Fri, Jul 4, 2025
[Archive]
Volume 10, Issue 3 (Summer 2024)
JCCNC 2024, 10(3): 191-198 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Fili R, Nazmi S, Behmanesh F, Omrani A, Nikbakht H, Amiri Farahani L. Barriers to Physical Activity in Pregnant Women: An Explanatory Sequential Mixed-method Study (Study Protocol). JCCNC 2024; 10 (3) :191-198
URL: http://jccnc.iums.ac.ir/article-1-530-en.html
URL: http://jccnc.iums.ac.ir/article-1-530-en.html
Romina Fili1 

 , Sana Nazmi1 , Fereshteh Behmanesh *2 , Atefeh Omrani3 , Hossein-Ali Nikbakht4 , Leila Amiri Farahani5
, Sana Nazmi1 , Fereshteh Behmanesh *2 , Atefeh Omrani3 , Hossein-Ali Nikbakht4 , Leila Amiri Farahani5
, Sana Nazmi1 , Fereshteh Behmanesh *2 , Atefeh Omrani3 , Hossein-Ali Nikbakht4 , Leila Amiri Farahani5
1- Student Research Committee, Babol University of Medical Sciences, Babol, Iran.
2- Social Determinants of Health Research Center, Health Research Institute, Babol University of Medical Sciences, Babol, Iran. ,f.behmanesh2015@gmail.com
3- Department of Health and Social Care, Faculty of Education and Society, University of Sunderland, London, United Kingdom.
4- Department of Biostatistics & Epidemiology, Social Determinants of Health Research Center, School of Public Health, Health Research Institute, Babol University of Medical Sciences, Babol, Iran.
5- Nursing and Midwifery Care Research Center, School of Nursing and Midwifery, Iran University of Medical Sciences, Tehran, Iran.
2- Social Determinants of Health Research Center, Health Research Institute, Babol University of Medical Sciences, Babol, Iran. ,
3- Department of Health and Social Care, Faculty of Education and Society, University of Sunderland, London, United Kingdom.
4- Department of Biostatistics & Epidemiology, Social Determinants of Health Research Center, School of Public Health, Health Research Institute, Babol University of Medical Sciences, Babol, Iran.
5- Nursing and Midwifery Care Research Center, School of Nursing and Midwifery, Iran University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 686 kb]
(393 Downloads)
| Abstract (HTML) (1841 Views)
Full-Text: (234 Views)
Introduction
Popular ways to do physical activity include moderate to severe (e.g. exercise, sports) and light activities (e.g. leisurely walking and routine daily tasks) (Meah et al., 2021). However, the prevalence of obesity and weight gain is increasing in Iran, and women are more at risk of weight gain than men (Yaghoobi et al., 2015). In the past, pregnant women were banned from physical activity. However, it is widely acknowledged that regular physical activity during pregnancy offers numerous benefits for maternal and fetal health (Guelfi et al., 2015; Misan et al., 2022). Regular and planned physical activity during pregnancy improves physical fitness and reduces the risk of maternal weight gain (Meah et al., 2021; Guelfi et al., 2015; Misan et al., 2022; Harrison et al., 2018), which is increasing worldwide and threatens maternal and fetal health (Hsiung et al., 2021). Despite the proven benefits of physical activity, many women prefer a sedentary lifestyle during pregnancy (Guelfi et al., 2015; Shakibzadeh et al., 2020). International studies show that many women reduce their physical activity levels since 23 to 25 weeks of pregnancy (Bauer et al., 2018). Physical activity in pregnancy decreases the risk of preeclampsia (Santos et al., 2014), high blood pressure (Connelly et al., 2015), gestational diabetes (Coll et al., 2017) and prenatal depression (Meah et al., 2021). It also reduces lower back pain and anxiety and improves sleep (Shakibzadeh et al., 2020; Coll et al., 2017; Harrison et al., 2018).
Some researchers have shown that physical activity during pregnancy reduces the risk of macrosomia, preterm labor, and cesarean section (Coll et al., 2017). Furthermore, it shortens the duration of delivery (Connolly et al., 2014). The increase in cesarean section rates in Iran is believed partly due to prolonged labor (Azizi et al., 2021), so physical activity may help alleviate this problem.
Infants born to physically active mothers during pregnancy are reported to have better neurological development (Connolly et al., 2014). Therefore, pregnant women are recommended to be physically active on most days of the week to enjoy its health-related benefits (Shakibzadeh et al., 2020).
Physical activity during pregnancy can be influenced by attitude, subjective norms and perceived behavior control (Guelfi et al., 2015). Pregnant women have stated that even with the availability of a wide range of sources of information, including advice from healthcare providers, friends, family, printed materials, the Internet and the media, physical activity is still a difficult and complicated subject for them (Evenson & Bradley, 2010). Pregnant women choose a more sedentary lifestyle for various reasons (Flannery et al., 2018). In a US-based survey, 60% of pregnant women were sedentary, while the mean inactivity in society was 30% (Rafiei et al., 2018). In a study in Iran, 40% of pregnant women avoided physical activity even though they had no restrictions to exercise during pregnancy (Rahimi & Seyed Rasouli, 2005). Research has shown that barriers to physical activity in pregnancy include fear of miscarriage (Shakibzadeh et al., 2020), adverse effects of physical activity on fetal health (Shakibzadeh et al., 2020; Okafor & Ter Goon, 2022), fatigue (Meah et al., 2021), busy life and suffering from physical symptoms, such as nausea, back pain (Dolatabadi et al., 2022), shortness of breath, heartburn and leg cramps (Guelfi et al., 2015; Bauer et al., 2018).
Identifying the barriers to physical activity in pregnancy can contribute to a deeper understanding of the factors influencing the attitudes and perceptions of pregnant women toward engaging in physical activities (Harrison et al., 2018). It is also important for future interventions to enhance physical activity during pregnancy (Okafor & Ter Goon, 2022).
