Tue, Aug 11, 2026
[Archive]
Volume 10, Issue 4 (Autumn 2024)
JCCNC 2024, 10(4): 277-286 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Sandhya Joseph J, Chinnathambi K. Adolescent Focused Intervention Bundle for Institutionalized Adolescents' Health Promotion: A Study Protocol. JCCNC 2024; 10 (4) :277-286
URL: http://jccnc.iums.ac.ir/article-1-592-en.html
URL: http://jccnc.iums.ac.ir/article-1-592-en.html



1- SRM College of Nursing, SRM Institute of Science and Technology, Kattankulathur, India. , jj3452@srmist.edu.in
2- SRM College of Nursing, SRM Institute of Science and Technology, Kattankulathur, India.
2- SRM College of Nursing, SRM Institute of Science and Technology, Kattankulathur, India.
Full-Text [PDF 521 kb]
(828 Downloads)
| Abstract (HTML) (2933 Views)
Full-Text: (318 Views)
Introduction
Adolescents, defined as individuals aged from 10-19, are in various stages of development and live in diverse contexts with different needs. Iron deficiency anemia (IDA) and emotional and behavioral problems (EBPs) are significant health concerns among adolescents, especially those in lower middle-income countries. These issues are particularly prevalent among adolescents in unstable family environments with inadequate parental care. During adolescence, the body's demand for iron increases due to growth and pubertal changes. However, poor dietary intake of iron can deplete iron stores, resulting in IDA (Shafiee et al., 2015; Tarasova & Chernov, 2012). Research has shown that IDA is widespread, with global prevalence rates ranging from 5% to 90%. However, lower middle-income countries face the extreme of this spectrum. Interestingly, recent studies have revealed that even boys in India have a moderately high prevalence (between 32% and 62%) of IDA. This situation makes the issue a significant public health concern in the country (Srivastava et al., 2022; Upadhye & Upadhye, 2017).
Iron deficiency persists from childhood through adolescence and can adversely affect cognitive ability and behavior. Several studies have suggested a link between iron deficiency and EBPs (Mesías et al., 2013; Chen et al., 2013; Kim & Wessling-Resnick, 2014). However, other research studies indicate that factors such as poor parental support and insufficient familial communication can also contribute to these problems (Jilek et al., 2022). Globally, the prevalence of EBPs among adolescents varies between 3.8% and 52%. This prevalence is consistent with findings from studies on adolescent tribal children in India (Edlina et al., 2020). Despite the profound implications of these health issues, research on those living in children's houses is limited. However, the available studies indicate significant variation in the co-occurrence of IDA and EBPs in these populations (DeLacey et al., 2020).
Addressing this health issue is complicated by several barriers. For example, studies on iron supplementation programs have highlighted challenges, such as interpersonal, intrapersonal, and sociodemographic factors affecting adherence to iron pills (Gosdin et al., 2020). Furthermore, while iron-rich foods and fortifications have been recommended, access to these resources can be limited because the bioavailable iron-rich foods are often animal-based and either expensive or minimally consumed due to cultural restrictions (Mantadakis, 2020; Nath Agarwal, 2020). However, certain plant-based foods, such as moringa leaves (28 mg/%), ground nuts (4.58 mg/%), millets (the pearl millets 5-11 mg/% and finger millets 3-5.2 mg/%) have been identified as excellent sources of bioavailable iron (Arya et al., 2016; Anitha et al., 2021; Patil et al., 2023; Singh & Raghuvanshi, 2012). Supplementing bioavailable iron from natural sources addresses the issue of iron deficiency and may add value to the routine iron pill supplementation.
The second issue addressed in this study protocol is EBPs, which commonly affect adolescent health. Certain research evidence claims that combining mindfulness and life skills training reduces EBPs and increases resilience (Huang et al., 2020). However, meticulous planning for combining interventions and delivering them is challenging in the context of adolescent health promotion (Salam et al., 2016). World Health Organization (WHO) report on global accelerated action for the health of adolescents (AA-HA!) proposed that the effectiveness of adolescent health interventions is more productive if they are adolescent-specific and planned comprehensively to include subpopulations (WHO, 2017). Despite many studies on this topic, few are conducted rigorously in the middle-income countries (Mohan Srivastava, 2016). An ideal delivery platform that can augment the coverage of proven adolescent health-specific interventions with a divergent approach may facilitate adolescent health promotion. Also, it may provide an opportunity to reach hard-to-reach and disadvantaged subpopulations of those living in child care institutions (CCIs).
Adolescent-focused intervention bundle (AFIB)
Considering the wide range of interventions available for promoting adolescent health and identifying institutionalized adolescents as more susceptible, an intervention bundle will be developed to supplement Moringa Amla millet bars, life skill training, and mindful mandala art therapy. These interventions aim to enhance hematological parameters by preserving iron stores, decreasing emotional and behavioral issues, and enhancing resilience. The primary focus is on adolescents living in vulnerable situations, focusing on their physical and psychological well-being. This intervention is called the AFIB. A bundle is two or three evidence-based interventions grouped to impact a single yet complex problem. Here, the bundle aims to supply the iron needed to maintain optimum hematological parameters to manage anemia, and combined life skill training and mindful mandala art therapy are supposed to help build resilience and lower the occurrence of emotional and behavioral disorders. This intervention is adolescent-focused since the age group chosen has a specific need for preserving the optimum iron stores for sound mental and social health, for their multidimensional developmental needs in relevance to their EBPs and anemic status.
Study objectives
The study will determine if AFIB improves the hematological parameters, including hemoglobin (HB), hematocrit (HCT), mean corpuscular volume (MCV), mean corpuscular HB (MCH), mean corpuscular HB concentration (MCHC), red cell distribution width (RDW) indicative of iron sufficiency. Also, we will assess whether AFIB improves the Connor-Davidson resilience scale (CD-RISC) score and reduces EBPs by checking the strength and difficulties questionnaire (SDQ) score. Finally, we see if AFIB impacts adolescent health promotion by checking biological growth parameters, including weight, height, mid upper arm circumference (MUAC), body mass index (BMI), and life skill efficacy.
