff can help to improve the level of knowledge in such patients by planning and executing regular educational programs and consequently providing the opportunities to improve self-care in the patients..
1. Background
Osteoarthritis is a common and very devastating disease that affects one or both knees. In the United States, more than 4.5 million people live with knee osteoarthritis (Tehrani‐Banihashemi et al. 2014) and its prevalence in Iran is estimated 19.34%, which shows its growth in the country (Tehrani‐Banihashemi et al. 2014). According to the World Health Organization, the disease will be the fourth cause of physical disability in the world by 2020 (Jalali et al. 2015).
There is no well-known treatment for arthritis, and therapies are designed to reduce pain and movement limitations. When medication and non-invasive treatments are not helpful, Total Knee Replacement (TKR) is the treatment of choice that can reduce pain and improve quality of life in patients with degenerative knee joint diseases (Bonnin et al. 2010). Demand for TKR is rising since it increases life expectancy, and public expectations for wellbeing and delays the disease progression (Jafari et al. 2017).
Compared to other therapeutic methods, TKR has significant advantages due to its cost-effectiveness and its impact on the patient’s quality of life (Motififard & Mir Amirkhani 2012). Released statistics indicate that about 300,000 patients underwent TKR surgery in the United States annually, which is expected to increase by 6.1% by 2030 (Ghaeeni & Amirkhani 2015).
Such patients expect to be considered by health care providers (Farahani et al. 2013) and receive adequate information and knowledge (Lewis et al. 2014). Therefore, patients undergoing TKR surgery need nursing care and education in all fields, including infection prevention, pain management, prevention of deep vein thrombosis, leaving the bed, rehabilitation, and daily activities. As the quality of care and education improves, the level of knowledge increases, which in turn leads to the improvement of knee performance and reduction of postoperative complications (Thomsen et al. 2016).
However, in Iran, the time to educate patients is very limited (Farahani et al. 2013). Patient education is considered as an important task and one of the quality standards of nursing care, and it is necessary to be implemented and evaluated like other nursing interventions (Tahery et al. 2011). Orthopedic patients’ education is also an important part of nursing care process leading to a more positive effect of care and treatment. On the other hand, there is a close relationship between the knowledge received and the quality of life in such patients (Montin et al. 2010).
Patients should be able to restore muscle strength and joint function in both legs after surgery; but many of such patients are not able to do so due to lack of sufficient knowledge about the process of knee performance improvement . More than 76,000 cases of knee replacement surgeries are performed annually in the UK, and 5% of them require another surgery for up to 10 years. Among the causes of repeated surgeries is inadequate knowledge about care, which leads to poor knee performance, knee stiffness, and persistence of pain (Khan et al. 2016).
Studies show that only 26% of individuals have an effective and planned physical activity after discharge (Pozzi et al. 2013). Some researches of the health centers in Iran also stated that patient education is not good and the patient and his/her family and also the society should face the consequent problems (Tahery et al. 2011).
Experiences of the researchers working in the orthopedic departments for many years indicate the frequent visits and contacts of patients after surgery to ask questions about their care. It seems that they have not received the essential education. Also, the growth of TKA in recent years, the importance of knowledge of patients after surgery, and conduction no studies to meet the needs in Iran so far, indicate the need for more studies on this issue. Accordingly, the current study aimed at determining the knowledge of patients undergoing total knee replacement referring to selected hospitals in Tehran/Iran.
2. Materials and Methods
Sample
The current descriptive cross-sectional study was conducted on 140 patients under TKR referring to selected hospitals of Iran University of Medical Sciences; the subjects were recruited by convenience sampling method. The inclusion criteria were: undergoing TKA minimum two weeks and maximum 28 weeks before the study, age range of 18-65 years (Huber et al. 2013), lack of known psychological illnesses according to the patient, lack of any type of disease affecting the muscle strength and balance, lack of complications associated with surgery such as infection of the surgery site based on the clinician’s diagnosis, and lack of previous knee replacement.