Consistent physical activity offers numerous advantages for maternal and fetal health during pregnancy (Guelfi et al., 2015). Therefore, it is crucial to comprehend the obstacles of physical activity. This understanding is essential for shaping future interventions to enhance physical activity in pregnant women (Shakibzadeh et al., 2020).
Limited studies have been conducted on barriers to physical activity and pregnant women’s feelings and perceptions about exercise during pregnancy (Rafiei et al., 2018). While previous investigations into obstacles of physical activity during pregnancy have been either solely quantitative or qualitative, combining both approaches can yield more valid and lucid results. Notably, no existing study in Iran has investigated this issue and no explanatory sequential mixed methods design has been employed.
Relying solely on quantitative research results, without complementary qualitative research, may not suffice for developing effective interventions to alter women’s perceptions and behaviors regarding physical activity during pregnancy. Furthermore, due to its limitation in generalizing to the wider society, qualitative research lacks efficiency for practical planning.
A mixed-method design enhances the quality of inferences and reduces the potential bias associated with relying solely on a single research method (Subedi, 2016).
In the first phase of this study, a questionnaire will be used to gather data and determine barriers to physical activity in pregnant women admitted to pregnancy clinics covered by Babol University of Medical Sciences in Iran. A qualitative study will be conducted after analyzing the results of the quantitative phase of the study. The second phase will aim to explain the results of quantitative research further. In the qualitative phase of the study, in-depth interviews will be conducted to discuss barriers to physical activity, women’s false beliefs and misconceptions around this issue, or barriers not directly mentioned in the questionnaire. Participating women can freely and without any limitations discuss their perceived barriers and beliefs about physical activity during pregnancy. Applying a mixed-method approach strengthens the results of research by putting together the powers of quantitative studies (generalization, large sample size) and qualitative studies (listening to participants’ points of view and gaining in-depth insights through discussions), hence providing a more complete picture of the subject (Taghizadeh et al., 2015). As a result, the present mixed-method study will be conducted with the following objectives.
Quantitative objective: To determine the barriers to physical activity in pregnant women admitted to pregnancy clinics covered by Babol University of Medical Sciences, Iran; qualitative objective: To explain the barriers to physical activity from the perspectives of pregnant women admitted to pregnancy clinics covered by Babol University of Medical Sciences, Iran and mixed-method objective: To integrate the quantitative and qualitative findings and interpret the barriers to physical activity in pregnant women admitted to pregnancy clinics covered by Babol University of Medical Sciences, Iran.
Materials and Methods
This research is an explanatory sequential mixed-method study. This two-phase research will be conducted to determine and interpret the barriers to physical activity in pregnant women admitted to pregnancy clinics covered by Babol University of Medical Sciences, Iran. In the study’s first phase, barriers to physical activity during pregnancy scale (BPAPS) and demographic and obstetric data questionnaires will be used to collect quantitative data. The second qualitative phase of the study will be implemented to explain the pregnant women’s perspectives regarding barriers to physical activity in the light of quantitative data. Thus, the unexpected, astonishing results of key variables that differentiate groups of participants or locate them at the two ends of a spectrum will be studied in depth. Using a symbolization system, the sequence and weight of quantitative and qualitative phases in the study can be shown as follows: Quan→qual. The researchers prioritize the initial quantitative stage, and the subsequent qualitative stage provides a more detailed explanation of the quantitative results. Finally, quantitative and qualitative findings will be integrated and interpreted for more valid results.
Phase one: Quantitative study
Design, setting and sample
The quantitative phase of the project is a cross-sectional study that will use a demographic and obstetrics information questionnaire and a valid and reliable questionnaire to collect data regarding barriers to physical activity in pregnant women. The subjects will be recruited using convenience sampling from pregnant women who meet the inclusion criteria. The study setting will be pregnancy clinics covered by Babol University of Medical Sciences, Iran.
According to the objectives, the maximum sample size is determined in this study. Referring to previous studies (Dolatabadi et al., 2022) regarding the Mean±SD of the total barriers to physical activity (88.55±19.28) and considering a confidence level of 95% with an acceptable error of 1.5, it is calculated that 325 participants are required. Due to the possible sample attrition, 10% will be added to the obtained sample size and the final sample size will be 358. The sample size formula and its values are provided in Equation 1:

Where n is the number of samples required, and the probability of the first type error (α) equals 0.05. As a result, the (Z) equals 1.96, (σ) standard deviation is 19.28 and d estimation error is the desired accuracy in parameter estimation as 1.5.

The inclusion criteria for the first phase of the study are as follows: Aged 18 to 45 years, gestational age of 10 to 37 weeks, no medical conditions that restrict or prevent exercise during pregnancy, the ability to read and write, lack of disability and symptoms of excessive shortness of breath, severe chest pain, dizziness or fainting that cannot be resolved by rest and lack of symptoms of preterm labor (e.g. regular and painful contractions of the uterus, vaginal bleeding and continuous loss of vaginal fluid). The exclusion criteria will involve participants who fail to respond to a maximum of 10% of the questions in the questionnaire (Nulty, 2008). Participation in the study is entirely voluntary, and participants have the freedom not to fill out the questionnaire or withdraw from the study at any point. Women participating in the qualitative phase will be requested to share their phone numbers. It is assured that their information will be kept confidential.
Study instruments
Demographic and obstetrics information questionnaire: Questions will be asked to collect information regarding age, education, place of residence, husband’s age, woman’s employment status, husband’s job, living expenses, history of smoking, alcohol and drug abuse, weight, gestational age, number of children, number of previous pregnancies and involvement in childbirth preparation classes, body mass index (BMI) before pregnancy or early pregnancy and routine exercise before pregnancy.