Materials and Methods
Study design
It is a feasibility randomized control trial. AFIB will be used as the intervention in this study.
Study overview
Three interventions are combined and will be delivered simultaneously, aiming to improve adolescent health in terms of IDA and EBPs.
Nutritional supplementation intervention
This supplementation includes a millet-based moringa Amla iron-rich bar developed by the researcher, which will be tested for nutritional values and adolescent sensory acceptance. Each day, 30 g will be given to the participants for 90 days (12 weeks).
Mindful mandala art therapy
This therapy refers to coloring pre-filled sheets with colored pencils while listening to mindful music. There will be 12 sessions of mindful art therapy lasting for 30-45 minutes once a week for 90 days (12 weeks).
Life skill training intervention
This training refers to core life skills such as thinking, emotional, and social skills with a subcategory of 10 skills. There will be 12 life skill training sessions lasting 30-45 minutes once a week for 90 days (12 weeks).
Sample size
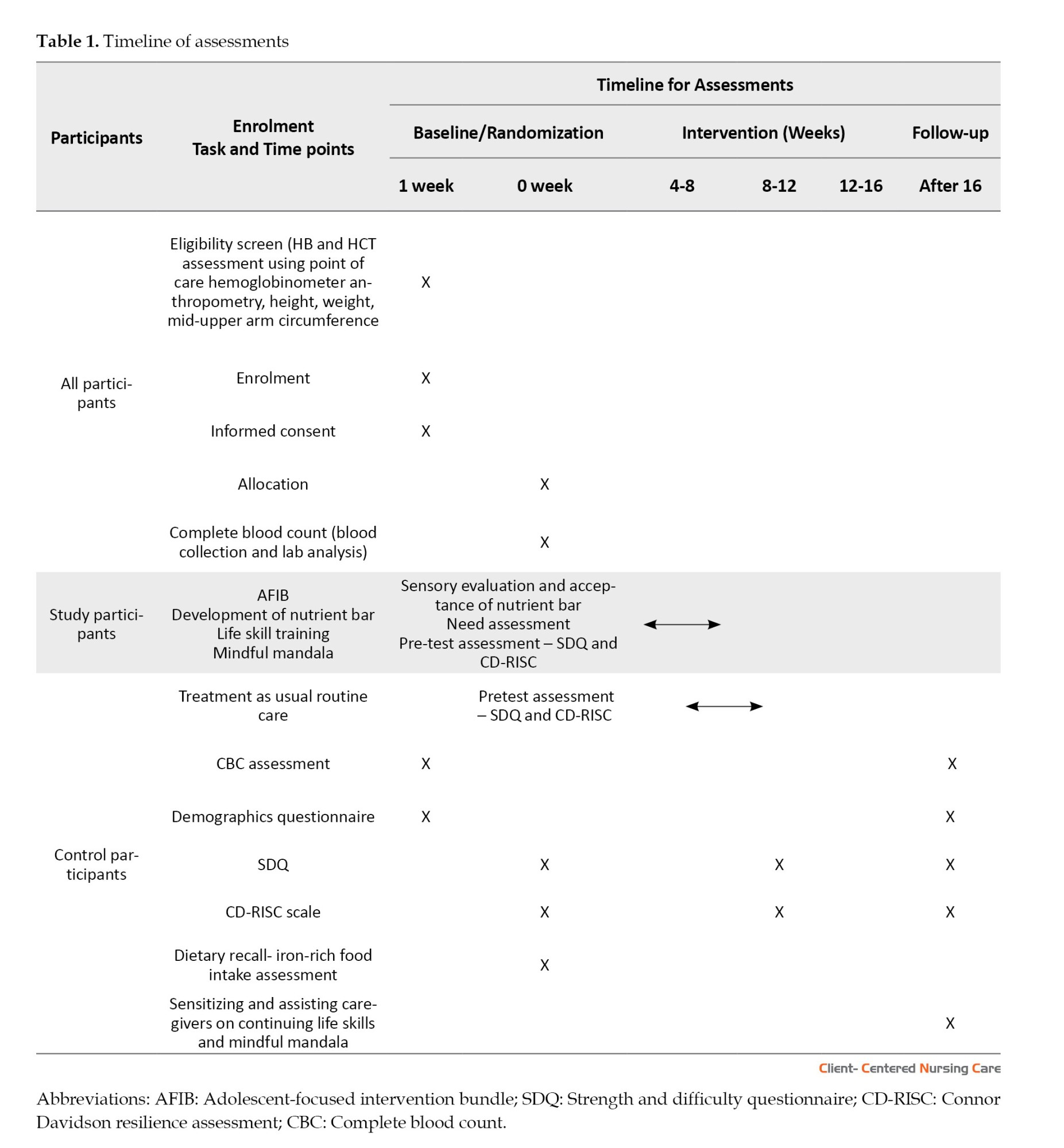
Based on data from the highest-quality studies available on Moringa’s effect on hematological parameters (Loa et al., 2021) iron, and vitamin C that potentially prevent anemia more common in pregnant women. In the manufacture of cookies that are substituted Moringa Oleifera leaf flour substitution, 40% obtained Fe levels 22.68 ppm so that it can be developed to prevent anemia. The purpose of this research is to know the effect of giving biscuits (cookies, we calculated the sample size for 80% power at a 95% confidence interval. Additionally, data from studies available on combined interventions regarding the effects of mindfulness and life skill training on EBPs are utilized for sample size calculation (Hosseinian & Nooripour, 2019). According to this, 98 participants would be needed to see an effect as they observed after 8 weeks with Moringa snack supplementation. We will increase the sample size to the maximum estimated because of the possibility of sample attrition and a much smaller effect. Will be 120 participants equally assigned to study (n=60) and control (n=60) groups. Table 1 shows the timeline of the study process.
