Thu, Aug 15, 2024
[Archive]
Volume 10, Issue 2 (Spring 2024)
JCCNC 2024, 10(2): 113-124 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Taheri H, Kheirkhah M, Ghobadi A, Eshraghi N, Haghani S. The Effect of Vitamin C Cream on Pregnancy Striae in Primiparous Women: A Randomized Controlled Clinical Trial. JCCNC 2024; 10 (2) :113-124
URL: http://jccnc.iums.ac.ir/article-1-502-en.html
URL: http://jccnc.iums.ac.ir/article-1-502-en.html



1- Department of Midwifery Education, School of Nursing and Midwifery, Iran University of Medical Sciences, Tehran, Iran.
2- Nursing and Midwifery Care Research Center, School of Nursing and Midwifery, Iran University of Medical Sciences, Tehran, Iran. ,shivakheirkhah1345@gmail.com
3- Department of Traditional Medicine, School of Persian Medicine, Iran University of Medical Sciences, Tehran, Iran.
4- Shahid Akbarabadi Clinical Research Development Unit (ShACRDU), School of Medicine, Iran University of Medical Sciences, Tehran, Iran.
5- Nursing and Midwifery Care Research Center, School of Nursing and Midwifery, Iran University of Medical Sciences, Tehran, Iran.
2- Nursing and Midwifery Care Research Center, School of Nursing and Midwifery, Iran University of Medical Sciences, Tehran, Iran. ,
3- Department of Traditional Medicine, School of Persian Medicine, Iran University of Medical Sciences, Tehran, Iran.
4- Shahid Akbarabadi Clinical Research Development Unit (ShACRDU), School of Medicine, Iran University of Medical Sciences, Tehran, Iran.
5- Nursing and Midwifery Care Research Center, School of Nursing and Midwifery, Iran University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 769 kb]
(147 Downloads)
| Abstract (HTML) (502 Views)
• Pregnancy striae are the most common connective tissue changes during pregnancy. They affect primiparous and multiparous women of any race.
• Striae are not medically dangerous for the mother or the fetus. However, these changes can cause psychological distress in women and lead to undesirable maternal and neonatal outcomes.
• Vitamin C cream effectively reduces the occurrence and severity of pregnancy striae.
• Vitamin C cream can serve as an effective, cost-effective, safe, and acceptable intervention for pregnant women in the prevention of pregnancy striae.
• Striae are not medically dangerous for the mother or the fetus. However, these changes can cause psychological distress in women and lead to undesirable maternal and neonatal outcomes.
• Vitamin C cream effectively reduces the occurrence and severity of pregnancy striae.
• Vitamin C cream can serve as an effective, cost-effective, safe, and acceptable intervention for pregnant women in the prevention of pregnancy striae.
Plain Language Summary
Pregnancy is a crucial and sensitive stage in a woman’s life, with a direct impact on both maternal and fetal health. Pregnancy brings significant changes, one of the most common of which is pregnancy striae. This condition is often perceived as a cosmetic concern but can lead to psychological burdens for the affected women. So far, the effect of local treatment with vitamin creams on this condition has not been investigated. The results of this study confirm the effectiveness of vitamin C cream in reducing the occurrence and severity of pregnancy striae.
Full-Text: (40 Views)
Introduction
Pregnancy is a critical and sensitive stage in women’s lives and is of great importance due to the direct effect on the health of the mother and fetus (Slade et al., 2019). Pregnancy brings about significant changes, one of which is the physiological changes of the skin (Tabaee et al., 2017; Rodrigues et al., 2020). Pregnancy striae are the most common connective tissue changes that occur during pregnancy. Gestational striae commonly occur in the third trimester and can affect primiparous and multiparous women of any race (Brennan et al., 2020). Striae can occur in various physiological and pathological conditions. It is commonly observed on women’s abdomen, thighs, and breasts (Kamrani et al., 2015). Striae appear as reddish or purple streaks, remain like shiny silver lines on the skin, and are seen as folds on the surface. The length of these pregnancy striae lines is up to several centimeters, and their width varies from 1 to 10 mm (Taavoni et al., 2011). These stretch marks are observed in 50%-90% of pregnant women before 24 weeks of pregnancy (Taavoni et al., 2010; Kamrani et al., 2015; Brennan et al., 2016). The estimated prevalence of these skin changes ranges from 50% to 90% in the general population (Liu et al., 2018) and is estimated to be 87.7% among Iranian pregnant women (Soltanipour et al., 2012; Gaber et al., 2021). Some women accept these marks as a natural part of pregnancy. The exact cause of striae is still unknown (Kocaöz et al., 2014). However, genetic and hormonal factors and increased mechanical pressure are believed to play a significant role in their development (Hocaoglu et al., 2020). striae can also develop after sudden weight gain, certain endocrine conditions, and long-term exposure to steroids (Tabaee et al., 2017; Moloudi Mones et al., 2014).
The mother’s age, body mass index (BMI), weight gain during pregnancy, abdominal diameter, baby weight, family history of pregnancy striae, and quality of nutrition, including consumption of liquids, fruits, and vegetables, also influence the severity of pregnancy striae (Al Niaimi & Chiang, 2017; Ren et al., 2019). Although these physiological changes are not medically dangerous for the mother or the fetus, they can cause emotional distress in women and lead to adverse maternal and newborn outcomes depending on different cultures. These outcomes may include psychological issues and negative body image perception, negative impact on sexual response and quality of life, development of wounds in the affected areas due to itching, formation of itchy papules and plaques, chronic stress and anxiety in the mother, and creating problems in infant’s temperament (Austin et al., 2005; Khalid et al., 2021). These changes cause many primiparous women or women intending to become pregnant to inquire about the factors that contribute to this condition and the methods of its prevention and treatment (Kamrani et al., 2015). They are willing to pay exorbitant costs for its treatment (Taavoni et al., 2012). Interventions for striae are focused on prevention and treatment. During pregnancy, the emphasis is on preventing or reducing their severity.
Nowadays, various methods are available to prevent the occurrence of striae and treat existing ones (Osman et al., 2007). These methods include regular exercise, maintaining a healthy diet, staying hydrated by drinking adequate water, using a wide range of cosmetics and health products, and utilizing therapeutic approaches such as microdermabrasion and microneedling. However, it should be noted that some of these methods, such as microdermabrasion and microneedling, can be costly and may not be accessible to everyone in the community (Wollina & Goldman, 2017). A study showed a significant relationship between the presence of striae and blood levels of vitamin C (Findik et al., 2011). A review study showed limited evidence that Centella and possibly massage with bitter almond oil may prevent striae gravidarum (SG) and or reduce their severity. There is also weak evidence that hyaluronic acid prevents SG. Tretinoin holds promise for reducing the severity of new-onset SG, but its use is limited by its pregnancy category. Also, cocoa butter and olive oil are not effective in preventing SG or reducing the severity of the lesions (Korgavkar & Wang, 2015; Osman et al., 2008).
Some studies have suggested the potential effect of certain vitamins, including vitamin C, on the development of striae. Vitamin C, also known as ascorbic acid or ascorbate, is a water-soluble vitamin and has a structural composition of a 6-carbon lactone (Sheldon et al., 2001). Additionally, this vitamin acts as an antioxidant and rejuvenating agent, but it oxidizes rapidly when exposed to air (Conningham et al., 2022). It is an essential element in the diet of humans and many animals, and its deficiency can lead to scurvy and the non-healing of wounds. The skin contains a high concentration of vitamin C (ranging from 0.4 to 1 mg/100 g of wet tissue weight), primarily concentrated in the intracellular compartments. Blood vessels transport it to the skin layer (Dattola et al., 2020). The recommended daily vitamin C intake during pregnancy is 80 to 85 mg, approximately 20% higher than the requirement during non-pregnancy (Conningham et al., 2022; Newman, 2004; Sauermann & Jaspers, 2004).
Unlike plants and some animals, humans cannot produce it due to the absence of the enzyme L-gulono gamma lactone oxidase. Unlike the high doses of vitamin C supplements, only its small fraction is biologically present and active in the skin. Vitamin C, one of the strongest antioxidants, protects the skin against aging, light, immune system suppression caused by ultraviolet (UV) rays, and carcinogenesis (Abdolbaqiyan et al., 2020). This vitamin reduces the formation of melanin and pigments and affects wound healing (Al Niaimi & Chiang, 2017). Vitamin C prevents the activation of proteinase-1 and reduces the production of matrix metalloproteinase (an enzyme degrading collagen), inhibiting the biological synthesis of elastin (Conningham et al., 2020; Al Niaimi & Chiang, 2017). In animal studies, applying 5% ascorbic acid 2 hours before UV ray exposure reduces skin wrinkles (Conningham et al., 2020; Al Niaimi & Chiang, 2017). Clinical studies on the effects of various formulations of topical vitamin C on human skin are still limited and require further investigation (Al Niaimi & Chiang, 2017).
Considering what was discussed, conflicting results about the effectiveness of interventions, limited studies on the effect of vitamin C, the prevalence of this condition, and the high costs of cosmetic products and medical treatments, investigating the impact of vitamin C cream on pregnancy striae seems necessary. This study would be a step towards improving the quality of life for pregnant mothers during pregnancy and, consequently, benefiting families and society. Therefore, the present study was designed and conducted to determine the effect of vitamin C cream on pregnancy striae in primiparous women.