BPAPS: The scale was developed by Amiri-Farahani et al. (2021) and comprises 29 questions with four factors: “Pregnancy-related intrapersonal barriers,” “non-pregnancy-related intrapersonal barriers,” “interpersonal barriers” and “environmental barriers.” The items are scored on a 5-point Likert scale from 5=strongly agree to 1=strongly disagree. The BPAPS total score ranges from 29 to 145, with a higher score indicating a greater presence of barriers to physical activity during pregnancy. The Cronbach α for the 29-point scale was 0.824, and the intra-class correlation coefficient (ICC) between the test and the retest was 0.87, confirming the high reliability of this scale. The construct validity of BPAPS was confirmed through known group validation and exploratory factor analysis (Amiri-Farahani et al., 2021).
Quantitative data analysis
Descriptive statistics will be employed to characterize socio-demographic and obstetric variables and women’s barriers to physical activity. The Pearson correlation coefficient will investigate the linear relationships between quantitative variables, such as barriers to physical activity and its subscales. Linear regression will also be applied to predict the association between the barriers to physical activity and its subscales with other variables. Multivariate analysis will be employed to control confounding variables in the study. In this analysis, standard and non-standard regression coefficients and their corresponding 95% confidence intervals (CI) will be presented as measures of the effect size. All the tests will be two-tailed. The analyses will be performed using SPSS software, version 20, and P<0.05 will be deemed statistically significant.
Phase two: Qualitative study
This phase aims to provide a more detailed explanation of the results obtained in the quantitative phase by incorporating insights from the qualitative data.
Study participants
It is important to note that in an explanatory sequential study, quantitative and qualitative data collection are interconnected rather than distinct phases. Since the researcher aims to elucidate preliminary quantitative findings in this model, individuals involved in the qualitative follow-up phase should be the same as those who participated in the quantitative data collection. Simultaneously, quantitative statistical results guide the ongoing sampling process, allowing the selection of participants who are best suited to provide insights into the phenomenon under investigation. At this stage, the sampling approach will involve purposeful sampling, where participants will be invited based on the results of the quantitative phase. Thus, the unexpected, astonishing results and key variables that differentiate groups of participants or locate them at the two ends of a spectrum will be studied more deeply (Cresswell & Clark, 2011).
There is no specific guideline for sample size in qualitative studies. The sample size cannot be measured by previous qualitative research and sampling will continue until data saturation is reached. Participants will be recruited based on the findings from the quantitative phase of the study. This condition implies that the initial quantitative findings will guide the formulation of study questions (interview guide) and select participants for the qualitative phase. This design represents an emergent approach in mixed-method studies, as Cresswell & Clark, (2011) outlined.
Data generation
At this phase, individual semi-structured interviews will be conducted. Upon inviting the recruited women to participate in interviews, the scheduling and location of the interviews will be organized to suit their convenience. In addition to the interviewer’s notes taken during the interviews, each session will be audio-recorded. Before conducting the research, an interview guide will be prepared and ways to obtain valid data from the interviews and how to focus on the research questions will be reviewed.
When participants provide concise answers, express themselves unclearly, or introduce significant points not covered by others, in-depth and probing questions will be employed. Such questions may include prompts like “Can you explain more?” “What do you mean?” “Why?” and “How?”. Interviews will continue until data saturation is achieved. The duration of each interview will vary based on conditions, the interviewee’s ability to articulate and their willingness to continue the conversation.
Data trustworthiness
In this study, Enworo (2023) criteria, including credibility, dependability, confirmability and transferability, will be used to ensure the trustworthiness of the data. Based on this, long engagement with the data in the research environment, member checking, peer debriefing, data source triangulation, inquiry audit, audit trail, reflexivity and a thick description of the study context will be used (Enworo, 2023).
Qualitative data analysis
Conventional content analysis will be employed to analyze qualitative data. The advantage of this approach lies in acquiring direct information from participants’ data without imposing predetermined categories or pre-existing theoretical perspectives (Graneheim & Lundman, 2004). The researchers will meticulously examine the interview transcriptions, extracting codes, categories, and themes. The recordings will be listened to multiple times to establish a general framework. Subsequently, each audio-taped interview will be transcribed accurately by the corresponding author and thoroughly reviewed to capture its apparent and intrinsic elements. The text will be coded and these codes will be iteratively applied to sentences or significant paragraphs until the themes and categories emerge. The expected outcome is that the themes emerging from this phase will provide additional insights and interpretations of the quantitative results. The outcome is the emergence of themes and categories that will complete the results obtained from the initial stage of the study (Taghizadeh et al., 2015). MAXQDA software, version 10 will be employed to manage the qualitative data analysis.