Study setting
Study activities will be conducted in selected CCIs registered under the juvenile justice act (JJAct) and the directorate of social defence. The institutions located at Kodungaiyur, Vyasarpadi, Perambur, Alandhur, Periamed, Pallavaram, Park Town, Mannivakkam, and Erukanchery in the State of Tamil Nadu will be included in the study. This region was selected after a survey that showed that there are many childcare institutions in Tamil Nadu compared to other states of India and that the number of children in these institutions is increasing.
Randomization
Selected childcare institutions that give residential care for healthy adolescents aged 10-17 years, both boys and or girls with conjunctival pallor as identified by the researcher, will be screened for anemic status using point-of-care (POC) equipment (Mission Hemoglobin) by finger prick capillary sampling. The centers with a mean HB of 9.0±1.5 g/dL will be identified and included in the trial. Proportional stratified random sampling will be used to enroll the study participants at study and control centers. Randomization will be stratified by the regions of Chennai (South, North, Central, and Greater/Expanded Chennai), and random allocation will be done by a statistician who will be blind to center identity and independent of the researcher.
Recruitment and enrolment
Without physiological or mental impairments and with HB ranging from 9.0 to 12.9 g/dL who reside at a childcare institution for more than a year and intend to stay for the next 3 months, male or female adolescents aged 10-17 years will be automatically randomized into the control or study group based on the enrolment site. Utilizing four different centers for control and study groups will help prevent the “spillover effect” of the intervention bundle with non-intervention centers. Consent will be obtained from the childcare institutions’ guardians or superintendents. Adolescents who are on treatment for health problems, girls with menstrual irregularities, on other nutrient supplements for iron deficiency, refusing to take supplements, on psychotherapy, and life skill training will be excluded from the study. The researcher will enroll the participants with assent in the regional language (Tamil) or English, collect demographic details, assess anthropometric measurements with a stadiometer, digital weighing scale, and MUAC tape, and collect blood samples for complete blood count (CBC). An undertaking will be given for collected blood samples to be tested only in a specified hospital on the same day for analysis. Resilience will be assessed using CD-RISC (Connor & Davidson, 2003), and the adolescents will rate 25 statements. The EBPs will be evaluated using SDQ (Goodman, 1997), comprising 25 questions rated by wardens in childcare institutions. The data will be uploaded later using Google Forms. Based on the previous week’s menu, the food frequency questionnaire for iron-rich foods will be completed for each of eight centers. A dropout rate of 10% is expected, and new participants will be enrolled if anyone withdraws from the study within 2 weeks.
Description of the tools
The demographic profile of the participants includes age, gender, stage of adolescence, type of orphanhood, type of school, class, and place of residence, as well as birth before admission to the CCI.
CCIs are characterized by 3 items, including their location, financial support, and the type of gender-based admissions into the CCI. Anthropometric assessment (weight, height, MUAC), BMI, height for age (HAZ), and BMI for age (BAZ) scores will be calculated using the WHO software Anthro Plus, version 1.0.4 (x86) (updated September 17, 2014). The type of pallor will also be determined. The digital weighing scale, stadiometer, and inch tape will be validated and uniformly used for all the samples.
Hematological parameters, including Hb and HCT, are measured by a POC device (Mission® Plus Hb). This outcome is standardized and assessed for errors. The functions of the portable Hb/HCT meter and the hematology analyzer are standardized daily based on the manufacturers’ recommendations (Mission HB).
CD-RISC 25
The CD-RISC is a standardized questionnaire consisting of 25 self-rated items (Connor & Davidson, 2003) to measure resilience in healthy individuals, as well as those with posttraumatic disorders, depression, and generalized anxiety. The questionnaire measures resilience on a 5-point Likert scale: 0=not true at all; 1=rarely true; 2=sometimes true; 3=often true; and 4=true nearly all the time. It includes statements that describe various aspects of resilience. It assesses hardiness (commitment, challenge, and control), coping, adaptability/flexibility, meaningfulness/purpose, optimism, regulation of emotion and cognition, and self-efficacy. The individual is directed to respond to the statements based on situations concerning the previous months, understanding that the problem has not arisen. The resilience is assessed at the beginning and end of a 12-week program. The researcher offers clarification to help adolescents understand the context of the situation/statement. The interview takes between 10 to 15 minutes for individual participants to complete. The total score is calculated by adding up all 25 items, ranging from 0 to 100. A higher score indicates greater resilience, while a lower score indicates less resilience. In previous studies conducted in India, the mean score on the CD-RISC 25 ranged from 60.4 to 71.4, with a standard deviation 15.6 (Connor & Davidson, 2003). The CD-RISC reliability was also confirmed (0.89) in a study on Indian students (Singh & Choubisa, 2009). Experts purchased and validated the authorized Tamil version of the tool. The reliability index of equivalence correlation coefficient was r=0.82 and r= 0.87, respectively.
The scores are categorized based on this mean score (low: 0-59; high: 60-100). Categorizing resilience levels is done with the consensus of the author-Connor and Davidson- and according to previous studies (Sidheek et al., 2017).
Strength and difficulty questionnaire (SDQ)
SDQ was developed by Professor Robert Goodman (Goodman, 1997). It is one of the most widely used screening tools for children aged 2 to 18. The questionnaire consists of 25 equally distributed across five scales, measuring emotional symptoms, conduct issues, hyperactivity-inattention, peer problems, and prosocial behavior. SDQ is a reliable tool to assess young children’s EBPs in community settings (Dahlberg et al., 2020). The researcher evaluates the emotional and behavioral difficulties of the participants twice, once at the beginning of the program (baseline) and then again at the end (endline) of a 12-week program. It will be completed by the participant’s guardian from the childcare institution. The questionnaire requires the guardian to indicate whether each item is “not true=0)”, “somewhat true=1”, or “certainly true=2” based on the child’s behavior over the last one to six months. For each of the 5 scales, the score can range from 0 to 10 if all items are completed. The total difficulties score is created by adding the scores from all the scales except the prosocial scale. A score of 0 is the best result in the emotional, conduct, hyperactivity, and peer relationship fields. The normal prosocial field score ranges from 6 to 10; it is abnormal if the score ranges from 0 to 4. The validity and reliability of the scale have been proven (Mieloo et al., 2012) and will be reassessed in our study.