Materials and Methods
Design, setting, and sample
This study is a triple-blinded, randomized controlled trial. The research population consisted of primiparous women with a gestational age of 18-20 weeks who were referred to Shahid Akbarabadi Hospital in Tehran, Iran, from July 20, 2022, to January 20, 2023. Shahid Akbarabadi Educational and Therapeutic Center is a referral center for mothers in south Tehran Province. The Equation 1 was used to determine the minimum required sample size at a 95% confidence level and 80% test power, assuming a 6-unit difference between the intervention and control groups is considered statistically significant (Abbas et al., 2020). As a result, a sample size of 24 was calculated for each group, and considering a potential 20% attrition rate, the estimated sample size for each group was 30.

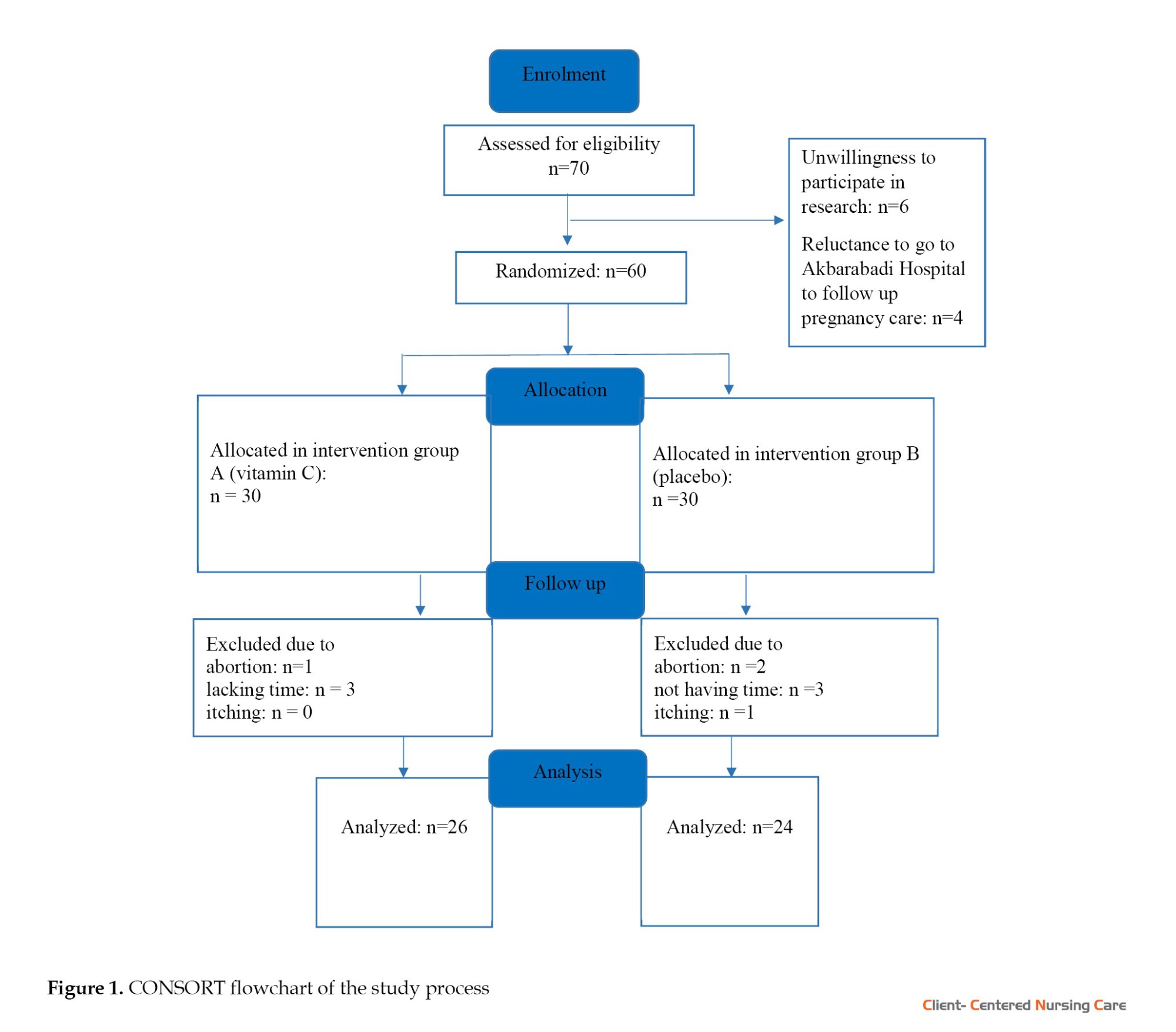
First, the subjects were selected using continuous sampling based on the inclusion criteria. The allocation of samples into groups was done using the random block allocation method. Initially, the two study groups were assigned the labels A and B. Then, the samples were allocated to the two groups using Envelope Randomization Software (ERS) online, with random block allocation of 4 and 8, based on a pre-prepared list. Concealment was achieved using the code the Sealed Envelope website provided on pre-prepared and sealed envelopes. According to the list, 30 participants were in each intervention and placebo group. In the vitamin C group, one person was excluded from the study due to abortion, three people were excluded due to lack of time, and finally, 26 people remained in the intervention group. In the placebo group, two people were excluded from the study due to abortion, three people due to lack of time, and one person due to itching, and finally, the sample size in this group reached 24 people (Figure 1).
The inclusion criteria for the study were as follows: Healthy primiparous women willing to participate in the study, aged between 20 and 40 years in the 6th to 20th week of pregnancy, BMI before the intervention in the range of 18.5 to 25 kg/m2, having a minimum level of literacy, lacking a history of skin diseases before the occurrence of stretch marks, and not having a history of allergy to vitamin C. The exclusion criteria were as follows: Having a systemic disease or a known medical condition (such as gestational diabetes, preeclampsia, adrenal gland disorder, or Cushing disease) during the study, multiple pregnancies, maternal polyhydramnios, and diagnosis of fetal macrosomia. Other exclusion criteria were using other drugs for the prevention or treatment of striae during the study, unwillingness to continue taking the drug, experiencing side effects such as itching, burning, and redness caused by the drug during the study, not following the correct use of the drug (including dosage, frequency, and instructions for use) and concomitant use of medications that may interact with vitamin C (such as corticosteroids and anticoagulants) during the study.
Study instruments
The data were collected by a demographic questionnaire and the Atwal SG scorecard. The demographic questionnaire was developed based on a thorough review of reputable and recent literature, as well as guidance from expert professors, and included age, education, economic status, BMI, history of abortion, history of striae in first-degree relatives, and skin color. The researcher observed and recorded the number and severity of striae erythema using the Atwal SG scorecard. The maximum score for each area (abdomen, breasts, thighs, and buttocks) was set at 6 (0 to 3 for the number of striae and 0 to 3 for erythema severity). In each area, a score of 0 was given if no striae were present. For less than 5 striae, a score of 1 was assigned. For 5 to 10 striae, a score of 2 was given, and for more than 10 striae, a score of 3 was assigned. For the absence of erythema, a score of 0 was given. For mild erythema (light red or pink), a score of 1 was assigned. For marked erythema (dark red), a score of 2 was given; for intense erythema (purple), a score of 3 was assigned. The total score ranged from 0 to 3, indicating no striae or negligible striae, from 4 to 9, indicating mild striae, and from 10 to 15, indicating moderate striae. Finally, scores above 16 indicate severe striae. These two scores were then summed up to obtain the overall score. Based on this, the total striae score ranged from 0 to 24 for all body parts. Women were divided into the following four groups: Scores of 0-3 indicating no signs of pregnancy striae, scores of 4-9 indicating mild striae, scores of 10-15 indicating moderate striae, and scores above 16 indicating severe striae (Atwal et al., 2006).
The validity of the Atwal SG score has been confirmed by Atwal et al. (2006). The validity of both tools was also confirmed by 7 faculty members at Iran University of Medical Sciences (IUMS). Inter-rater reliability was utilized to assess the reliability of the Atwal SG scorecard. In this manner, the status, number, and severity of pregnancy-related striae were independently examined and recorded by the researcher and a midwifery expert in 10 participants. The correlation between the results was determined, and ultimately, an intra-class correlation coefficient value of 1 was obtained for all the areas, indicating a perfect agreement.
Study intervention
The primiparous mothers were enrolled in the study at weeks 18-20 of gestation and were followed up for 4 months during their pregnancy (at 4, 8, 12, and 16 weeks after the initiation of the intervention). The sampling for this study was done in six months, from July 20, 2022, to January 20, 2023. The pregnant women were provided with necessary explanations regarding the implementation of the research, and it was mentioned that they may be randomly assigned to either the intervention or placebo groups. The questionnaire on personal characteristics, BMI, and gestational age was completed at the beginning of the study. Then, pregnant women who met the research criteria were placed into either the vitamin C cream group or the placebo group based on a predetermined table after completing the demographic information form. These creams were prepared at the researcher’s request and in collaboration with a consultant pharmacist from the Faculty of Traditional Medicine at Iran University of Medical Sciences. The creams of both groups had similar packaging and appearance, and they shared the same color and smell. Concealment was also performed based on the code provided by the sealed envelope website, and the creams were divided into two groups: Group A and group B. The vitamin C cream contained 3% topical vitamin C in 100 g of Oraand base cream, including alco-acetyl, glycerin, triethanolamine, monostarch acid, white vaseline, and distilled water. The placebo cream, on the other hand, was composed of the Oraand base cream without any active ingredients.