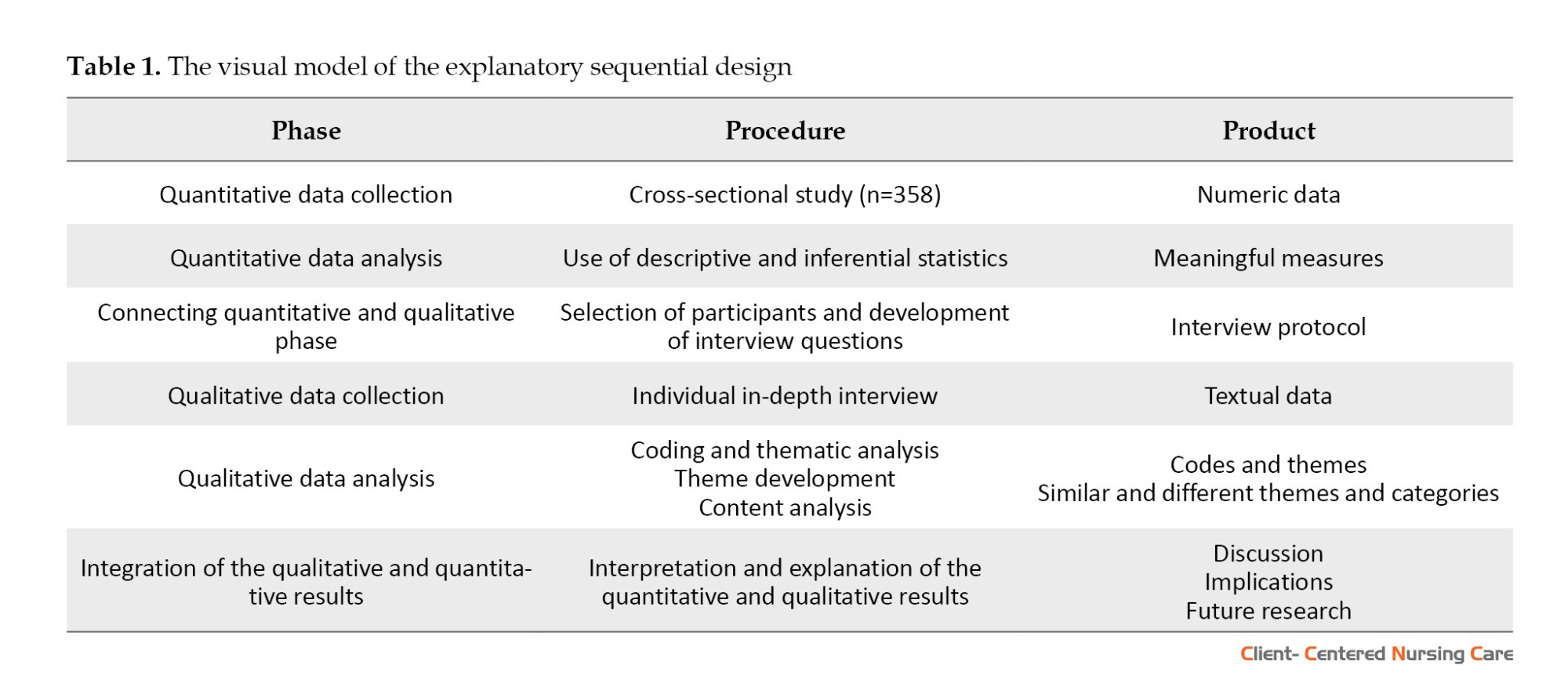
Integration of quantitative and qualitative results
In the last stage, following the analysis of the qualitative data, an interpretation of the results of the quantitative study will be presented using the findings of the qualitative study. The visual model of explanatory sequential design is shown in Figure 1 (Cresswell & Clark, 2011) and Table 1.

Discussion
This study aims to explain and interpret barriers to physical activity in pregnant women by applying an explanatory sequential mixed method. Identifying pregnant women’s beliefs, habits and perceptions about physical activity enables practitioners to address the barriers and issues more effectively. This research is the first study in Iran to explain and interpret obstacles to physical activity in pregnant women with an explanatory sequential mixed-method design. Limited studies have been conducted on barriers to physical activities during pregnancy and pregnant women’s perceptions and beliefs about exercise and physical activity during pregnancy (Rafiei et al., 2018). Therefore, there is a need for additional research in this area, particularly in developing countries like Iran. This research will especially facilitate the handling of issues such as the increase in obesity and cesarean section among pregnant women in Iran (Azizi et al., 2021; Yaghoobi et al., 2015).
In this study, after analyzing the results of the quantitative phase, the mean BPAPS values during pregnancy and its specific subscales, encompassing “pregnancy-related intrapersonal barriers,” “non-pregnancy related intrapersonal barriers,” “interpersonal barriers” and “environmental barriers,” will be determined. In addition, the relationship between physical activity barriers and socio-demographic and midwifery variables will be determined. During this stage, specific questions may arise, necessitating further clarification. The qualitative study will play a crucial role in providing this necessary explanation. The extraction of codes, categories and themes in the qualitative phase will aid in interpreting how to explain quantitative results through qualitative research. Utilizing an explanatory sequential mixed method design is a notable strength of the study, offering a richer and more detailed exploration of the barriers to physical activity in pregnant women.
The study’s findings can significantly impact women’s misconceptions regarding barriers to physical activity during pregnancy. Moreover, the results will be valuable in designing interventions to eliminate these barriers, promote physical activity participation, and enhance pregnant women’s overall health and well-being, consequently reducing the risk of pregnancy complications.
However, one potential limitation in this study could be the non-cooperation of mothers in participating in the second phase. To address this limitation, the researcher will try to communicate the study objectives and assure participants of the confidentiality of the information gathered.
Conclusion
Regular exercise during pregnancy brings numerous advantages for both maternal and fetal health. The results of this study are crucial for strategic planning, aiming to correct misconceptions about physical activity in pregnancy among women. Furthermore, this research will assist in developing interventions to eliminate barriers to exercise, promoting pregnant women's physical activity engagement, and ultimately enhancing their health and wellness throughout pregnancy.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of the Babol University of Medical Sciences (Code: IR.MUBABOL.HRI.REC.1401.238). During this study’s quantitative and qualitative stages, participants must provide written
informed consent.
Funding
This research was supported financially by Babol University of Medical Sciences (Grant No.: 724134896).
Authors' contributions
Writing the original draft: Fereshteh Behmanesh and Romina Fili; Review and editing: Sana Nazmi, Leila Amiri Farahani, Atefeh Omrani and Hossein-Ali Nikbakht; Conceptualization, study design and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank Vice-Chancellor for Research and Technology, Babol University of Medical Sciences for the financial support and Clinical Research Development Unit of Shahid Yahyanezhad Hospital.