Dietary profile
The dietary intake of iron is calculated based on the frequency of consuming iron-rich food supplied by the daily menu in the CCIs against the skipping meal data obtained from the individual participants. It includes skipping breakfast, snacks, lunch, and dinner. The average iron intake is calculated as a dietary variable.
Study intervention
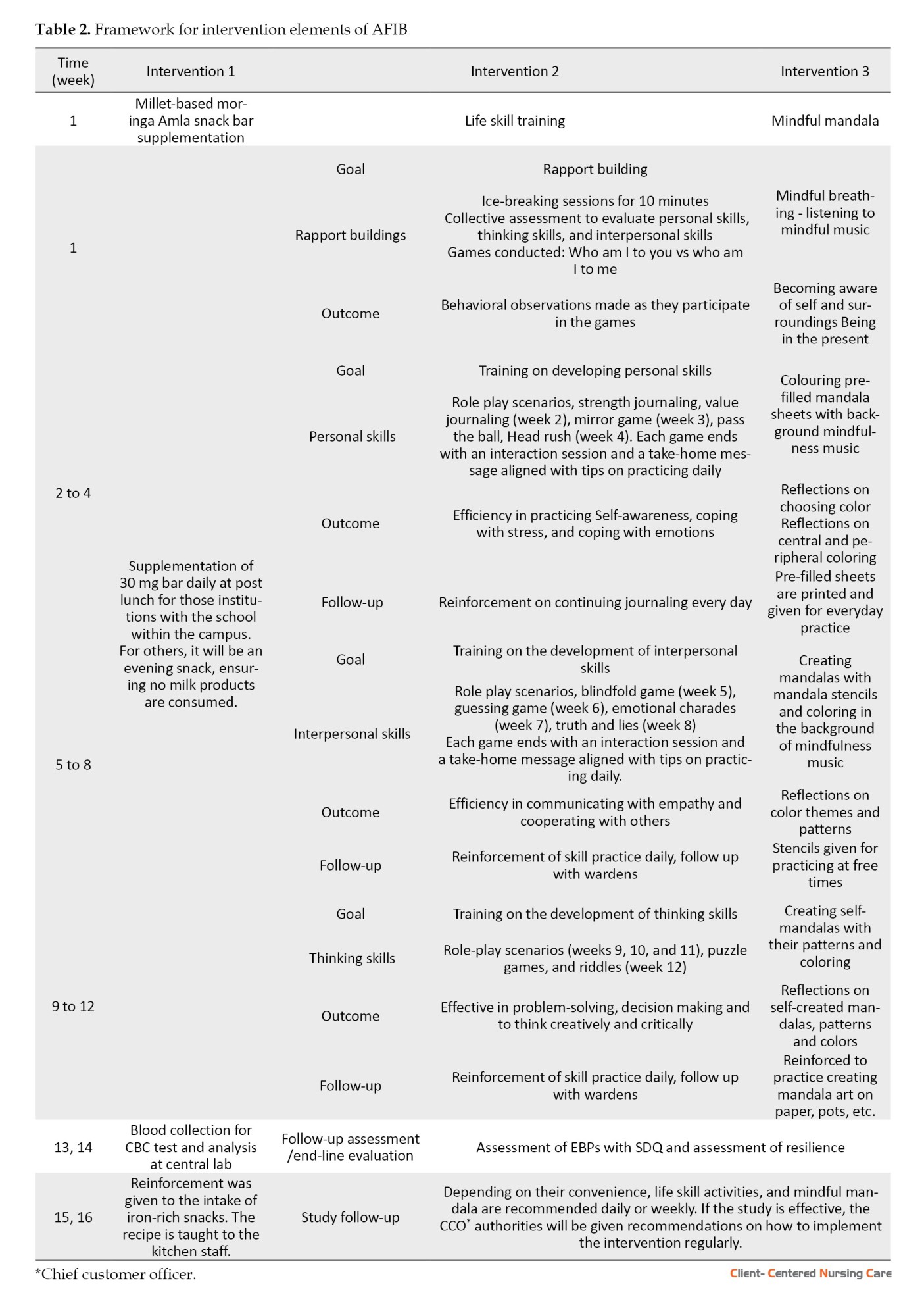
All the study participants will receive 30 g of moringa iron-rich millet snack bar once daily in the evening every day for 90 days. The center’s participants and wardens are instructed not to consume food products like milk that interfere with iron absorption. The researcher prepares the Moringa millet bars fresh at the site, wraps them in butter paper packs, and stores them in airtight containers to be stocked for 4 days of use. The process continues for 90 days. The study participants will be dewormed as per the deworming protocol. The study participants in their respective institutions will be grouped for group sessions on need-based life skill training once a week, followed by mindful mandala art therapy sessions for 60 minutes and continued for 12 consecutive weeks, alongside daily nutritional supplementation with bar. The researcher delivers 12 interactive need-based life skill training sessions using team activities lasting 45 minutes after school hours and off days. Mindful mandala will be delivered through a 5-minute mindful breathing exercise followed by a 25-minute session on coloring pre-filled mandala sheets using colored pencils in the background mindfulness music played on a speaker. For the next 4 weeks, the researcher will make the participants create mandalas using stencils. For the last 4 weeks, the study participants will be trained to doodle (simple drawings that can have a specific symbolic meaning or consist of random, abstract lines or shapes) and, as a result, create their mandala based on the feeling of “How I am here and now”. The total intervention period will be 12 weeks. For the control group, the warden and the participants in the CCIs are given only the snacks per the respective center’s menu as standard care, and group counseling sessions are provided as standard care. Both the study and control groups are recommended to follow Anemia Mukth Bharath guidelines on iron supplementation of two iron–folic–acid (IFA) tablets (each with 60 mg elemental iron and 500 mcg folic acid), once daily for 3 months, orally after meals. The intervention summary is shown in Table 2.