The participants of both groups were provided with detailed recommendations on the correct use of the creams. They were advised to apply a thin layer of creams twice a day at 12-hour intervals topically with their fingers, gently and without massaging for 4 months. The subjects were instructed not to wash off the cream until fully absorbed. Furthermore, the researcher provided face-to-face instructions to women on correctly completing the daily checklists during their first visit. Before the intervention, the researcher observed and recorded the number and severity of striae using the Atwal scorecard. After each use, the women were asked to record the daily application of the creams on the checklists. The researcher used the Atwal scorecard to assess the number and severity of pregnancy-induced striae at 4, 8, 12, and 16 weeks after the initiation of the intervention. The researcher visited the research samples at the Perinatology Clinic of Shahid Akbarabadi Center at different follow-up times. During each visit, the researcher examined the usage of each cream by the subjects. The examination times of the samples were matched with their scheduled visits for pregnancy care. Additionally, due to the impact of weight on striae, the patient’s weight was measured at each stage. The researcher maintained weekly communication with the research samples through phone calls or messages to ensure the proper use of creams, completion of the checklists, and to stay informed about potential side effects such as itching and redness. The subjects were requested in advance to inform the researcher if they experienced any side effects. The sampling process continued until the completion of the final sample size, taking into account the possibility of sample attrition in both groups. At the end of the study, the researcher recorded the BMI and gestational age of the women and documented the occurrence and severity of pregnancy striae.
Blinding
This study was a triple-blinded, randomized controlled trial. The analyst, the researcher, and the samples were unaware of the groups. The samples were unaware whether they were assigned to the intervention or control group. Both groups received creams. Neither the researcher nor the samples were aware of the contents of the creams, as they had identical packaging, appearance, color, and smell, and there were no differences in the shape and color of the creams.
Data analysis
The data were analyzed using descriptive statistics (relative frequency and Mean±SD). Since the Kolmogorov-Smirnov test showed that the data distribution was not normal, the non-parametric Mann-Whitney U test was used to compare the incidence of striae. Also, the chi-square test was used to compare the education and midwifery characteristics; the Fisher exact test was used to compare the economic status, and the independent t-test was used to compare the age and BMI between the two groups. SPSS software, version 16, was used to analyze the data, and the significance level was set at P<0.05.
Results
Most of the subjects in the vitamin C group were 35-40 years old, while in the placebo group, the age range was 30-35 years. After the intervention, their BMI ranged between 25 and 29.9 (Table 1). There was no significant difference between the groups in terms of age, education level, economic status, and BMI (P>0.05) (Table 1).

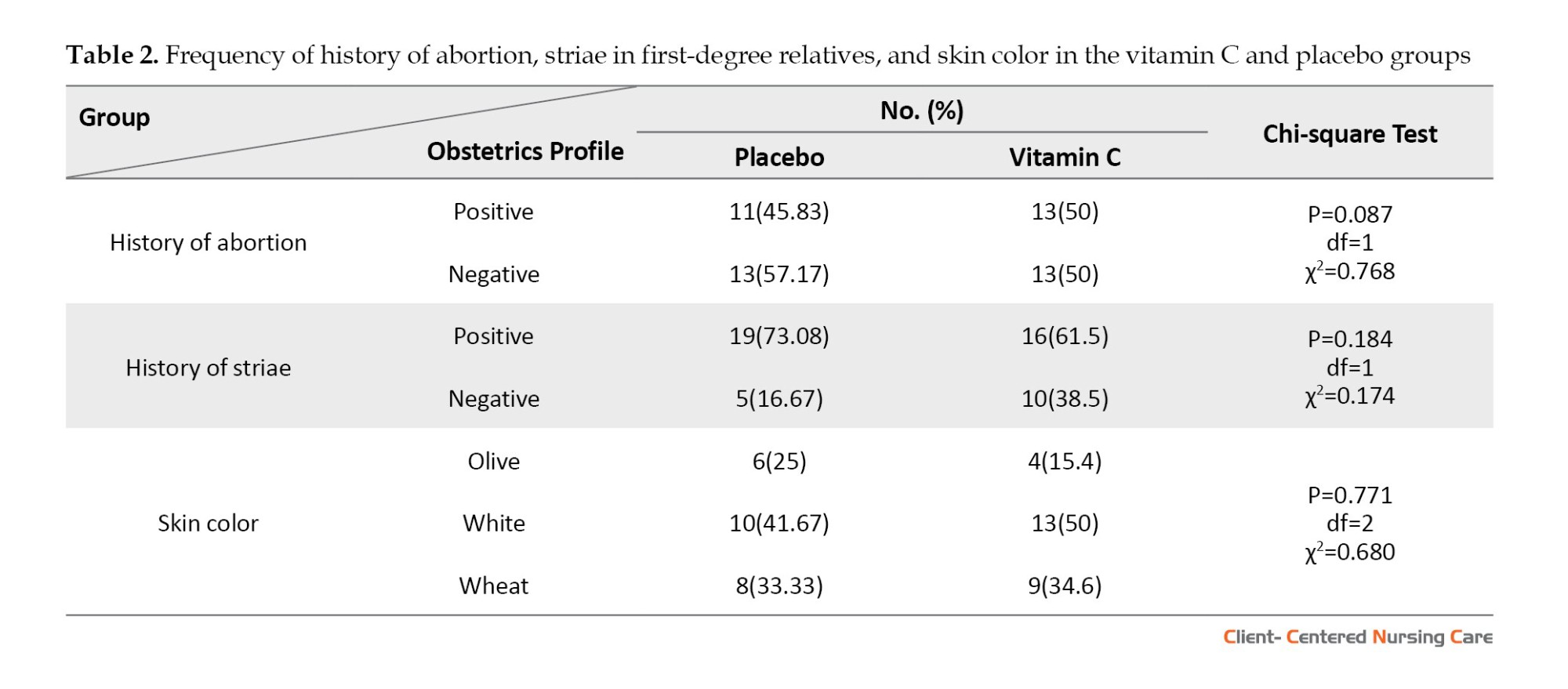
There was no significant difference between the skin color, history of abortion, and history of striae in first-degree relatives of the two groups (P>0.05) (Table 2).
As Table 3 shows, there is a significant difference between the occurrence of pregnancy striae between the two groups at weeks 4 (P=0.012), 8 (P=0.004), 12 (P=0.001), and 16 (P<0.001) after the intervention.

Discussion
This study was conducted to determine the effect of vitamin C cream on pregnancy striae in primiparous women. The results showed a significant difference between the group using vitamin C and the placebo group in terms of the incidence of pregnancy striae. Although research conducted in this field is limited and scarce, and vitamin C has not been specifically used in this regard, a study by Abdolbaghiyan et al. (2020) entitled “expression changes of collagen І and ІІІ genes in human skin fibroblast cells due to microalgae extract Chlorella vulgaris and its comparison with vitamin C” conducted at the National Center of Genetic and Biological Resources of Iran, demonstrated that the algae extract and vitamin C have increased the expression of collagen type І by 3.14-fold and 1.42-fold, respectively. The C. vulgaris algae extract had a greater effect on the collagen type І gene expression. In comparison, vitamin C had a greater impact on increasing the expression of collagen type ІІІ gene, leading to a 2.12-fold increase in its expression. Finally, the findings indicated that C. vulgaris algae extract and vitamin C stimulate collagen synthesis in fibroblast cells, suggesting their potential as suitable alternatives to harmful chemicals used for collagen production in the skin (Abdolbaghiyan et al., 2020). These results align with the present study’s findings regarding the use of vitamin C in the collagen production process and its ultimate impact on pregnancy striae.
The results of a study by Hernández et al. (2013) to evaluate the effectiveness of an anti-crack cream (cream containing hydroxyprolisilane C, rosemary oil, Centella asiatica triterpenes, and vitamin E) in the prevention of SG, show that the use of the anti-crack skin product is effective in reducing the severity of striae during pregnancy. It effectively prevented the formation of new striae and halted the progression of existing ones. The result of this study is consistent with the findings of the present research regarding the use of topical compounds for pregnancy striae. It should be noted that C. asiatica extract contains vitamin C, and considering the effect of this vitamin on collagen production and its role in the skin, this compatibility can be considered. However, it cannot be fully expressed since vitamin C has not been used alone in this context (Hernández et al., 2013).
In 2018, Hajhashemi et al. conducted a study to evaluate the effectiveness of aloe vera gel and sweet almond oil on pregnancy striae in primiparous women. The findings demonstrated that the creams containing aloe vera and sweet almond oil had a greater impact on reducing striae erythema than base cream. These creams also reduced itching and prevented the progression of striae (P<0.001). The results of this study are consistent with the findings of the present research regarding the use of topical compounds on the severity of pregnancy striae erythema. Additionally, aloe vera gel contains vitamin C, and considering the effect of this vitamin on collagen production and its role in the skin, this correspondence can be significant (Hajhashemi et al., 2018). However, it should be noted that this correspondence cannot be fully accepted, as vitamin C alone was not used in the study.