The researcher completed the questionnaires by interview after taking approval from the ethics committee of Iran University of Medical Sciences. The interviews were carried out in the orthopedic clinic of the hospitals, and each took 20 minutes.
Instrument and data collection
The data were collected by two structured questionnaires. The first questionnaire included demographic information such as age, gender, marital status, and level of education. The second one was the Received Knowledge of Hospital Patients (RKHP), first designed in 1994 by Leino-kilpi & Vuorenhemio, and included 40 items in six dimensions. Biophysiological (eight items: knowledge about symptoms, examinations, treatment, and complications), functional (eight items: knowledge about daily life, rest, mobility, nutrition, body hygiene, elimination, equipment, and aids), experimental (three items: knowledge about emotions, earlier health, and hospital experiences), ethical (nine items: Knowledge about decision-making, patient’s rights, duties, confidentiality), social (six items: knowledge about social support from relatives, significant others, and patients support groups, etc.), and financial (six items: Knowledge about costs related to rehabilitation, insurance, continuity of care and medication).
The patients were asked to rank each item based on a Likert scale (1=completely agree, 4=completely disagree); a fifth option was also included (0=“Does not apply”) (Montin et al. 2010). The lowest score (40), indicated more received knowledge, and the highest score (160) indicated the lowest knowledge that the patient received.
The reliability of RKHP questionnaire in the study by Klemetti (2014) was estimated 0.89-0.95. In the present study, Cronbach's α coefficient (0.807) was obtained, which was an acceptable and appropriate reliability coefficient. Validity was achieved through content validation by ten qualified professors. The collected data were analyzed by SPSS V. 19 using descriptive and inferential statistical tests such as mean, standard deviation, and minimum and maximum.
3. Results
Characteristics of the Sample
The demographic characteristics of the patients (Table 1) indicated that most of the subjects were in the age range of 51-65 (81.4%), female (59.3%), housewives (52.9%), married (89.3%), urban residents (92.9%), and with sufficient income and secondary education level and illiterate (43%). The majority of participants in the study were not educated about arthroplasty (80%), had no history of another surgical procedure on the same foot (90%), had no history of other knee arthroplasty (86.6%), and the length of their stay at the hospital was 5-7 days (80.7%).
Knowledge score in six Dimensions
The mean score of total knowledge was (2.09) with SD=0.28. This score was higher than the average score (2) of knowledge, which indicated that the level of knowledge was unacceptable and suggested that patients needed to receive more information. Also, the highest mean (2.46) was in the ethical dimension, which indicated that the knowledge of patients was less in this dimension than the other dimensions, and the lowest mean was in the economic dimension (1.65), which indicated that the knowledge of patients was more in this dimension than the other dimensions (Table 2).
4. Discussion
Research on knowledge of patients undergoing TKR is very limited in Iran and such a study is not conducted so far. In terms of knowledge score and its six dimensions, the knowledge score in the present study was higher than the average, which indicated an inadequate level of knowledge of patients. Patients received the highest score in the financial aspect, and the lowest score in the ethical dimension.
A study on patients undergoing TKA showed that the mean score for all dimensions of knowledge was 1.62. Maximum knowledge was received in the biophysiological dimension with a mean of 1.36, and the minimum knowledge was received in the financial dimension with a mean of 2.24 (P=0.001). In this study, the knowledge score was lower than the average, which showed an acceptable level of received knowledge in patients, while in the current study, this score was more than the average level, which is not consistent with the present study (Montin et al. 2010).
A study which examined six dimensions of knowledge (bio physiological, functional, experimental, ethical, social, and financial) showed that adequate education of patients empowers their self-care. In this study, the minimum difference was observed in functional (3.358) and bio physiological dimensions (3.361).