Blinding
This study employs a single-blinded design, where the participants will be blinded to their study and control group assignments. The CCIs are located apart, and their nature of participation in the research (study or control) makes blinding feasible and reduces “spillover effects” as well. Blinding will be implemented to minimize potential bias or influence from the participant’s knowledge of their treatment group.
Data collection and analysis
A structured questionnaire will collect sociodemographic data in Google Form by the researcher herself. The dietary assessment uses the food frequency table for iron-rich food consumption using the standard dietary guidelines prescribed by the nutrition handbook of India 2021 (RDA & EAR for Indians, 2020).
Blood samples will be collected with 2-mL disposable syringes after cleaning the sites with a commercial alcohol swab and sterile dry cotton. The veins of the antecubital fossa will be chosen for blood collection. The blood samples are collected in EDTA (ethylenediaminetetraacetic acid) tubes. The collected samples are transferred according to the protocols of the central laboratory of SRM Medical College Hospitals and Research Center within 2 hours after blood collection. The blood will be analyzed in a high-quality, fully automated 5-part hematology analyzer. The reports will be obtained on the same day of analysis.
Children and wardens will complete the CD-RISC scale and SDQ, respectively. It will be done by conducting structured interviews with the researcher using Google Forms. This procedure is done after enrolment but before allocation to treatment and control groups. The post-intervention evaluation will be done at the end of the 12-week study period. Anthropometric measurements will be assessed at baseline and end-line.
Statistical analysis
We will assess the normal data distribution using the Kolmogorov-Smirnov test and ggplot. Continuous variables will be presented as the mean, standard deviation, and median, whereas categorical variables will be presented as percentages/proportions. Statistical analysis will include univariate and multivariate analysis for primary and secondary outcomes assessed as a delta change from baseline per individual and group and compared with controls. We will use the Pearson correlation for relationships between continuous variables, Pearson Chi-square and Fisher exact test for associations between binary variables, and independent samples t-test for associations between binary and continuous variables. We will also utilize paired t-test as needed. All enrolled participants will be included in the analysis, excluding those lost to follow-up. Appropriate adjustments for multiple comparisons will be used for all statistical tests.
Discussion
The AFIB aims to provide new data supporting the use of a unique snack bar supplying 57 mg of iron made from millet, Moringa, and Amla ingredients (100 g of Moringa Amla snack bar contains 57 mg of iron) as a supplement intervention along with the weekly iron supplementation program in preventing anemia. It seeks to provide iron supplementation in a snack more appealing to adolescents than routine elemental iron therapy (60 mg). The study incorporates life skill training intervention, mindful mandala art therapy, and snack bar supplements in a comprehensive strategy at the CCIs. The study design seeks to identify a significant difference in the selected health promotion outcomes among adolescents in their institutional settings. This study differs from previous ones as it utilizes a bundle approach to select evidence-based interventions in its design. The study includes an initial evaluation of HB levels in adolescents residing in selected CCIs in Chennai and surrounding areas such as Chengalpattu and Madhavaram.
Conclusion
In conclusion, the study protocol for evaluating the effectiveness of an intervention bundle focused on adolescents in CCIs, specifically in terms of anemia, emotional-behavioral problems, and improving resilience. This research can potentially address the complex issues and challenges that at-risk population living in CCIs encounter. Significant improvement in emotional, physical, and mental well-being is expected upon strategic implementation of this bundle. Through a rigorous research methodology and a comprehensive analysis of the data collected, this study aims to offer valuable insights into enhancing the overall quality of care and support provided to adolescents in childcare institutional settings. Eventually, the findings have the potential to inform evidence-based practices, thus leading to more effective interventions and better outcomes for adolescents in similar contexts worldwide.
The challenge and limitation of the study is that it cannot assess the efficacy of AFIB directly due to the absence of a placebo snack or placebo for mindful mandala art and life skill training. The study examines the effectiveness of AFIB compared with standard care practices only. Efficacy trials involving placebo have the potential to yield compelling evidence of enhanced efficacy.
Research implications and limitations
Adolescents residing in CCIs are susceptible to physical and mental health issues. Specifically, anemia, EBPs, and poor resilience are notably prevalent at a comparatively higher rate. School health nurses serve as the primary personnel in identifying learning disabilities, depression, and malnutrition among school children based on the state policy and protocol. However, those residing in CCIs require a dual focus due to inconsistent caretakers and collective care giving by the wardens. The individual attention received by those in family care settings is compromised for those residing in childcare institutions. The present comprehensive approach attempts to address the widespread issue of anemia, often combined with malnutrition, as well as the EBPs that are more common among such adolescents. This approach consists of evidence-based interventions, including Moringa iron-rich snack supplementation, life skill training, and mindful mandala, which have individually proven effective in addressing anemia, emotional, and behavioral problems, and enhancing resilience. These interventions are often tested individually in school settings. However, the bundle approach tackles these issues holistically and simultaneously within this study design. The evidence gathered from the randomized control trial will provide insights into the prevalence of anemia and emotional-behavioral problems in the selected settings included in the study. This study uses POC methods to conduct anemia screening in a larger sample. The recruited sample is then subjected to laboratory testing, specifically a CBC, to detect IDA based on red blood cell indices. The correlation between POC measures and laboratory measures will help identify the effectiveness of employing POC methods for screening purposes within the community. Furthermore, the study attempts to derive a conceptual mapping of emotional behavioral problems, life skills, mindfulness, and resilience from the study findings.