In 2021, Bagherian et al. conducted a study to investigate the effect of aloe vera gel in preventing pregnancy striae. The study found that the incidence of striae (P=0.001) and the intensity of itching and erythema (P=0.001) in the 28th week of pregnancy were significantly lower in the group using aloe vera gel. This study concluded that due to the presence of vitamin C in aloe vera gel, it could be recommended to pregnant women as a low-cost option for preventing pregnancy striae (Bagherian et al., 2021). Aloe vera gel contains vitamin C, which is consistent with the findings of the present research regarding the use of vitamin C in preventing the occurrence of pregnancy striae. The results of this study confirmed the effectiveness of vitamin C in preventing pregnancy striae in women, and it can be utilized as an effective, affordable, safe, and acceptable intervention for pregnant women to prevent pregnancy striae. A systematic review of the role of vitamins in skin health demonstrated that vitamin C reduces dimer changes and thymine mutations caused by UV radiation, as well as the formation of apoptotic cells resulting from sunburn. These effects potentially reduce the risk of carcinogenesis. Additionally, vitamin C effectively improves skin elasticity, maintains moisture, and enhances the skin’s antioxidant capacity. The role of ascorbic acid in synthesizing collagen and elastin is very important in maintaining skin health. This vitamin is a cofactor for prolyl and lysyl hydroxylases, enzymes that catalyze the formation of hydroxyproline and hydroxylysine. It appears that ascorbate also regulates the transcription of collagen type I and III genes. In vitro studies have shown that fibroblasts stimulated with ascorbic acid exhibit increased collagen gene expression. Oral supplements of this vitamin can reduce the severity of skin spots, improve erythema and texture, and clean skin pores. Vitamin C levels are lower in aged or photodamaged skin, and adequate levels of ascorbic acid can help counteract the adverse effects of UV rays. Aged human skin fibroblasts can increase their proliferative capacity when treated with sufficient levels of ascorbic acid. Vitamin C deficiency is associated with the loss of several skin functions and changes in wound healing (related to the lack of collagen production), thickening of the stratum corneum, and subcutaneous bleeding due to fragility and changes in connective tissue morphology (Dattola et al., 2020). The result of this study is consistent with the findings of this research regarding the effect of vitamin C on collagen production.
Conclusion
This study examined the effect of vitamin C cream on pregnancy striae in primiparous women.
It is suggested that further studies be conducted to investigate the effectiveness of this cream in the treatment of SG, as well as their potential application to other populations, such as women looking to change their weight and athletes concerned about the development of stretch marks. The target audience for the results of this research includes primiparous women, obstetricians/gynecologists, midwives, healthcare providers, and officials and planners responsible for the educational and support programs for pregnant women. Considering that assisting pregnant women is one of the most important goals of midwifery and healthcare, one of these forms of assistance is the prevention and treatment of pregnancy striae. Due to the high prevalence of pregnancy striae and the significant costs associated with cosmetic products and medical treatments, the use of vitamin supplements is highly advantageous. It is necessary to provide sufficient information about striae to pregnant mothers to reduce their anxiety and concerns. It is suggested that further studies be conducted to investigate the effectiveness of these creams in treating SG and their potential application to other populations, such as women looking to change their weight and athletes concerned about the development of stretch marks. In this study, a vitamin C cream was used, and other vitamin creams, such as the combination of vitamin E and C, are recommended in future research to assess their impact on pregnancy striae. Additionally, the effectiveness of this cream should be explicitly investigated in multiparous women.
One of the strengths of this study was the presence of a placebo group, the random assignment of participants to different groups, and the blinding and concealment of the samples. Among the limitations of this research are the impossibility of precise control of the frequency of using the cream by the participants and the insufficient information about the serum levels of vitamin C in the samples.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Iran University of Medical Sciences (IUMS) (Code: IR.IUMS.REC.1401.215). The study proposal was registered in the Iranian Registry of Clinical Trials (IRCT) (Code:: IRCT20220509054799N1). A letter of introduction was obtained from the Faculty of Nursing and Midwifery at IUMS and the Shahid Akbarabadi Educational and Therapeutic Center in Tehran. Informed consent was obtained from all participants.
Funding
This article results from a Master’s thesis in Midwifery Education at Iran University of Medical Sciences (Project No.: 3-1400-3-3-22271). The Research Deputy of Iran University of Medical Sciences financially supported this study.
Authors' contributions
Supervison: Masoomeh Kheirkhah; Conceptualisation: Hadis Taheri and Masoomeh Kheirkhah; Implementation: Hadis Taheri; Sampling and data collection: Hadis Taheri and Nooshin Eshraghi; Data analysis and preparing the initial draft of the manuscript: Hadis Taheri and Shima Haghani; Preparation of creams: Hadis Taheri and Ali Ghobadi; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The research team expresses its great gratitude to the Research Vice-Chancellor of Iran University of Medical Sciences (IUMS). The authors also appreciate the Clinical Research Development Unit of Shahid Akbarabadi Hospital-IUMS for conducting this research.
References
Abbas A, et al., 2020, Atwal striae gravidarum score for prediction of perineal tears during vaginal delivery: A cross sectional study. World Journal of Gynecology & Women’s Health, 4(3), pp. 25-32. [DOI:10.33552/WJGWH.2020.04.000587]
Abdolbaghian, S., et al., 2020, [Gene expression changes of collagen І and ІІІ in human skin fibroblast cells in effect of microalga Chlorella vulgaris extract and compared to vitamin C (Persian). Journal of Marine Biology, 11(44), pp. 1-10. [Link]
Al-Niaimi, F. & Chiang, N. Y. Z., 2017. Topical Vitamin C and the Skin: Mechanisms of action and clinical applications. Journal of Clinical and Aesthetic Dermatology, 10(7), pp. 14-17. [PMID]
Atwal, G. S., et al., 2006. Striae gravidarum in primiparae. The British Journal of Dermatology, 155(5), pp. 965–9. [DOI:10.1111/j.1365-2133.2006.07427.x] [PMID]
Austin MP, et al., 2005, Maternal trait anxiety, depression and life event stress in pregnancy: relationships with infant temperament. Early Hum Dev 81(2):183-90. [DOI:10.1016/j.earlhumdev.2004.07.001] [PMID]
Bagherian, S., et al., 2021. [Effect of Aloe Vera Gel on prevention of Striae Gravidarum (Persian)]. Iranian Journal of Obstetrics, Gynecology and Infertility, 23(11), pp. 41-50. [DOI:10.22038/IJOGI.2021.17619]
Brennan M, et al., 2020, A qualitative study of the factors influencing recruitment to a pilot trial on the prevention of striae gravidarum. BMC Pregnancy and Childbirth, 20(1), pp. 103. [DOI:10.1186/s12884-020-2781-x] [PMID]
Brennan M & Clarke M & Devane D, 2016, The use of anti-stretch marks’ products by women in pregnancy: a descriptive, cross-sectional survey. BMC Pregnancy and Childbirth Sep 21;16(1):276. [DOI:10.1186/s12884-016-1075-9] [PMID]
Conningham, F. G., et al., 2022. Williams Obstetrics 26e. New York: McGraw Hill Medical. [Link]
Dattola A, et al., 2020, Role of Vitamins in Skin Health: A Systematic Review. Current Nutrition Reports, 9(3), pp. 226–35. [DOI:10.1007/s13668-020-00322-4] [PMID]
Findik, R. B, et al., 2011, Striae gravidarum, vitamin C and other related factors. International Journal for Vitamin and Nutrition Research. Internationale Zeitschrift fur Vitamin- und Ernahrungsforschung. Journal International de Vitaminologie et de Nutrition, 81(1), pp. 43–8. [DOI:10.1024/0300-9831/a000049] [PMID]
Gaber, M. & Mohamed Elshafie, A., 2021. The impact of striae gravidarum on quality-of-life issues. The Egyptian Journal of Hospital Medicine, 82(1), pp. 31-6. [DOI:10.21608/ejhm.2021.137550]
García Hernández, J. Á., et al., 2013. Use of a specific anti-stretch mark cream for preventing or reducing the severity of striae gravidarum. Randomized, double-blind, controlled trial. International Journal of Cosmetic Science, 35(3), pp. 233-7. [DOI:10.1111/ics.12029] [PMID]
Hajhashemi, M., et al., 2018. The effect of Aloe vera gel and sweet almond oil on striae gravidarum in nulliparous women. The Journal of Maternal-Fetal & Neonatal Medicine: The Official Journal of the European Association of Perinatal Medicine, The Federation of Asia and Oceania Perinatal Societies, the International Society of Perinatal Obstetricians, 31(13), pp. 1703–8. [DOI:10.1080/14767058.2017.1325865] [PMID]