In these two functional and biophysiological dimensions, the score of knowledge was higher than the average, and patients had the lowest received knowledge. In the present study, patients in the ethical dimension including: knowledge about decision-making, patient’s rights, duties, and confidentiality, had the least received knowledge score. It means that they needed to receive more knowledge in this dimension and the result was not consistent with those of the present study. It may be due to the high number of samples of that research as well as the longer period of sampling (Klemetti et al. 2015) .
Knowledge of patients about self-care is strongly emphasized in many studies. The study by Chen et al. (2014) showed that patient education before TKR surgery, increased post-surgical knowledge, and pain relief, and improved function of patients (Chen et al. 2014). Firooz et al. (2015) also stated that increasing the knowledge of patients in all respects: physiological, social, emotional, and spiritual was a cost-effective way to reduce the costs of medical care (Firooz et al. 2016). The descriptive study by Sigurdardottir et al. (2015), which was part of a partnership between the countries of north of Europe (Finland, Iceland, Sweden) and the countries of southern Europe (Cyprus, Greece and Spain) and lasted from 2009 to 2011, showed that the knowledge score was 2.72, which was higher than average and showed an unacceptable received knowledge in such patients (Sigurdardottir et al. 2015). In the present study, this score was more than average, indicating unacceptable received knowledge in patients, consistent with that study.
Patient education is the most important goal and task of nursing staff. In fact, it has many positive effects such as increasing patient satisfaction, improving quality of life, reducing the complications of disease and the cost of treatment and re-admissions. One of the most important barriers to patient education in Iran is the lack of physical and psychological readiness of the patient, serious nursing shortage, lack of time for education, and lack of effective relationship between patients and nurses (Tahery et al. 2011). The researchers found that patient education is done by giving a pamphlet and a brief description at the patient’s bedside and education of ethical aspects is extensively overlooked.
The current study was conducted to determine the knowledge of individuals undergoing total knee replacement. According to the results, the findings in relation to the knowledge and its six dimensions showed that patients after surgery had the most received knowledge in the financial dimension and the least received knowledge in the ethical dimension. It means that they needed more training. The most received knowledge in other dimensions was experimental, social, functional, and bio physiological, respectively.
The total score of received knowledge was slightly higher than average, indicating an inadequate level of knowledge and awareness of patients. Nursing managers and nursing staff can help to improve the level of knowledge of such patients by planning and executing regular educational programs and consequently provide more chance to improve self-care of such patients.
Ethical Considerations
Compliance with ethical guidelines
Permission to conduct the study was obtained from Iran University of Medical Sciences. Patients were informed about the purpose of the study and all the data were collected and handled anonymously. A written informed consent was obtained from all participants. The approval was based on national standard. To use of RKHP, permission was given by all copyright holders.
Funding
The current study was part of MSc. thesis of the first author in Department of Nursing, Faculty of Nursing and Midwifery, Iran University of Medical Sciences. This article was supported by Iran University of Medical Sciences.
Authors' contributions
All authors contributed in designing, running, and writing all parts of the research.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors appreciate Iran University of Medical Sciences for its financial support. Authors wish to thank all the patients and their families that assigned their time to complete the questionnaire, also the managers of the hospitals and clinics, nurses, and orthopedic clinicians who collaborated and contributed to conduct this study.
References
Bonnin, M., et al., 2010. Can patients really do sport after TKA?. Knee Surgery, Sports Traumatology, Arthroscopy, 18(7), pp. 853-62. [DOI:10.1007/s00167-009-1009-4]
Chen, S. R., Chen, C. S. & Lin, P. C., 2014. The effect of educational intervention on the pain and rehabilitation performance of patients who undergo a total knee replacement. Journal of Clinical Nursing, 23(1-2), pp. 279-87. [DOI:10.1111/jocn.12466]
Farahani, M. A., et al., 2013. Factors influencing the patient education: A qualitative research. Iranian Journal of Nursing and Midwifery Research, 18(2), p. 133.