Ethical Considerations
Compliance with ethical guidelines
This study is registered at the Clinical Trial Registry India (Code: CTRI/2023/10/059027). Ethical approval was obtained from the Institutional Review Board and Institutional Ethical Committee under SRM Medical College Hospital and Research Centre (Code: 8372/IEC/ 2022). Written informed consent and required permissions are obtained from all the participants and responsible persons before the study procedures begin.
Funding
This paper is an output of the cross-sectional survey among institutionalized adolescents in Chennai conducted as part of PhD dissertation of Joy Sandhya Joseph by a research scholar at SRM College of Nursing in SRM Institute of Science and Technology (SRMIST).
Authors' contributions
Conceptualization: Joy Sandhya Joseph; Supervision: Kanniammal Chinnathambi; Methodology: Joy Sandhya Joseph and Kanniammal Chinnathambi; Investigation: Joy Sandhya Joseph; Writing: Joy Sandhya Joseph; Review & Editing: Kanniammal Chinnathambi; Data collection: Joy Sandhya Joseph and Kanniammal Chinnathambi; Data analysis: Joy Sandhya Joseph and Kanniammal Chinnathambi.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
We are grateful to Ms, Vania Olivia, UK Nurse Researcher, for giving expertise in the field of study protocol framing.
References
Adolescents, defined as individuals aged from 10-19, are in various stages of development and live in diverse contexts with different needs. Iron deficiency anemia (IDA) and emotional and behavioral problems (EBPs) are significant health concerns among adolescents, especially those in lower middle-income countries. These issues are particularly prevalent among adolescents in unstable family environments with inadequate parental care. During adolescence, the body's demand for iron increases due to growth and pubertal changes. However, poor dietary intake of iron can deplete iron stores, resulting in IDA (Shafiee et al., 2015; Tarasova & Chernov, 2012). Research has shown that IDA is widespread, with global prevalence rates ranging from 5% to 90%. However, lower middle-income countries face the extreme of this spectrum. Interestingly, recent studies have revealed that even boys in India have a moderately high prevalence (between 32% and 62%) of IDA. This situation makes the issue a significant public health concern in the country (Srivastava et al., 2022; Upadhye & Upadhye, 2017).
Iron deficiency persists from childhood through adolescence and can adversely affect cognitive ability and behavior. Several studies have suggested a link between iron deficiency and EBPs (Mesías et al., 2013; Chen et al., 2013; Kim & Wessling-Resnick, 2014). However, other research studies indicate that factors such as poor parental support and insufficient familial communication can also contribute to these problems (Jilek et al., 2022). Globally, the prevalence of EBPs among adolescents varies between 3.8% and 52%. This prevalence is consistent with findings from studies on adolescent tribal children in India (Edlina et al., 2020). Despite the profound implications of these health issues, research on those living in children's houses is limited. However, the available studies indicate significant variation in the co-occurrence of IDA and EBPs in these populations (DeLacey et al., 2020).
Addressing this health issue is complicated by several barriers. For example, studies on iron supplementation programs have highlighted challenges, such as interpersonal, intrapersonal, and sociodemographic factors affecting adherence to iron pills (Gosdin et al., 2020). Furthermore, while iron-rich foods and fortifications have been recommended, access to these resources can be limited because the bioavailable iron-rich foods are often animal-based and either expensive or minimally consumed due to cultural restrictions (Mantadakis, 2020; Nath Agarwal, 2020). However, certain plant-based foods, such as moringa leaves (28 mg/%), ground nuts (4.58 mg/%), millets (the pearl millets 5-11 mg/% and finger millets 3-5.2 mg/%) have been identified as excellent sources of bioavailable iron (Arya et al., 2016; Anitha et al., 2021; Patil et al., 2023; Singh & Raghuvanshi, 2012). Supplementing bioavailable iron from natural sources addresses the issue of iron deficiency and may add value to the routine iron pill supplementation.
The second issue addressed in this study protocol is EBPs, which commonly affect adolescent health. Certain research evidence claims that combining mindfulness and life skills training reduces EBPs and increases resilience (Huang et al., 2020). However, meticulous planning for combining interventions and delivering them is challenging in the context of adolescent health promotion (Salam et al., 2016). World Health Organization (WHO) report on global accelerated action for the health of adolescents (AA-HA!) proposed that the effectiveness of adolescent health interventions is more productive if they are adolescent-specific and planned comprehensively to include subpopulations (WHO, 2017). Despite many studies on this topic, few are conducted rigorously in the middle-income countries (Mohan Srivastava, 2016). An ideal delivery platform that can augment the coverage of proven adolescent health-specific interventions with a divergent approach may facilitate adolescent health promotion. Also, it may provide an opportunity to reach hard-to-reach and disadvantaged subpopulations of those living in child care institutions (CCIs).
Adolescent-focused intervention bundle (AFIB)
Considering the wide range of interventions available for promoting adolescent health and identifying institutionalized adolescents as more susceptible, an intervention bundle will be developed to supplement Moringa Amla millet bars, life skill training, and mindful mandala art therapy. These interventions aim to enhance hematological parameters by preserving iron stores, decreasing emotional and behavioral issues, and enhancing resilience. The primary focus is on adolescents living in vulnerable situations, focusing on their physical and psychological well-being. This intervention is called the AFIB. A bundle is two or three evidence-based interventions grouped to impact a single yet complex problem. Here, the bundle aims to supply the iron needed to maintain optimum hematological parameters to manage anemia, and combined life skill training and mindful mandala art therapy are supposed to help build resilience and lower the occurrence of emotional and behavioral disorders. This intervention is adolescent-focused since the age group chosen has a specific need for preserving the optimum iron stores for sound mental and social health, for their multidimensional developmental needs in relevance to their EBPs and anemic status.
Study objectives
The study will determine if AFIB improves the hematological parameters, including hemoglobin (HB), hematocrit (HCT), mean corpuscular volume (MCV), mean corpuscular HB (MCH), mean corpuscular HB concentration (MCHC), red cell distribution width (RDW) indicative of iron sufficiency. Also, we will assess whether AFIB improves the Connor-Davidson resilience scale (CD-RISC) score and reduces EBPs by checking the strength and difficulties questionnaire (SDQ) score. Finally, we see if AFIB impacts adolescent health promotion by checking biological growth parameters, including weight, height, mid upper arm circumference (MUAC), body mass index (BMI), and life skill efficacy.