García Hernández, J. Á., et al., 2013. Use of a specific anti-stretch mark cream for preventing or reducing the severity of striae gravidarum. Randomized, double-blind, controlled trial. International Journal of Cosmetic Science, 35(3), pp. 233–7.[DOI:10.1111/ics.12029] [PMID]
Hocaoglu, E., Hocaoglu, M. & Akdeniz, E., 2020. Association between serum 25-hydroxyvitamin D levels and the presence and severity of striae gravidarum in primigravid women. Journal of Cosmetic Dermatology, 19(11), pp. 3107–14. [DOI:10.1111/jocd.13386] [PMID]
Kamrani A & Malakouti J & Farshbaf Khalili A, 2015, [The effect of sweet almond oil, sesame oil and the combination of sweet almond oil and sesame oil in the prevention of striae pregnancy and the itching caused by it in primiparous women: a randomized controlled clinical trial (Persian)]. Iranian Journal of Obstetrics, Gynecology and Infertility. 18(169);1-11.[DOI: 10.22038/IJOGI.2015.6129]
Khalid El, et al., 2021, Assessment of Quality of Life and Sexual Function in ladies with Pregnancy-Related Skin Changes, The Egyptian Journal of Hospital Medicine 83(1):1105-1112. [DOI:10.21608/ejhm.2021.160881]
Kocaöz S & Gördeles Beşer N & Kizilirmak A. 2019, Striae gravidarum in primigravid women: prevalence, risk factors, prevention interventions and body image. The Journal of Maternal-Fetal & Neonatal Medicine 33(23):1-7. [DOI:10.1080/14767058.2019.1591363] [PMID]
Korgavkar, K. & Wang, F., 2015. Stretch marks during pregnancy: A review of topical prevention. The British Journal of Dermatology, 172(3), pp. 606-15. [DOI:10.1111/bjd.13426] [PMID]
Liu, L., et al., 2018. Risk factors of striae gravidarum in Chinese primiparous women. Plos One, 13(6), pp. e0198720. [DOI:10.1371/journal.pone.0198720] [PMID]
Moloudi Mones, et al., 2014, Evaluation of pregnancy striae and related risk factors in primiparous women referring to Imam Reza (AS) Hospital in Urmia. Journal of Nursing and Midwifery 12(3):207-213. [Link]
Newman WA. 2004, Dorland's medical dictionary [Persian trans] Mohebi, H., Nikfarjam R. Tehran: Golban Medical Publication 803. [Link]
Osman H, et al., 2007, Risk factors for the development of steria gravidarum. A M J Obstet Gynecol 196(1):62.e1-5. [DOI:10.1016/j.ajog.2006.08.044] [PMID]
Osman H, et al., 2008, Cocoa butter lotion for prevention of striae gravidarum: a double-blind, randomised and placebo-controlled trial. BJOG 115(9):1138-42. [DOI:10.1111/j.1471-0528.2008.01796.x] [PMID]
Ren P, et al., 2019, Risk factors for the formation of striae gravidarum in women in Jiangsu Province of China. Taiwan J Obstet Gynecol 58(5):640-644. [DOI:10.1016/j.tjog.2019.07.010] [PMID]
Rodrigues M, et al., 2020, Evaluation of effect of a vitamin-based barrier cream on the clinical severity of actinic cheilitis: A preliminary study. Oral Medicine and Pathology 12(10): 944-50. [DOI:10.4317/jced.57013] [PMID]
Sauermann, K., et al., 2004. Topically applied vitamin C increases the density of dermal papillae in aged human skin. BMC Dermatology, 4(1), pp. 13. [DOI:10.1186/1471-5945-4-13] [PMID]
Seirafianpour, F., et al., 2021. Systematic review of single and combined treatments for different types of striae: A comparison of striae treatments. Journal of the European Academy of Dermatology and Venereology: JEADV, 35(11), pp. 2185–98. [DOI:10.1111/jdv.17374] [PMID]
Sheldon R. et al., 2001, Topical L-Ascorbic Acid: Percutaneous Absorption Studies. American Society for Dermatologic Surgery. Dermatol Surg 27(2):137-42. [DOI:10.1046/j.1524-4725.2001.00264.x] [PMID]
Slade, P., et al., 2019. Establishing a valid construct of fear of childbirth: Findings from in-depth interviews with women and midwives. BMC Pregnancy and Childbirth, pp. 19(1), 96.[DOI:10.1186/s12884-019-2241-7] [PMID]
Soltanipour F, et al., 2012, Determining the effect of teak cream on pregnancy striae. Scientific Research Journal of Yasouj University of Medical Sciences, 17(5):379-386. [DOI: 10.1016/j.ctim.2013.11.011] [PMID]
Taavoni, S., et al., 2012. [The effect of olive oil and teak cream on striae of pregnancy in the second trimester of pregnancy (Persian)]. Iranian Journal of Nursing, 25(75), pp. 45-51. [Link]
Taavoni, S., et al., 2010. [A survey on the effects of olive oil on striae gravidarum in the second trimester of pregnancy (Persian)]. Nursing and Midwifery Journal, 8(1), pp. 6-10. [Link]
Taavoni, S., et al., 2011. Effects of olive oil on striae gravidarum in the second trimester of pregnancy. Complementary Therapies in Clinical Practice, 17(3), pp. 167–9. [DOI:10.1016/j.ctcp.2010.10.003] [PMID]
Tabaee, S., et al., 2016. [Investigating the effect of fractional ablative CO2 laser in reducing pregnancy striae in patients with pregnancy striae (Persian)]. Laser in Medicine, 14(1), pp. 2-9. [Link]
Wollina, U. & Goldman, A., 2017. Management of stretch marks (with a focus on striae rubrae). Journal of Cutaneous and Aesthetic Surgery, 10(3), pp. 124-9. [DOI:10.4103/JCAS.JCAS_118_17] [PMID]
Pregnancy is a critical and sensitive stage in women’s lives and is of great importance due to the direct effect on the health of the mother and fetus (Slade et al., 2019). Pregnancy brings about significant changes, one of which is the physiological changes of the skin (Tabaee et al., 2017; Rodrigues et al., 2020). Pregnancy striae are the most common connective tissue changes that occur during pregnancy. Gestational striae commonly occur in the third trimester and can affect primiparous and multiparous women of any race (Brennan et al., 2020). Striae can occur in various physiological and pathological conditions. It is commonly observed on women’s abdomen, thighs, and breasts (Kamrani et al., 2015). Striae appear as reddish or purple streaks, remain like shiny silver lines on the skin, and are seen as folds on the surface. The length of these pregnancy striae lines is up to several centimeters, and their width varies from 1 to 10 mm (Taavoni et al., 2011). These stretch marks are observed in 50%-90% of pregnant women before 24 weeks of pregnancy (Taavoni et al., 2010; Kamrani et al., 2015; Brennan et al., 2016). The estimated prevalence of these skin changes ranges from 50% to 90% in the general population (Liu et al., 2018) and is estimated to be 87.7% among Iranian pregnant women (Soltanipour et al., 2012; Gaber et al., 2021). Some women accept these marks as a natural part of pregnancy. The exact cause of striae is still unknown (Kocaöz et al., 2014). However, genetic and hormonal factors and increased mechanical pressure are believed to play a significant role in their development (Hocaoglu et al., 2020). striae can also develop after sudden weight gain, certain endocrine conditions, and long-term exposure to steroids (Tabaee et al., 2017; Moloudi Mones et al., 2014).
The mother’s age, body mass index (BMI), weight gain during pregnancy, abdominal diameter, baby weight, family history of pregnancy striae, and quality of nutrition, including consumption of liquids, fruits, and vegetables, also influence the severity of pregnancy striae (Al Niaimi & Chiang, 2017; Ren et al., 2019). Although these physiological changes are not medically dangerous for the mother or the fetus, they can cause emotional distress in women and lead to adverse maternal and newborn outcomes depending on different cultures. These outcomes may include psychological issues and negative body image perception, negative impact on sexual response and quality of life, development of wounds in the affected areas due to itching, formation of itchy papules and plaques, chronic stress and anxiety in the mother, and creating problems in infant’s temperament (Austin et al., 2005; Khalid et al., 2021). These changes cause many primiparous women or women intending to become pregnant to inquire about the factors that contribute to this condition and the methods of its prevention and treatment (Kamrani et al., 2015). They are willing to pay exorbitant costs for its treatment (Taavoni et al., 2012). Interventions for striae are focused on prevention and treatment. During pregnancy, the emphasis is on preventing or reducing their severity.
Nowadays, various methods are available to prevent the occurrence of striae and treat existing ones (Osman et al., 2007). These methods include regular exercise, maintaining a healthy diet, staying hydrated by drinking adequate water, using a wide range of cosmetics and health products, and utilizing therapeutic approaches such as microdermabrasion and microneedling. However, it should be noted that some of these methods, such as microdermabrasion and microneedling, can be costly and may not be accessible to everyone in the community (Wollina & Goldman, 2017). A study showed a significant relationship between the presence of striae and blood levels of vitamin C (Findik et al., 2011). A review study showed limited evidence that Centella and possibly massage with bitter almond oil may prevent striae gravidarum (SG) and or reduce their severity. There is also weak evidence that hyaluronic acid prevents SG. Tretinoin holds promise for reducing the severity of new-onset SG, but its use is limited by its pregnancy category. Also, cocoa butter and olive oil are not effective in preventing SG or reducing the severity of the lesions (Korgavkar & Wang, 2015; Osman et al., 2008).