References
Popular ways to do physical activity include moderate to severe (e.g. exercise, sports) and light activities (e.g. leisurely walking and routine daily tasks) (Meah et al., 2021). However, the prevalence of obesity and weight gain is increasing in Iran, and women are more at risk of weight gain than men (Yaghoobi et al., 2015). In the past, pregnant women were banned from physical activity. However, it is widely acknowledged that regular physical activity during pregnancy offers numerous benefits for maternal and fetal health (Guelfi et al., 2015; Misan et al., 2022). Regular and planned physical activity during pregnancy improves physical fitness and reduces the risk of maternal weight gain (Meah et al., 2021; Guelfi et al., 2015; Misan et al., 2022; Harrison et al., 2018), which is increasing worldwide and threatens maternal and fetal health (Hsiung et al., 2021). Despite the proven benefits of physical activity, many women prefer a sedentary lifestyle during pregnancy (Guelfi et al., 2015; Shakibzadeh et al., 2020). International studies show that many women reduce their physical activity levels since 23 to 25 weeks of pregnancy (Bauer et al., 2018). Physical activity in pregnancy decreases the risk of preeclampsia (Santos et al., 2014), high blood pressure (Connelly et al., 2015), gestational diabetes (Coll et al., 2017) and prenatal depression (Meah et al., 2021). It also reduces lower back pain and anxiety and improves sleep (Shakibzadeh et al., 2020; Coll et al., 2017; Harrison et al., 2018).
Some researchers have shown that physical activity during pregnancy reduces the risk of macrosomia, preterm labor, and cesarean section (Coll et al., 2017). Furthermore, it shortens the duration of delivery (Connolly et al., 2014). The increase in cesarean section rates in Iran is believed partly due to prolonged labor (Azizi et al., 2021), so physical activity may help alleviate this problem.
Infants born to physically active mothers during pregnancy are reported to have better neurological development (Connolly et al., 2014). Therefore, pregnant women are recommended to be physically active on most days of the week to enjoy its health-related benefits (Shakibzadeh et al., 2020).
Physical activity during pregnancy can be influenced by attitude, subjective norms and perceived behavior control (Guelfi et al., 2015). Pregnant women have stated that even with the availability of a wide range of sources of information, including advice from healthcare providers, friends, family, printed materials, the Internet and the media, physical activity is still a difficult and complicated subject for them (Evenson & Bradley, 2010). Pregnant women choose a more sedentary lifestyle for various reasons (Flannery et al., 2018). In a US-based survey, 60% of pregnant women were sedentary, while the mean inactivity in society was 30% (Rafiei et al., 2018). In a study in Iran, 40% of pregnant women avoided physical activity even though they had no restrictions to exercise during pregnancy (Rahimi & Seyed Rasouli, 2005). Research has shown that barriers to physical activity in pregnancy include fear of miscarriage (Shakibzadeh et al., 2020), adverse effects of physical activity on fetal health (Shakibzadeh et al., 2020; Okafor & Ter Goon, 2022), fatigue (Meah et al., 2021), busy life and suffering from physical symptoms, such as nausea, back pain (Dolatabadi et al., 2022), shortness of breath, heartburn and leg cramps (Guelfi et al., 2015; Bauer et al., 2018).
Identifying the barriers to physical activity in pregnancy can contribute to a deeper understanding of the factors influencing the attitudes and perceptions of pregnant women toward engaging in physical activities (Harrison et al., 2018). It is also important for future interventions to enhance physical activity during pregnancy (Okafor & Ter Goon, 2022).
Consistent physical activity offers numerous advantages for maternal and fetal health during pregnancy (Guelfi et al., 2015). Therefore, it is crucial to comprehend the obstacles of physical activity. This understanding is essential for shaping future interventions to enhance physical activity in pregnant women (Shakibzadeh et al., 2020).
Limited studies have been conducted on barriers to physical activity and pregnant women’s feelings and perceptions about exercise during pregnancy (Rafiei et al., 2018). While previous investigations into obstacles of physical activity during pregnancy have been either solely quantitative or qualitative, combining both approaches can yield more valid and lucid results. Notably, no existing study in Iran has investigated this issue and no explanatory sequential mixed methods design has been employed.
Relying solely on quantitative research results, without complementary qualitative research, may not suffice for developing effective interventions to alter women’s perceptions and behaviors regarding physical activity during pregnancy. Furthermore, due to its limitation in generalizing to the wider society, qualitative research lacks efficiency for practical planning.
A mixed-method design enhances the quality of inferences and reduces the potential bias associated with relying solely on a single research method (Subedi, 2016).
In the first phase of this study, a questionnaire will be used to gather data and determine barriers to physical activity in pregnant women admitted to pregnancy clinics covered by Babol University of Medical Sciences in Iran. A qualitative study will be conducted after analyzing the results of the quantitative phase of the study. The second phase will aim to explain the results of quantitative research further. In the qualitative phase of the study, in-depth interviews will be conducted to discuss barriers to physical activity, women’s false beliefs and misconceptions around this issue, or barriers not directly mentioned in the questionnaire. Participating women can freely and without any limitations discuss their perceived barriers and beliefs about physical activity during pregnancy. Applying a mixed-method approach strengthens the results of research by putting together the powers of quantitative studies (generalization, large sample size) and qualitative studies (listening to participants’ points of view and gaining in-depth insights through discussions), hence providing a more complete picture of the subject (Taghizadeh et al., 2015). As a result, the present mixed-method study will be conducted with the following objectives.
Quantitative objective: To determine the barriers to physical activity in pregnant women admitted to pregnancy clinics covered by Babol University of Medical Sciences, Iran; qualitative objective: To explain the barriers to physical activity from the perspectives of pregnant women admitted to pregnancy clinics covered by Babol University of Medical Sciences, Iran and mixed-method objective: To integrate the quantitative and qualitative findings and interpret the barriers to physical activity in pregnant women admitted to pregnancy clinics covered by Babol University of Medical Sciences, Iran.