Materials and Methods
Study design
It is a feasibility randomized control trial. AFIB will be used as the intervention in this study.
Study overview
Three interventions are combined and will be delivered simultaneously, aiming to improve adolescent health in terms of IDA and EBPs.
Nutritional supplementation intervention
This supplementation includes a millet-based moringa Amla iron-rich bar developed by the researcher, which will be tested for nutritional values and adolescent sensory acceptance. Each day, 30 g will be given to the participants for 90 days (12 weeks).
Mindful mandala art therapy
This therapy refers to coloring pre-filled sheets with colored pencils while listening to mindful music. There will be 12 sessions of mindful art therapy lasting for 30-45 minutes once a week for 90 days (12 weeks).
Life skill training intervention
This training refers to core life skills such as thinking, emotional, and social skills with a subcategory of 10 skills. There will be 12 life skill training sessions lasting 30-45 minutes once a week for 90 days (12 weeks).
Sample size
Based on data from the highest-quality studies available on Moringa’s effect on hematological parameters (Loa et al., 2021) iron, and vitamin C that potentially prevent anemia more common in pregnant women. In the manufacture of cookies that are substituted Moringa Oleifera leaf flour substitution, 40% obtained Fe levels 22.68 ppm so that it can be developed to prevent anemia. The purpose of this research is to know the effect of giving biscuits (cookies, we calculated the sample size for 80% power at a 95% confidence interval. Additionally, data from studies available on combined interventions regarding the effects of mindfulness and life skill training on EBPs are utilized for sample size calculation (Hosseinian & Nooripour, 2019). According to this, 98 participants would be needed to see an effect as they observed after 8 weeks with Moringa snack supplementation. We will increase the sample size to the maximum estimated because of the possibility of sample attrition and a much smaller effect. Will be 120 participants equally assigned to study (n=60) and control (n=60) groups. Table 1 shows the timeline of the study process.
Study setting
Study activities will be conducted in selected CCIs registered under the juvenile justice act (JJAct) and the directorate of social defence. The institutions located at Kodungaiyur, Vyasarpadi, Perambur, Alandhur, Periamed, Pallavaram, Park Town, Mannivakkam, and Erukanchery in the State of Tamil Nadu will be included in the study. This region was selected after a survey that showed that there are many childcare institutions in Tamil Nadu compared to other states of India and that the number of children in these institutions is increasing.
Randomization
Selected childcare institutions that give residential care for healthy adolescents aged 10-17 years, both boys and or girls with conjunctival pallor as identified by the researcher, will be screened for anemic status using point-of-care (POC) equipment (Mission Hemoglobin) by finger prick capillary sampling. The centers with a mean HB of 9.0±1.5 g/dL will be identified and included in the trial. Proportional stratified random sampling will be used to enroll the study participants at study and control centers. Randomization will be stratified by the regions of Chennai (South, North, Central, and Greater/Expanded Chennai), and random allocation will be done by a statistician who will be blind to center identity and independent of the researcher.
Recruitment and enrolment
Without physiological or mental impairments and with HB ranging from 9.0 to 12.9 g/dL who reside at a childcare institution for more than a year and intend to stay for the next 3 months, male or female adolescents aged 10-17 years will be automatically randomized into the control or study group based on the enrolment site. Utilizing four different centers for control and study groups will help prevent the “spillover effect” of the intervention bundle with non-intervention centers. Consent will be obtained from the childcare institutions’ guardians or superintendents. Adolescents who are on treatment for health problems, girls with menstrual irregularities, on other nutrient supplements for iron deficiency, refusing to take supplements, on psychotherapy, and life skill training will be excluded from the study. The researcher will enroll the participants with assent in the regional language (Tamil) or English, collect demographic details, assess anthropometric measurements with a stadiometer, digital weighing scale, and MUAC tape, and collect blood samples for complete blood count (CBC). An undertaking will be given for collected blood samples to be tested only in a specified hospital on the same day for analysis. Resilience will be assessed using CD-RISC (Connor & Davidson, 2003), and the adolescents will rate 25 statements. The EBPs will be evaluated using SDQ (Goodman, 1997), comprising 25 questions rated by wardens in childcare institutions. The data will be uploaded later using Google Forms. Based on the previous week’s menu, the food frequency questionnaire for iron-rich foods will be completed for each of eight centers. A dropout rate of 10% is expected, and new participants will be enrolled if anyone withdraws from the study within 2 weeks.
Description of the tools
The demographic profile of the participants includes age, gender, stage of adolescence, type of orphanhood, type of school, class, and place of residence, as well as birth before admission to the CCI.
CCIs are characterized by 3 items, including their location, financial support, and the type of gender-based admissions into the CCI. Anthropometric assessment (weight, height, MUAC), BMI, height for age (HAZ), and BMI for age (BAZ) scores will be calculated using the WHO software Anthro Plus, version 1.0.4 (x86) (updated September 17, 2014). The type of pallor will also be determined. The digital weighing scale, stadiometer, and inch tape will be validated and uniformly used for all the samples.
Hematological parameters, including Hb and HCT, are measured by a POC device (Mission® Plus Hb). This outcome is standardized and assessed for errors. The functions of the portable Hb/HCT meter and the hematology analyzer are standardized daily based on the manufacturers’ recommendations (Mission HB).