Farahani, M. A., et al., 2011. Communication barriers to patient education in cardiac inpatient care: A qualitative study of multiple perspectives. International Journal of Nursing Practice, 17(3), pp. 322-8. [DOI:10.1111/j.1440-172X.2011.01940.x]
Firooz, M., et al., 2016. [Comparison between the effect of group education and group counseling on emotional self-care in type II diabetics (Persian)]. Journal of Birjand University of Medical Sciences, 22(4), pp. 54-9.
Ghaeeni, S. & Amirkhani, F. 2015. [The effect of a rehabilitation program with progressive intensity on dynamic growth of lower extremity strength in the elderly with osteoarthritis after total knee arthroplasty (Persian)]. Journal of Sport Medicine, 7(1), pp. 69-84.
Huber, E. O., et al., 2013. Effect of pre-operative neuromuscular training on functional outcome after total knee replacement: a randomized-controlled trial. BMC Musculoskeletal Disorders, 14(1), p. 157. [DOI:10.1186/1471-2474-14-157]
Jafari, M., et al., 2017. [The effect of pilates exercises on pain, outcomes, and quality of life of the patients with total knee replacement (Persian)]. Sadra Medical Sciences Journal, 3(1), pp. 1-12.
Jalali, S., et al., 2015. [Platelet-rich plasma (A new way in Platlet-Rich plasma treatment) for knee osteoarthritis (Persian)]. Medical Journal of Mashhad University of Medical Sciences, 58, pp. 74-9.
Khan, M., et al., 2016. The epidemiology of failure in total knee arthroplasty: avoiding your next revision. The Bone & Joint Journal, 98(1 Supple A), pp. 105-12. [DOI:10.1302/0301-620X.98B1.36293]
Klemetti, S., et al., 2015. Difference between received and expected knowledge of patients undergoing knee or hip replacement in seven European countries. Clinical Nursing Research, 24(6), pp. 624-43. [DOI:10.1177/1054773814549992]
Lewis, S., et al., 2014. Development of a scale to assess performance following primary total knee arthroplasty. Value in Health, 17(4), pp. 350-9. [DOI:10.1016/j.jval.2014.01.006]
Montin, L., et al., 2010. Total joint arthroplasty patients’ perception of received knowledge of care. Orthopaedic Nursing, 29(4), pp. 246-53. [DOI:10.1097/NOR.0b013e3181e51868]
Motififard, M. & Amirkhani, F. M., 2012. [Effects of total knee replacement on quality of life in 60-70 year-old patients with advanced knee osteoarthritis (Persian)]. Journal of Isfahan Medical School, 29(169), 2591-8.
Pozzi, F., Snyder-Mackler, L. & Zeni, J., 2013. Physical exercise after knee arthroplasty: A systematic review of controlled trials. European Journal of Physical and Rehabilitation Medicine, 49(6), p. 877-92. [PMID] [PMCID]
Sigurdardottir, A. K., et al., 2015. Fulfilment of knowledge expectations among family members of patients undergoing arthroplasty: A European perspective. Scandinavian Journal of Caring Sciences, 29(4), pp. 615-24. [DOI:10.1111/scs.12199]
Tahery, N. R. Z. M., et al., 2011. [Importance of patient education according Abadan nursing students’ opinions (Persian)]. Modern Care Journal, 8(2), 100-6.
Tehrani Banihashemi, A., et al., 2014. Prevalence of osteoarthritis in rural areas of I ran: a WHO-ILAR COPCORD study. International Journal of Rheumatic Diseases, 17(4), pp. 384-8. [DOI:10.1111/1756-185X.12312]
Thomsen, et al., 2016. Does knee awareness differ between different knee arthroplasty prostheses? A matched, case-control, cross-sectional study. BMC Musculoskeletal Disorders, 17, p. 141. [DOI:10.1186/s12891-016-1001-3]
In these two functional and biophysiological dimensions, the score of knowledge was higher than the average, and patients had the lowest received knowledge. In the present study, patients in the ethical dimension including: knowledge about decision-making, patient’s rights, duties, and confidentiality, had the least received knowledge score. It means that they needed to receive more knowledge in this dimension and the result was not consistent with those of the present study. It may be due to the high number of samples of that research as well as the longer period of sampling (Klemetti et al. 2015) .