Some studies have suggested the potential effect of certain vitamins, including vitamin C, on the development of striae. Vitamin C, also known as ascorbic acid or ascorbate, is a water-soluble vitamin and has a structural composition of a 6-carbon lactone (Sheldon et al., 2001). Additionally, this vitamin acts as an antioxidant and rejuvenating agent, but it oxidizes rapidly when exposed to air (Conningham et al., 2022). It is an essential element in the diet of humans and many animals, and its deficiency can lead to scurvy and the non-healing of wounds. The skin contains a high concentration of vitamin C (ranging from 0.4 to 1 mg/100 g of wet tissue weight), primarily concentrated in the intracellular compartments. Blood vessels transport it to the skin layer (Dattola et al., 2020). The recommended daily vitamin C intake during pregnancy is 80 to 85 mg, approximately 20% higher than the requirement during non-pregnancy (Conningham et al., 2022; Newman, 2004; Sauermann & Jaspers, 2004).
Unlike plants and some animals, humans cannot produce it due to the absence of the enzyme L-gulono gamma lactone oxidase. Unlike the high doses of vitamin C supplements, only its small fraction is biologically present and active in the skin. Vitamin C, one of the strongest antioxidants, protects the skin against aging, light, immune system suppression caused by ultraviolet (UV) rays, and carcinogenesis (Abdolbaqiyan et al., 2020). This vitamin reduces the formation of melanin and pigments and affects wound healing (Al Niaimi & Chiang, 2017). Vitamin C prevents the activation of proteinase-1 and reduces the production of matrix metalloproteinase (an enzyme degrading collagen), inhibiting the biological synthesis of elastin (Conningham et al., 2020; Al Niaimi & Chiang, 2017). In animal studies, applying 5% ascorbic acid 2 hours before UV ray exposure reduces skin wrinkles (Conningham et al., 2020; Al Niaimi & Chiang, 2017). Clinical studies on the effects of various formulations of topical vitamin C on human skin are still limited and require further investigation (Al Niaimi & Chiang, 2017).
Considering what was discussed, conflicting results about the effectiveness of interventions, limited studies on the effect of vitamin C, the prevalence of this condition, and the high costs of cosmetic products and medical treatments, investigating the impact of vitamin C cream on pregnancy striae seems necessary. This study would be a step towards improving the quality of life for pregnant mothers during pregnancy and, consequently, benefiting families and society. Therefore, the present study was designed and conducted to determine the effect of vitamin C cream on pregnancy striae in primiparous women.
Materials and Methods
Design, setting, and sample
This study is a triple-blinded, randomized controlled trial. The research population consisted of primiparous women with a gestational age of 18-20 weeks who were referred to Shahid Akbarabadi Hospital in Tehran, Iran, from July 20, 2022, to January 20, 2023. Shahid Akbarabadi Educational and Therapeutic Center is a referral center for mothers in south Tehran Province. The Equation 1 was used to determine the minimum required sample size at a 95% confidence level and 80% test power, assuming a 6-unit difference between the intervention and control groups is considered statistically significant (Abbas et al., 2020). As a result, a sample size of 24 was calculated for each group, and considering a potential 20% attrition rate, the estimated sample size for each group was 30.
First, the subjects were selected using continuous sampling based on the inclusion criteria. The allocation of samples into groups was done using the random block allocation method. Initially, the two study groups were assigned the labels A and B. Then, the samples were allocated to the two groups using Envelope Randomization Software (ERS) online, with random block allocation of 4 and 8, based on a pre-prepared list. Concealment was achieved using the code the Sealed Envelope website provided on pre-prepared and sealed envelopes. According to the list, 30 participants were in each intervention and placebo group. In the vitamin C group, one person was excluded from the study due to abortion, three people were excluded due to lack of time, and finally, 26 people remained in the intervention group. In the placebo group, two people were excluded from the study due to abortion, three people due to lack of time, and one person due to itching, and finally, the sample size in this group reached 24 people (Figure 1).
The inclusion criteria for the study were as follows: Healthy primiparous women willing to participate in the study, aged between 20 and 40 years in the 6th to 20th week of pregnancy, BMI before the intervention in the range of 18.5 to 25 kg/m2, having a minimum level of literacy, lacking a history of skin diseases before the occurrence of stretch marks, and not having a history of allergy to vitamin C. The exclusion criteria were as follows: Having a systemic disease or a known medical condition (such as gestational diabetes, preeclampsia, adrenal gland disorder, or Cushing disease) during the study, multiple pregnancies, maternal polyhydramnios, and diagnosis of fetal macrosomia. Other exclusion criteria were using other drugs for the prevention or treatment of striae during the study, unwillingness to continue taking the drug, experiencing side effects such as itching, burning, and redness caused by the drug during the study, not following the correct use of the drug (including dosage, frequency, and instructions for use) and concomitant use of medications that may interact with vitamin C (such as corticosteroids and anticoagulants) during the study.
Study instruments
The data were collected by a demographic questionnaire and the Atwal SG scorecard. The demographic questionnaire was developed based on a thorough review of reputable and recent literature, as well as guidance from expert professors, and included age, education, economic status, BMI, history of abortion, history of striae in first-degree relatives, and skin color. The researcher observed and recorded the number and severity of striae erythema using the Atwal SG scorecard. The maximum score for each area (abdomen, breasts, thighs, and buttocks) was set at 6 (0 to 3 for the number of striae and 0 to 3 for erythema severity). In each area, a score of 0 was given if no striae were present. For less than 5 striae, a score of 1 was assigned. For 5 to 10 striae, a score of 2 was given, and for more than 10 striae, a score of 3 was assigned. For the absence of erythema, a score of 0 was given. For mild erythema (light red or pink), a score of 1 was assigned. For marked erythema (dark red), a score of 2 was given; for intense erythema (purple), a score of 3 was assigned. The total score ranged from 0 to 3, indicating no striae or negligible striae, from 4 to 9, indicating mild striae, and from 10 to 15, indicating moderate striae. Finally, scores above 16 indicate severe striae. These two scores were then summed up to obtain the overall score. Based on this, the total striae score ranged from 0 to 24 for all body parts. Women were divided into the following four groups: Scores of 0-3 indicating no signs of pregnancy striae, scores of 4-9 indicating mild striae, scores of 10-15 indicating moderate striae, and scores above 16 indicating severe striae (Atwal et al., 2006).
The validity of the Atwal SG score has been confirmed by Atwal et al. (2006). The validity of both tools was also confirmed by 7 faculty members at Iran University of Medical Sciences (IUMS). Inter-rater reliability was utilized to assess the reliability of the Atwal SG scorecard. In this manner, the status, number, and severity of pregnancy-related striae were independently examined and recorded by the researcher and a midwifery expert in 10 participants. The correlation between the results was determined, and ultimately, an intra-class correlation coefficient value of 1 was obtained for all the areas, indicating a perfect agreement.
Study intervention
The primiparous mothers were enrolled in the study at weeks 18-20 of gestation and were followed up for 4 months during their pregnancy (at 4, 8, 12, and 16 weeks after the initiation of the intervention). The sampling for this study was done in six months, from July 20, 2022, to January 20, 2023. The pregnant women were provided with necessary explanations regarding the implementation of the research, and it was mentioned that they may be randomly assigned to either the intervention or placebo groups. The questionnaire on personal characteristics, BMI, and gestational age was completed at the beginning of the study. Then, pregnant women who met the research criteria were placed into either the vitamin C cream group or the placebo group based on a predetermined table after completing the demographic information form. These creams were prepared at the researcher’s request and in collaboration with a consultant pharmacist from the Faculty of Traditional Medicine at Iran University of Medical Sciences. The creams of both groups had similar packaging and appearance, and they shared the same color and smell. Concealment was also performed based on the code provided by the sealed envelope website, and the creams were divided into two groups: Group A and group B. The vitamin C cream contained 3% topical vitamin C in 100 g of Oraand base cream, including alco-acetyl, glycerin, triethanolamine, monostarch acid, white vaseline, and distilled water. The placebo cream, on the other hand, was composed of the Oraand base cream without any active ingredients.
The participants of both groups were provided with detailed recommendations on the correct use of the creams. They were advised to apply a thin layer of creams twice a day at 12-hour intervals topically with their fingers, gently and without massaging for 4 months. The subjects were instructed not to wash off the cream until fully absorbed. Furthermore, the researcher provided face-to-face instructions to women on correctly completing the daily checklists during their first visit. Before the intervention, the researcher observed and recorded the number and severity of striae using the Atwal scorecard. After each use, the women were asked to record the daily application of the creams on the checklists. The researcher used the Atwal scorecard to assess the number and severity of pregnancy-induced striae at 4, 8, 12, and 16 weeks after the initiation of the intervention. The researcher visited the research samples at the Perinatology Clinic of Shahid Akbarabadi Center at different follow-up times. During each visit, the researcher examined the usage of each cream by the subjects. The examination times of the samples were matched with their scheduled visits for pregnancy care. Additionally, due to the impact of weight on striae, the patient’s weight was measured at each stage. The researcher maintained weekly communication with the research samples through phone calls or messages to ensure the proper use of creams, completion of the checklists, and to stay informed about potential side effects such as itching and redness. The subjects were requested in advance to inform the researcher if they experienced any side effects. The sampling process continued until the completion of the final sample size, taking into account the possibility of sample attrition in both groups. At the end of the study, the researcher recorded the BMI and gestational age of the women and documented the occurrence and severity of pregnancy striae.
Blinding
This study was a triple-blinded, randomized controlled trial. The analyst, the researcher, and the samples were unaware of the groups. The samples were unaware whether they were assigned to the intervention or control group. Both groups received creams. Neither the researcher nor the samples were aware of the contents of the creams, as they had identical packaging, appearance, color, and smell, and there were no differences in the shape and color of the creams.