Materials and Methods
This research is an explanatory sequential mixed-method study. This two-phase research will be conducted to determine and interpret the barriers to physical activity in pregnant women admitted to pregnancy clinics covered by Babol University of Medical Sciences, Iran. In the study’s first phase, barriers to physical activity during pregnancy scale (BPAPS) and demographic and obstetric data questionnaires will be used to collect quantitative data. The second qualitative phase of the study will be implemented to explain the pregnant women’s perspectives regarding barriers to physical activity in the light of quantitative data. Thus, the unexpected, astonishing results of key variables that differentiate groups of participants or locate them at the two ends of a spectrum will be studied in depth. Using a symbolization system, the sequence and weight of quantitative and qualitative phases in the study can be shown as follows: Quan→qual. The researchers prioritize the initial quantitative stage, and the subsequent qualitative stage provides a more detailed explanation of the quantitative results. Finally, quantitative and qualitative findings will be integrated and interpreted for more valid results.
Phase one: Quantitative study
Design, setting and sample
The quantitative phase of the project is a cross-sectional study that will use a demographic and obstetrics information questionnaire and a valid and reliable questionnaire to collect data regarding barriers to physical activity in pregnant women. The subjects will be recruited using convenience sampling from pregnant women who meet the inclusion criteria. The study setting will be pregnancy clinics covered by Babol University of Medical Sciences, Iran.
According to the objectives, the maximum sample size is determined in this study. Referring to previous studies (Dolatabadi et al., 2022) regarding the Mean±SD of the total barriers to physical activity (88.55±19.28) and considering a confidence level of 95% with an acceptable error of 1.5, it is calculated that 325 participants are required. Due to the possible sample attrition, 10% will be added to the obtained sample size and the final sample size will be 358. The sample size formula and its values are provided in Equation 1:
Where n is the number of samples required, and the probability of the first type error (α) equals 0.05. As a result, the (Z) equals 1.96, (σ) standard deviation is 19.28 and d estimation error is the desired accuracy in parameter estimation as 1.5.
The inclusion criteria for the first phase of the study are as follows: Aged 18 to 45 years, gestational age of 10 to 37 weeks, no medical conditions that restrict or prevent exercise during pregnancy, the ability to read and write, lack of disability and symptoms of excessive shortness of breath, severe chest pain, dizziness or fainting that cannot be resolved by rest and lack of symptoms of preterm labor (e.g. regular and painful contractions of the uterus, vaginal bleeding and continuous loss of vaginal fluid). The exclusion criteria will involve participants who fail to respond to a maximum of 10% of the questions in the questionnaire (Nulty, 2008). Participation in the study is entirely voluntary, and participants have the freedom not to fill out the questionnaire or withdraw from the study at any point. Women participating in the qualitative phase will be requested to share their phone numbers. It is assured that their information will be kept confidential.
Study instruments
Demographic and obstetrics information questionnaire: Questions will be asked to collect information regarding age, education, place of residence, husband’s age, woman’s employment status, husband’s job, living expenses, history of smoking, alcohol and drug abuse, weight, gestational age, number of children, number of previous pregnancies and involvement in childbirth preparation classes, body mass index (BMI) before pregnancy or early pregnancy and routine exercise before pregnancy.
BPAPS: The scale was developed by Amiri-Farahani et al. (2021) and comprises 29 questions with four factors: “Pregnancy-related intrapersonal barriers,” “non-pregnancy-related intrapersonal barriers,” “interpersonal barriers” and “environmental barriers.” The items are scored on a 5-point Likert scale from 5=strongly agree to 1=strongly disagree. The BPAPS total score ranges from 29 to 145, with a higher score indicating a greater presence of barriers to physical activity during pregnancy. The Cronbach α for the 29-point scale was 0.824, and the intra-class correlation coefficient (ICC) between the test and the retest was 0.87, confirming the high reliability of this scale. The construct validity of BPAPS was confirmed through known group validation and exploratory factor analysis (Amiri-Farahani et al., 2021).
Quantitative data analysis
Descriptive statistics will be employed to characterize socio-demographic and obstetric variables and women’s barriers to physical activity. The Pearson correlation coefficient will investigate the linear relationships between quantitative variables, such as barriers to physical activity and its subscales. Linear regression will also be applied to predict the association between the barriers to physical activity and its subscales with other variables. Multivariate analysis will be employed to control confounding variables in the study. In this analysis, standard and non-standard regression coefficients and their corresponding 95% confidence intervals (CI) will be presented as measures of the effect size. All the tests will be two-tailed. The analyses will be performed using SPSS software, version 20, and P<0.05 will be deemed statistically significant.
Phase two: Qualitative study
This phase aims to provide a more detailed explanation of the results obtained in the quantitative phase by incorporating insights from the qualitative data.
Study participants
It is important to note that in an explanatory sequential study, quantitative and qualitative data collection are interconnected rather than distinct phases. Since the researcher aims to elucidate preliminary quantitative findings in this model, individuals involved in the qualitative follow-up phase should be the same as those who participated in the quantitative data collection. Simultaneously, quantitative statistical results guide the ongoing sampling process, allowing the selection of participants who are best suited to provide insights into the phenomenon under investigation. At this stage, the sampling approach will involve purposeful sampling, where participants will be invited based on the results of the quantitative phase. Thus, the unexpected, astonishing results and key variables that differentiate groups of participants or locate them at the two ends of a spectrum will be studied more deeply (Cresswell & Clark, 2011).
There is no specific guideline for sample size in qualitative studies. The sample size cannot be measured by previous qualitative research and sampling will continue until data saturation is reached. Participants will be recruited based on the findings from the quantitative phase of the study. This condition implies that the initial quantitative findings will guide the formulation of study questions (interview guide) and select participants for the qualitative phase. This design represents an emergent approach in mixed-method studies, as Cresswell & Clark, (2011) outlined.