Knowledge of patients about self-care is strongly emphasized in many studies. The study by Chen et al. (2014) showed that patient education before TKR surgery, increased post-surgical knowledge, and pain relief, and improved function of patients (Chen et al. 2014). Firooz et al. (2015) also stated that increasing the knowledge of patients in all respects: physiological, social, emotional, and spiritual was a cost-effective way to reduce the costs of medical care (Firooz et al. 2016). The descriptive study by Sigurdardottir et al. (2015), which was part of a partnership between the countries of north of Europe (Finland, Iceland, Sweden) and the countries of southern Europe (Cyprus, Greece and Spain) and lasted from 2009 to 2011, showed that the knowledge score was 2.72, which was higher than average and showed an unacceptable received knowledge in such patients (Sigurdardottir et al. 2015). In the present study, this score was more than average, indicating unacceptable received knowledge in patients, consistent with that study.
Patient education is the most important goal and task of nursing staff. In fact, it has many positive effects such as increasing patient satisfaction, improving quality of life, reducing the complications of disease and the cost of treatment and re-admissions. One of the most important barriers to patient education in Iran is the lack of physical and psychological readiness of the patient, serious nursing shortage, lack of time for education, and lack of effective relationship between patients and nurses (Tahery et al. 2011). The researchers found that patient education is done by giving a pamphlet and a brief description at the patient’s bedside and education of ethical aspects is extensively overlooked.
The current study was conducted to determine the knowledge of individuals undergoing total knee replacement. According to the results, the findings in relation to the knowledge and its six dimensions showed that patients after surgery had the most received knowledge in the financial dimension and the least received knowledge in the ethical dimension. It means that they needed more training. The most received knowledge in other dimensions was experimental, social, functional, and bio physiological, respectively.
The total score of received knowledge was slightly higher than average, indicating an inadequate level of knowledge and awareness of patients. Nursing managers and nursing staff can help to improve the level of knowledge of such patients by planning and executing regular educational programs and consequently provide more chance to improve self-care of such patients.
Ethical Considerations
Compliance with ethical guidelines
Permission to conduct the study was obtained from Iran University of Medical Sciences. Patients were informed about the purpose of the study and all the data were collected and handled anonymously. A written informed consent was obtained from all participants. The approval was based on national standard. To use of RKHP, permission was given by all copyright holders.
Funding
The current study was part of MSc. thesis of the first author in Department of Nursing, Faculty of Nursing and Midwifery, Iran University of Medical Sciences. This article was supported by Iran University of Medical Sciences.
Authors' contributions
All authors contributed in designing, running, and writing all parts of the research.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors appreciate Iran University of Medical Sciences for its financial support. Authors wish to thank all the patients and their families that assigned their time to complete the questionnaire, also the managers of the hospitals and clinics, nurses, and orthopedic clinicians who collaborated and contributed to conduct this study.
References
Bonnin, M., et al., 2010. Can patients really do sport after TKA?. Knee Surgery, Sports Traumatology, Arthroscopy, 18(7), pp. 853-62. [DOI:10.1007/s00167-009-1009-4]
Chen, S. R., Chen, C. S. & Lin, P. C., 2014. The effect of educational intervention on the pain and rehabilitation performance of patients who undergo a total knee replacement. Journal of Clinical Nursing, 23(1-2), pp. 279-87. [DOI:10.1111/jocn.12466]
Farahani, M. A., et al., 2013. Factors influencing the patient education: A qualitative research. Iranian Journal of Nursing and Midwifery Research, 18(2), p. 133.