Data analysis
The data were analyzed using descriptive statistics (relative frequency and Mean±SD). Since the Kolmogorov-Smirnov test showed that the data distribution was not normal, the non-parametric Mann-Whitney U test was used to compare the incidence of striae. Also, the chi-square test was used to compare the education and midwifery characteristics; the Fisher exact test was used to compare the economic status, and the independent t-test was used to compare the age and BMI between the two groups. SPSS software, version 16, was used to analyze the data, and the significance level was set at P<0.05.
Results
Most of the subjects in the vitamin C group were 35-40 years old, while in the placebo group, the age range was 30-35 years. After the intervention, their BMI ranged between 25 and 29.9 (Table 1). There was no significant difference between the groups in terms of age, education level, economic status, and BMI (P>0.05) (Table 1).
There was no significant difference between the skin color, history of abortion, and history of striae in first-degree relatives of the two groups (P>0.05) (Table 2).
As Table 3 shows, there is a significant difference between the occurrence of pregnancy striae between the two groups at weeks 4 (P=0.012), 8 (P=0.004), 12 (P=0.001), and 16 (P<0.001) after the intervention.
Discussion
This study was conducted to determine the effect of vitamin C cream on pregnancy striae in primiparous women. The results showed a significant difference between the group using vitamin C and the placebo group in terms of the incidence of pregnancy striae. Although research conducted in this field is limited and scarce, and vitamin C has not been specifically used in this regard, a study by Abdolbaghiyan et al. (2020) entitled “expression changes of collagen І and ІІІ genes in human skin fibroblast cells due to microalgae extract Chlorella vulgaris and its comparison with vitamin C” conducted at the National Center of Genetic and Biological Resources of Iran, demonstrated that the algae extract and vitamin C have increased the expression of collagen type І by 3.14-fold and 1.42-fold, respectively. The C. vulgaris algae extract had a greater effect on the collagen type І gene expression. In comparison, vitamin C had a greater impact on increasing the expression of collagen type ІІІ gene, leading to a 2.12-fold increase in its expression. Finally, the findings indicated that C. vulgaris algae extract and vitamin C stimulate collagen synthesis in fibroblast cells, suggesting their potential as suitable alternatives to harmful chemicals used for collagen production in the skin (Abdolbaghiyan et al., 2020). These results align with the present study’s findings regarding the use of vitamin C in the collagen production process and its ultimate impact on pregnancy striae.
The results of a study by Hernández et al. (2013) to evaluate the effectiveness of an anti-crack cream (cream containing hydroxyprolisilane C, rosemary oil, Centella asiatica triterpenes, and vitamin E) in the prevention of SG, show that the use of the anti-crack skin product is effective in reducing the severity of striae during pregnancy. It effectively prevented the formation of new striae and halted the progression of existing ones. The result of this study is consistent with the findings of the present research regarding the use of topical compounds for pregnancy striae. It should be noted that C. asiatica extract contains vitamin C, and considering the effect of this vitamin on collagen production and its role in the skin, this compatibility can be considered. However, it cannot be fully expressed since vitamin C has not been used alone in this context (Hernández et al., 2013).
In 2018, Hajhashemi et al. conducted a study to evaluate the effectiveness of aloe vera gel and sweet almond oil on pregnancy striae in primiparous women. The findings demonstrated that the creams containing aloe vera and sweet almond oil had a greater impact on reducing striae erythema than base cream. These creams also reduced itching and prevented the progression of striae (P<0.001). The results of this study are consistent with the findings of the present research regarding the use of topical compounds on the severity of pregnancy striae erythema. Additionally, aloe vera gel contains vitamin C, and considering the effect of this vitamin on collagen production and its role in the skin, this correspondence can be significant (Hajhashemi et al., 2018). However, it should be noted that this correspondence cannot be fully accepted, as vitamin C alone was not used in the study.
In 2021, Bagherian et al. conducted a study to investigate the effect of aloe vera gel in preventing pregnancy striae. The study found that the incidence of striae (P=0.001) and the intensity of itching and erythema (P=0.001) in the 28th week of pregnancy were significantly lower in the group using aloe vera gel. This study concluded that due to the presence of vitamin C in aloe vera gel, it could be recommended to pregnant women as a low-cost option for preventing pregnancy striae (Bagherian et al., 2021). Aloe vera gel contains vitamin C, which is consistent with the findings of the present research regarding the use of vitamin C in preventing the occurrence of pregnancy striae. The results of this study confirmed the effectiveness of vitamin C in preventing pregnancy striae in women, and it can be utilized as an effective, affordable, safe, and acceptable intervention for pregnant women to prevent pregnancy striae. A systematic review of the role of vitamins in skin health demonstrated that vitamin C reduces dimer changes and thymine mutations caused by UV radiation, as well as the formation of apoptotic cells resulting from sunburn. These effects potentially reduce the risk of carcinogenesis. Additionally, vitamin C effectively improves skin elasticity, maintains moisture, and enhances the skin’s antioxidant capacity. The role of ascorbic acid in synthesizing collagen and elastin is very important in maintaining skin health. This vitamin is a cofactor for prolyl and lysyl hydroxylases, enzymes that catalyze the formation of hydroxyproline and hydroxylysine. It appears that ascorbate also regulates the transcription of collagen type I and III genes. In vitro studies have shown that fibroblasts stimulated with ascorbic acid exhibit increased collagen gene expression. Oral supplements of this vitamin can reduce the severity of skin spots, improve erythema and texture, and clean skin pores. Vitamin C levels are lower in aged or photodamaged skin, and adequate levels of ascorbic acid can help counteract the adverse effects of UV rays. Aged human skin fibroblasts can increase their proliferative capacity when treated with sufficient levels of ascorbic acid. Vitamin C deficiency is associated with the loss of several skin functions and changes in wound healing (related to the lack of collagen production), thickening of the stratum corneum, and subcutaneous bleeding due to fragility and changes in connective tissue morphology (Dattola et al., 2020). The result of this study is consistent with the findings of this research regarding the effect of vitamin C on collagen production.
Conclusion
This study examined the effect of vitamin C cream on pregnancy striae in primiparous women.
It is suggested that further studies be conducted to investigate the effectiveness of this cream in the treatment of SG, as well as their potential application to other populations, such as women looking to change their weight and athletes concerned about the development of stretch marks. The target audience for the results of this research includes primiparous women, obstetricians/gynecologists, midwives, healthcare providers, and officials and planners responsible for the educational and support programs for pregnant women. Considering that assisting pregnant women is one of the most important goals of midwifery and healthcare, one of these forms of assistance is the prevention and treatment of pregnancy striae. Due to the high prevalence of pregnancy striae and the significant costs associated with cosmetic products and medical treatments, the use of vitamin supplements is highly advantageous. It is necessary to provide sufficient information about striae to pregnant mothers to reduce their anxiety and concerns. It is suggested that further studies be conducted to investigate the effectiveness of these creams in treating SG and their potential application to other populations, such as women looking to change their weight and athletes concerned about the development of stretch marks. In this study, a vitamin C cream was used, and other vitamin creams, such as the combination of vitamin E and C, are recommended in future research to assess their impact on pregnancy striae. Additionally, the effectiveness of this cream should be explicitly investigated in multiparous women.
One of the strengths of this study was the presence of a placebo group, the random assignment of participants to different groups, and the blinding and concealment of the samples. Among the limitations of this research are the impossibility of precise control of the frequency of using the cream by the participants and the insufficient information about the serum levels of vitamin C in the samples.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Iran University of Medical Sciences (IUMS) (Code: IR.IUMS.REC.1401.215). The study proposal was registered in the Iranian Registry of Clinical Trials (IRCT) (Code:: IRCT20220509054799N1). A letter of introduction was obtained from the Faculty of Nursing and Midwifery at IUMS and the Shahid Akbarabadi Educational and Therapeutic Center in Tehran. Informed consent was obtained from all participants.
Funding
This article results from a Master’s thesis in Midwifery Education at Iran University of Medical Sciences (Project No.: 3-1400-3-3-22271). The Research Deputy of Iran University of Medical Sciences financially supported this study.
Authors' contributions
Supervison: Masoomeh Kheirkhah; Conceptualisation: Hadis Taheri and Masoomeh Kheirkhah; Implementation: Hadis Taheri; Sampling and data collection: Hadis Taheri and Nooshin Eshraghi; Data analysis and preparing the initial draft of the manuscript: Hadis Taheri and Shima Haghani; Preparation of creams: Hadis Taheri and Ali Ghobadi; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The research team expresses its great gratitude to the Research Vice-Chancellor of Iran University of Medical Sciences (IUMS). The authors also appreciate the Clinical Research Development Unit of Shahid Akbarabadi Hospital-IUMS for conducting this research.