Data generation
At this phase, individual semi-structured interviews will be conducted. Upon inviting the recruited women to participate in interviews, the scheduling and location of the interviews will be organized to suit their convenience. In addition to the interviewer’s notes taken during the interviews, each session will be audio-recorded. Before conducting the research, an interview guide will be prepared and ways to obtain valid data from the interviews and how to focus on the research questions will be reviewed.
When participants provide concise answers, express themselves unclearly, or introduce significant points not covered by others, in-depth and probing questions will be employed. Such questions may include prompts like “Can you explain more?” “What do you mean?” “Why?” and “How?”. Interviews will continue until data saturation is achieved. The duration of each interview will vary based on conditions, the interviewee’s ability to articulate and their willingness to continue the conversation.
Data trustworthiness
In this study, Enworo (2023) criteria, including credibility, dependability, confirmability and transferability, will be used to ensure the trustworthiness of the data. Based on this, long engagement with the data in the research environment, member checking, peer debriefing, data source triangulation, inquiry audit, audit trail, reflexivity and a thick description of the study context will be used (Enworo, 2023).
Qualitative data analysis
Conventional content analysis will be employed to analyze qualitative data. The advantage of this approach lies in acquiring direct information from participants’ data without imposing predetermined categories or pre-existing theoretical perspectives (Graneheim & Lundman, 2004). The researchers will meticulously examine the interview transcriptions, extracting codes, categories, and themes. The recordings will be listened to multiple times to establish a general framework. Subsequently, each audio-taped interview will be transcribed accurately by the corresponding author and thoroughly reviewed to capture its apparent and intrinsic elements. The text will be coded and these codes will be iteratively applied to sentences or significant paragraphs until the themes and categories emerge. The expected outcome is that the themes emerging from this phase will provide additional insights and interpretations of the quantitative results. The outcome is the emergence of themes and categories that will complete the results obtained from the initial stage of the study (Taghizadeh et al., 2015). MAXQDA software, version 10 will be employed to manage the qualitative data analysis.
Integration of quantitative and qualitative results
In the last stage, following the analysis of the qualitative data, an interpretation of the results of the quantitative study will be presented using the findings of the qualitative study. The visual model of explanatory sequential design is shown in Figure 1 (Cresswell & Clark, 2011) and Table 1.
Discussion
This study aims to explain and interpret barriers to physical activity in pregnant women by applying an explanatory sequential mixed method. Identifying pregnant women’s beliefs, habits and perceptions about physical activity enables practitioners to address the barriers and issues more effectively. This research is the first study in Iran to explain and interpret obstacles to physical activity in pregnant women with an explanatory sequential mixed-method design. Limited studies have been conducted on barriers to physical activities during pregnancy and pregnant women’s perceptions and beliefs about exercise and physical activity during pregnancy (Rafiei et al., 2018). Therefore, there is a need for additional research in this area, particularly in developing countries like Iran. This research will especially facilitate the handling of issues such as the increase in obesity and cesarean section among pregnant women in Iran (Azizi et al., 2021; Yaghoobi et al., 2015).
In this study, after analyzing the results of the quantitative phase, the mean BPAPS values during pregnancy and its specific subscales, encompassing “pregnancy-related intrapersonal barriers,” “non-pregnancy related intrapersonal barriers,” “interpersonal barriers” and “environmental barriers,” will be determined. In addition, the relationship between physical activity barriers and socio-demographic and midwifery variables will be determined. During this stage, specific questions may arise, necessitating further clarification. The qualitative study will play a crucial role in providing this necessary explanation. The extraction of codes, categories and themes in the qualitative phase will aid in interpreting how to explain quantitative results through qualitative research. Utilizing an explanatory sequential mixed method design is a notable strength of the study, offering a richer and more detailed exploration of the barriers to physical activity in pregnant women.
The study’s findings can significantly impact women’s misconceptions regarding barriers to physical activity during pregnancy. Moreover, the results will be valuable in designing interventions to eliminate these barriers, promote physical activity participation, and enhance pregnant women’s overall health and well-being, consequently reducing the risk of pregnancy complications.
However, one potential limitation in this study could be the non-cooperation of mothers in participating in the second phase. To address this limitation, the researcher will try to communicate the study objectives and assure participants of the confidentiality of the information gathered.
Conclusion
Regular exercise during pregnancy brings numerous advantages for both maternal and fetal health. The results of this study are crucial for strategic planning, aiming to correct misconceptions about physical activity in pregnancy among women. Furthermore, this research will assist in developing interventions to eliminate barriers to exercise, promoting pregnant women's physical activity engagement, and ultimately enhancing their health and wellness throughout pregnancy.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of the Babol University of Medical Sciences (Code: IR.MUBABOL.HRI.REC.1401.238). During this study’s quantitative and qualitative stages, participants must provide written
informed consent.
Funding
This research was supported financially by Babol University of Medical Sciences (Grant No.: 724134896).
Authors' contributions
Writing the original draft: Fereshteh Behmanesh and Romina Fili; Review and editing: Sana Nazmi, Leila Amiri Farahani, Atefeh Omrani and Hossein-Ali Nikbakht; Conceptualization, study design and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank Vice-Chancellor for Research and Technology, Babol University of Medical Sciences for the financial support and Clinical Research Development Unit of Shahid Yahyanezhad Hospital.