Farahani, M. A., et al., 2011. Communication barriers to patient education in cardiac inpatient care: A qualitative study of multiple perspectives. International Journal of Nursing Practice, 17(3), pp. 322-8. [DOI:10.1111/j.1440-172X.2011.01940.x]
Firooz, M., et al., 2016. [Comparison between the effect of group education and group counseling on emotional self-care in type II diabetics (Persian)]. Journal of Birjand University of Medical Sciences, 22(4), pp. 54-9.
Ghaeeni, S. & Amirkhani, F. 2015. [The effect of a rehabilitation program with progressive intensity on dynamic growth of lower extremity strength in the elderly with osteoarthritis after total knee arthroplasty (Persian)]. Journal of Sport Medicine, 7(1), pp. 69-84.
Huber, E. O., et al., 2013. Effect of pre-operative neuromuscular training on functional outcome after total knee replacement: a randomized-controlled trial. BMC Musculoskeletal Disorders, 14(1), p. 157. [DOI:10.1186/1471-2474-14-157]
Jafari, M., et al., 2017. [The effect of pilates exercises on pain, outcomes, and quality of life of the patients with total knee replacement (Persian)]. Sadra Medical Sciences Journal, 3(1), pp. 1-12.
Jalali, S., et al., 2015. [Platelet-rich plasma (A new way in Platlet-Rich plasma treatment) for knee osteoarthritis (Persian)]. Medical Journal of Mashhad University of Medical Sciences, 58, pp. 74-9.
Khan, M., et al., 2016. The epidemiology of failure in total knee arthroplasty: avoiding your next revision. The Bone & Joint Journal, 98(1 Supple A), pp. 105-12. [DOI:10.1302/0301-620X.98B1.36293]
Klemetti, S., et al., 2015. Difference between received and expected knowledge of patients undergoing knee or hip replacement in seven European countries. Clinical Nursing Research, 24(6), pp. 624-43. [DOI:10.1177/1054773814549992]
Lewis, S., et al., 2014. Development of a scale to assess performance following primary total knee arthroplasty. Value in Health, 17(4), pp. 350-9. [DOI:10.1016/j.jval.2014.01.006]
Montin, L., et al., 2010. Total joint arthroplasty patients’ perception of received knowledge of care. Orthopaedic Nursing, 29(4), pp. 246-53. [DOI:10.1097/NOR.0b013e3181e51868]
Motififard, M. & Amirkhani, F. M., 2012. [Effects of total knee replacement on quality of life in 60-70 year-old patients with advanced knee osteoarthritis (Persian)]. Journal of Isfahan Medical School, 29(169), 2591-8.
Pozzi, F., Snyder-Mackler, L. & Zeni, J., 2013. Physical exercise after knee arthroplasty: A systematic review of controlled trials. European Journal of Physical and Rehabilitation Medicine, 49(6), p. 877-92. [PMID] [PMCID]
Sigurdardottir, A. K., et al., 2015. Fulfilment of knowledge expectations among family members of patients undergoing arthroplasty: A European perspective. Scandinavian Journal of Caring Sciences, 29(4), pp. 615-24. [DOI:10.1111/scs.12199]
Tahery, N. R. Z. M., et al., 2011. [Importance of patient education according Abadan nursing students’ opinions (Persian)]. Modern Care Journal, 8(2), 100-6.
Tehrani Banihashemi, A., et al., 2014. Prevalence of osteoarthritis in rural areas of I ran: a WHO-ILAR COPCORD study. International Journal of Rheumatic Diseases, 17(4), pp. 384-8. [DOI:10.1111/1756-185X.12312]
Thomsen, et al., 2016. Does knee awareness differ between different knee arthroplasty prostheses? A matched, case-control, cross-sectional study. BMC Musculoskeletal Disorders, 17, p. 141. [DOI:10.1186/s12891-016-1001-3]
Type of Study: Research |
Subject:
Special
Received: 2018/05/12 | Accepted: 2018/09/24 | Published: 2018/11/1
Received: 2018/05/12 | Accepted: 2018/09/24 | Published: 2018/11/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