References
Abbas A, et al., 2020, Atwal striae gravidarum score for prediction of perineal tears during vaginal delivery: A cross sectional study. World Journal of Gynecology & Women’s Health, 4(3), pp. 25-32. [DOI:10.33552/WJGWH.2020.04.000587]
Abdolbaghian, S., et al., 2020, [Gene expression changes of collagen І and ІІІ in human skin fibroblast cells in effect of microalga Chlorella vulgaris extract and compared to vitamin C (Persian). Journal of Marine Biology, 11(44), pp. 1-10. [Link]
Al-Niaimi, F. & Chiang, N. Y. Z., 2017. Topical Vitamin C and the Skin: Mechanisms of action and clinical applications. Journal of Clinical and Aesthetic Dermatology, 10(7), pp. 14-17. [PMID]
Atwal, G. S., et al., 2006. Striae gravidarum in primiparae. The British Journal of Dermatology, 155(5), pp. 965–9. [DOI:10.1111/j.1365-2133.2006.07427.x] [PMID]
Austin MP, et al., 2005, Maternal trait anxiety, depression and life event stress in pregnancy: relationships with infant temperament. Early Hum Dev 81(2):183-90. [DOI:10.1016/j.earlhumdev.2004.07.001] [PMID]
Bagherian, S., et al., 2021. [Effect of Aloe Vera Gel on prevention of Striae Gravidarum (Persian)]. Iranian Journal of Obstetrics, Gynecology and Infertility, 23(11), pp. 41-50. [DOI:10.22038/IJOGI.2021.17619]
Brennan M, et al., 2020, A qualitative study of the factors influencing recruitment to a pilot trial on the prevention of striae gravidarum. BMC Pregnancy and Childbirth, 20(1), pp. 103. [DOI:10.1186/s12884-020-2781-x] [PMID]
Brennan M & Clarke M & Devane D, 2016, The use of anti-stretch marks’ products by women in pregnancy: a descriptive, cross-sectional survey. BMC Pregnancy and Childbirth Sep 21;16(1):276. [DOI:10.1186/s12884-016-1075-9] [PMID]
Conningham, F. G., et al., 2022. Williams Obstetrics 26e. New York: McGraw Hill Medical. [Link]
Dattola A, et al., 2020, Role of Vitamins in Skin Health: A Systematic Review. Current Nutrition Reports, 9(3), pp. 226–35. [DOI:10.1007/s13668-020-00322-4] [PMID]
Findik, R. B, et al., 2011, Striae gravidarum, vitamin C and other related factors. International Journal for Vitamin and Nutrition Research. Internationale Zeitschrift fur Vitamin- und Ernahrungsforschung. Journal International de Vitaminologie et de Nutrition, 81(1), pp. 43–8. [DOI:10.1024/0300-9831/a000049] [PMID]
Gaber, M. & Mohamed Elshafie, A., 2021. The impact of striae gravidarum on quality-of-life issues. The Egyptian Journal of Hospital Medicine, 82(1), pp. 31-6. [DOI:10.21608/ejhm.2021.137550]
García Hernández, J. Á., et al., 2013. Use of a specific anti-stretch mark cream for preventing or reducing the severity of striae gravidarum. Randomized, double-blind, controlled trial. International Journal of Cosmetic Science, 35(3), pp. 233-7. [DOI:10.1111/ics.12029] [PMID]
Hajhashemi, M., et al., 2018. The effect of Aloe vera gel and sweet almond oil on striae gravidarum in nulliparous women. The Journal of Maternal-Fetal & Neonatal Medicine: The Official Journal of the European Association of Perinatal Medicine, The Federation of Asia and Oceania Perinatal Societies, the International Society of Perinatal Obstetricians, 31(13), pp. 1703–8. [DOI:10.1080/14767058.2017.1325865] [PMID]
García Hernández, J. Á., et al., 2013. Use of a specific anti-stretch mark cream for preventing or reducing the severity of striae gravidarum. Randomized, double-blind, controlled trial. International Journal of Cosmetic Science, 35(3), pp. 233–7.[DOI:10.1111/ics.12029] [PMID]
Hocaoglu, E., Hocaoglu, M. & Akdeniz, E., 2020. Association between serum 25-hydroxyvitamin D levels and the presence and severity of striae gravidarum in primigravid women. Journal of Cosmetic Dermatology, 19(11), pp. 3107–14. [DOI:10.1111/jocd.13386] [PMID]
Kamrani A & Malakouti J & Farshbaf Khalili A, 2015, [The effect of sweet almond oil, sesame oil and the combination of sweet almond oil and sesame oil in the prevention of striae pregnancy and the itching caused by it in primiparous women: a randomized controlled clinical trial (Persian)]. Iranian Journal of Obstetrics, Gynecology and Infertility. 18(169);1-11.[DOI: 10.22038/IJOGI.2015.6129]
Khalid El, et al., 2021, Assessment of Quality of Life and Sexual Function in ladies with Pregnancy-Related Skin Changes, The Egyptian Journal of Hospital Medicine 83(1):1105-1112. [DOI:10.21608/ejhm.2021.160881]
Kocaöz S & Gördeles Beşer N & Kizilirmak A. 2019, Striae gravidarum in primigravid women: prevalence, risk factors, prevention interventions and body image. The Journal of Maternal-Fetal & Neonatal Medicine 33(23):1-7. [DOI:10.1080/14767058.2019.1591363] [PMID]
Korgavkar, K. & Wang, F., 2015. Stretch marks during pregnancy: A review of topical prevention. The British Journal of Dermatology, 172(3), pp. 606-15. [DOI:10.1111/bjd.13426] [PMID]
Liu, L., et al., 2018. Risk factors of striae gravidarum in Chinese primiparous women. Plos One, 13(6), pp. e0198720. [DOI:10.1371/journal.pone.0198720] [PMID]
Moloudi Mones, et al., 2014, Evaluation of pregnancy striae and related risk factors in primiparous women referring to Imam Reza (AS) Hospital in Urmia. Journal of Nursing and Midwifery 12(3):207-213. [Link]
Newman WA. 2004, Dorland's medical dictionary [Persian trans] Mohebi, H., Nikfarjam R. Tehran: Golban Medical Publication 803. [Link]
Osman H, et al., 2007, Risk factors for the development of steria gravidarum. A M J Obstet Gynecol 196(1):62.e1-5. [DOI:10.1016/j.ajog.2006.08.044] [PMID]
Osman H, et al., 2008, Cocoa butter lotion for prevention of striae gravidarum: a double-blind, randomised and placebo-controlled trial. BJOG 115(9):1138-42. [DOI:10.1111/j.1471-0528.2008.01796.x] [PMID]
Ren P, et al., 2019, Risk factors for the formation of striae gravidarum in women in Jiangsu Province of China. Taiwan J Obstet Gynecol 58(5):640-644. [DOI:10.1016/j.tjog.2019.07.010] [PMID]
Rodrigues M, et al., 2020, Evaluation of effect of a vitamin-based barrier cream on the clinical severity of actinic cheilitis: A preliminary study. Oral Medicine and Pathology 12(10): 944-50. [DOI:10.4317/jced.57013] [PMID]
Sauermann, K., et al., 2004. Topically applied vitamin C increases the density of dermal papillae in aged human skin. BMC Dermatology, 4(1), pp. 13. [DOI:10.1186/1471-5945-4-13] [PMID]
Seirafianpour, F., et al., 2021. Systematic review of single and combined treatments for different types of striae: A comparison of striae treatments. Journal of the European Academy of Dermatology and Venereology: JEADV, 35(11), pp. 2185–98. [DOI:10.1111/jdv.17374] [PMID]
Sheldon R. et al., 2001, Topical L-Ascorbic Acid: Percutaneous Absorption Studies. American Society for Dermatologic Surgery. Dermatol Surg 27(2):137-42. [DOI:10.1046/j.1524-4725.2001.00264.x] [PMID]
Slade, P., et al., 2019. Establishing a valid construct of fear of childbirth: Findings from in-depth interviews with women and midwives. BMC Pregnancy and Childbirth, pp. 19(1), 96.[DOI:10.1186/s12884-019-2241-7] [PMID]
Soltanipour F, et al., 2012, Determining the effect of teak cream on pregnancy striae. Scientific Research Journal of Yasouj University of Medical Sciences, 17(5):379-386. [DOI: 10.1016/j.ctim.2013.11.011] [PMID]
Taavoni, S., et al., 2012. [The effect of olive oil and teak cream on striae of pregnancy in the second trimester of pregnancy (Persian)]. Iranian Journal of Nursing, 25(75), pp. 45-51. [Link]
Taavoni, S., et al., 2010. [A survey on the effects of olive oil on striae gravidarum in the second trimester of pregnancy (Persian)]. Nursing and Midwifery Journal, 8(1), pp. 6-10. [Link]
Taavoni, S., et al., 2011. Effects of olive oil on striae gravidarum in the second trimester of pregnancy. Complementary Therapies in Clinical Practice, 17(3), pp. 167–9. [DOI:10.1016/j.ctcp.2010.10.003] [PMID]
Tabaee, S., et al., 2016. [Investigating the effect of fractional ablative CO2 laser in reducing pregnancy striae in patients with pregnancy striae (Persian)]. Laser in Medicine, 14(1), pp. 2-9. [Link]
Wollina, U. & Goldman, A., 2017. Management of stretch marks (with a focus on striae rubrae). Journal of Cutaneous and Aesthetic Surgery, 10(3), pp. 124-9. [DOI:10.4103/JCAS.JCAS_118_17] [PMID]
Type of Study: Research |
Subject:
Special
Received: 2023/06/17 | Accepted: 2023/11/5 | Published: 2024/05/1
Received: 2023/06/17 | Accepted: 2023/11/5 | Published: 2024/05/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