References
Amiri-Farahani, L., et al., 2021. Development and psychometric testing of the ‘barriers to physical activity during pregnancy scale’ (BPAPS). BMC Public Health, 21, pp. 1483.[DOI:10.1186/s12889-021-11511-3] [PMID] [PMCID]
Azizi, M., et al., 2021. Fear of childbirth in Iran: A systematic review of psychological intervention research. International Journal of Reproductive BioMedicine, 19(5), pp. 401–20.[DOI:10.18502/ijrm.v19i5.9250] [PMCID]
Bauer, C., et al., 2018. Reasons, motivational factors, and perceived personal barriers to engagement in physical activity during pregnancy vary within the BMI classes: The Prenatal Prevention Project Germany. Journal of Physical Activity and Health, 15(3), pp. 204-11. [DOI:10.1123/jpah.2016-0563] [PMID]
Coll, C. V., et al., 2017. Perceived barriers to leisure-time physical activity during pregnancy: A literature review of quantitative and qualitative evidence. Journal of Science and Medicine in Sport, 20(1), pp. 17-25. [DOI:10.1016/j.jsams.2016.06.007] [PMID]
Connelly, M., et al., 2015. Modifiable barriers to leisure-time physical activity during pregnancy: A qualitative study investigating first time mother’s views and experiences. BMC Pregnancy and Childbirth, 15, pp. 100. [DOI:10.1186/s12884-015-0529-9] [PMID] [PMCID]
Connolly, C. P., Feltz, D. L. & Pivarnik, J. M., 2014. Overcoming barriers to physical activity during pregnancy and the postpartum period: The potential impact of social support. Kinesiology Review, 3(2), pp. 135-48. [DOI:10.1123/kr.2013-0009]
Cresswell, J. W. & Plano Clark, V. L., 2011. Designing and conducting: Mixed methods research. California: Sage. [Link]
Dolatabadi, Z., et al., 2022. Barriers to physical activity in pregnant women living in Iran and its predictors: A cross sectional study. BMC Pregnancy and Childbirth, 22, pp. 815. [DOI:10.1186/s12884-022-05124-w] [PMID] [PMCID]
Enworo, O. C., 2023. Application of Guba and Lincoln’s parallel criteria to assess trustworthiness of qualitative research on indigenous social protection systems. Qualitative Research Journal, 23(4), pp. 372-84. [DOI:10.1108/QRJ-08-2022-0116]
Evenson, K. R. & Bradley, C. B., 2010. Beliefs about exercise and physical activity among pregnant women. Patient Education and Counseling, 79(1), pp. 124–9. [DOI:10.1016/j.pec.2009.07.028] [PMID] [PMCID]
Flannery, C., et al., 2018. Enablers and barriers to physical activity in overweight and obese pregnant women: an analysis informed by the theoretical domains framework and COM-B model. BMC Pregnancy and Childbirth, 18, pp. 178. [DOI:10.1186/s12884-018-1816-z] [PMID] [PMCID]
Graneheim, U. H. & Lundman, B., 2004. Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Education Today, 24(2), pp. 105-12. [PMID]
Guelfi, K. J., et al., 2015. A comparison of beliefs about exercise during pregnancy between Chinese and Australian pregnant women. BMC Pregnancy and Childbirth, 15, pp. 345. [DOI:10.1186/s12884-015-0734-6] [PMID] [PMCID]
Harrison, A. L., et al., 2018. Attitudes, barriers and enablers to physical activity in pregnant women: A systematic review. Journal of Physiotherapy, 64(1), pp. 24-32. [DOI:10.1016/j.jphys.2017.11.012] [PMID]
Hsiung, Y., et al., 2021. Moving for My Baby!” Motivators and perceived barriers to facilitate readiness for physical activity during pregnancy among obese and overweight women of urban areas in Northern Taiwan. International Journal of Environmental Research and Public Health, 18(10), pp. 5275. [DOI:10.3390/ijerph18105275] [PMID] [PMCID]
Johonson, J, L., Adkins, D. & Chauvin, SH., 2020. A review of the quality indicators of rigor in qualitative research. American Journal of Pharmaceutical Education, 84(1), pp. 7120. [DOI:10.5688/ajpe7120] [PMID] [PMCID]
Meah, V. L., et al., 2021. Physical activity behaviors and barriers in multifetal pregnancy: What to expect when you’re expecting more. International Journal of Environmental Research and Public Health, 18(8), pp. 3907. [DOI:10.3390/ijerph18083907] [PMID] [PMCID]
Misan, N., et al., 2022. Do women play sports while pregnant? Ginekologia Polska, 93(9), pp. 710-5. [PMID]
Nulty, D. D., 2008. The adequacy of response rates to online and paper surveys: What can be done? Assessment & Evaluation in Higher Education, 33(3), pp. 301-14. [DOI:10.1080/02602930701293231]
Okafor, U. B. & Ter Goon, D., 2022. Uncovering barriers to prenatal physical activity and exercise among South African Pregnant Women: A cross-sectional, mixed-method analysis. Frontiers in Public Health, 10, pp. 697386. [DOI:10.3389/fpubh.2022.697386] [PMID] [PMCID]
Rafiei, M., et al., 2018. Prevalence, causes, and complications of cesarean delivery in Iran: A systematic review and meta-analysis. International Journal of Reproductive Biomedicine, 16(4), pp. 221-34. [PMID]
Rahimi, S. & Seyyed Rasouli, E., 2005. [Examining the knowledge and performance of pregnant women regarding exercise during pregnancy (Persian)]. Iranian Nursing Journal, 17(40), pp. 6-10. [Link]
Santos, P. C., et al., 2014. Impact of compliance with different guidelines on physical activity during pregnancy and perceived barriers to leisure physical activity. Journal of Sports Sciences, 32(14), pp. 1398-1408. [DOI:10.1080/02640414.2014.893369]
Shakibzadeh, E., et al., 2020. [The effect of educational intervention on self-efficacy, knowledge of benefits and safety tips of physical activity among pregnant women (Persian)]. Razi Journal of Medical Sciences, 26(11), pp. 98-111. [Link]
Subedi, D., 2016. Explanatory sequential mixed method design as the third research community of knowledge claim. American Journal of Educational Research, 4(7), pp. 570-7. [Link]
Type of Study: Research |
Subject:
Special
Received: 2023/09/3 | Accepted: 2024/01/23 | Published: 2024/08/1
Received: 2023/09/3 | Accepted: 2024/01/23 | Published: 2024/08/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