CD-RISC 25
The CD-RISC is a standardized questionnaire consisting of 25 self-rated items (Connor & Davidson, 2003) to measure resilience in healthy individuals, as well as those with posttraumatic disorders, depression, and generalized anxiety. The questionnaire measures resilience on a 5-point Likert scale: 0=not true at all; 1=rarely true; 2=sometimes true; 3=often true; and 4=true nearly all the time. It includes statements that describe various aspects of resilience. It assesses hardiness (commitment, challenge, and control), coping, adaptability/flexibility, meaningfulness/purpose, optimism, regulation of emotion and cognition, and self-efficacy. The individual is directed to respond to the statements based on situations concerning the previous months, understanding that the problem has not arisen. The resilience is assessed at the beginning and end of a 12-week program. The researcher offers clarification to help adolescents understand the context of the situation/statement. The interview takes between 10 to 15 minutes for individual participants to complete. The total score is calculated by adding up all 25 items, ranging from 0 to 100. A higher score indicates greater resilience, while a lower score indicates less resilience. In previous studies conducted in India, the mean score on the CD-RISC 25 ranged from 60.4 to 71.4, with a standard deviation 15.6 (Connor & Davidson, 2003). The CD-RISC reliability was also confirmed (0.89) in a study on Indian students (Singh & Choubisa, 2009). Experts purchased and validated the authorized Tamil version of the tool. The reliability index of equivalence correlation coefficient was r=0.82 and r= 0.87, respectively.
The scores are categorized based on this mean score (low: 0-59; high: 60-100). Categorizing resilience levels is done with the consensus of the author-Connor and Davidson- and according to previous studies (Sidheek et al., 2017).
Strength and difficulty questionnaire (SDQ)
SDQ was developed by Professor Robert Goodman (Goodman, 1997). It is one of the most widely used screening tools for children aged 2 to 18. The questionnaire consists of 25 equally distributed across five scales, measuring emotional symptoms, conduct issues, hyperactivity-inattention, peer problems, and prosocial behavior. SDQ is a reliable tool to assess young children’s EBPs in community settings (Dahlberg et al., 2020). The researcher evaluates the emotional and behavioral difficulties of the participants twice, once at the beginning of the program (baseline) and then again at the end (endline) of a 12-week program. It will be completed by the participant’s guardian from the childcare institution. The questionnaire requires the guardian to indicate whether each item is “not true=0)”, “somewhat true=1”, or “certainly true=2” based on the child’s behavior over the last one to six months. For each of the 5 scales, the score can range from 0 to 10 if all items are completed. The total difficulties score is created by adding the scores from all the scales except the prosocial scale. A score of 0 is the best result in the emotional, conduct, hyperactivity, and peer relationship fields. The normal prosocial field score ranges from 6 to 10; it is abnormal if the score ranges from 0 to 4. The validity and reliability of the scale have been proven (Mieloo et al., 2012) and will be reassessed in our study.
Dietary profile
The dietary intake of iron is calculated based on the frequency of consuming iron-rich food supplied by the daily menu in the CCIs against the skipping meal data obtained from the individual participants. It includes skipping breakfast, snacks, lunch, and dinner. The average iron intake is calculated as a dietary variable.
Study intervention
All the study participants will receive 30 g of moringa iron-rich millet snack bar once daily in the evening every day for 90 days. The center’s participants and wardens are instructed not to consume food products like milk that interfere with iron absorption. The researcher prepares the Moringa millet bars fresh at the site, wraps them in butter paper packs, and stores them in airtight containers to be stocked for 4 days of use. The process continues for 90 days. The study participants will be dewormed as per the deworming protocol. The study participants in their respective institutions will be grouped for group sessions on need-based life skill training once a week, followed by mindful mandala art therapy sessions for 60 minutes and continued for 12 consecutive weeks, alongside daily nutritional supplementation with bar. The researcher delivers 12 interactive need-based life skill training sessions using team activities lasting 45 minutes after school hours and off days. Mindful mandala will be delivered through a 5-minute mindful breathing exercise followed by a 25-minute session on coloring pre-filled mandala sheets using colored pencils in the background mindfulness music played on a speaker. For the next 4 weeks, the researcher will make the participants create mandalas using stencils. For the last 4 weeks, the study participants will be trained to doodle (simple drawings that can have a specific symbolic meaning or consist of random, abstract lines or shapes) and, as a result, create their mandala based on the feeling of “How I am here and now”. The total intervention period will be 12 weeks. For the control group, the warden and the participants in the CCIs are given only the snacks per the respective center’s menu as standard care, and group counseling sessions are provided as standard care. Both the study and control groups are recommended to follow Anemia Mukth Bharath guidelines on iron supplementation of two iron–folic–acid (IFA) tablets (each with 60 mg elemental iron and 500 mcg folic acid), once daily for 3 months, orally after meals. The intervention summary is shown in Table 2.
Blinding
This study employs a single-blinded design, where the participants will be blinded to their study and control group assignments. The CCIs are located apart, and their nature of participation in the research (study or control) makes blinding feasible and reduces “spillover effects” as well. Blinding will be implemented to minimize potential bias or influence from the participant’s knowledge of their treatment group.
Data collection and analysis
A structured questionnaire will collect sociodemographic data in Google Form by the researcher herself. The dietary assessment uses the food frequency table for iron-rich food consumption using the standard dietary guidelines prescribed by the nutrition handbook of India 2021 (RDA & EAR for Indians, 2020).
Blood samples will be collected with 2-mL disposable syringes after cleaning the sites with a commercial alcohol swab and sterile dry cotton. The veins of the antecubital fossa will be chosen for blood collection. The blood samples are collected in EDTA (ethylenediaminetetraacetic acid) tubes. The collected samples are transferred according to the protocols of the central laboratory of SRM Medical College Hospitals and Research Center within 2 hours after blood collection. The blood will be analyzed in a high-quality, fully automated 5-part hematology analyzer. The reports will be obtained on the same day of analysis.
Children and wardens will complete the CD-RISC scale and SDQ, respectively. It will be done by conducting structured interviews with the researcher using Google Forms. This procedure is done after enrolment but before allocation to treatment and control groups. The post-intervention evaluation will be done at the end of the 12-week study period. Anthropometric measurements will be assessed at baseline and end-line.
Statistical analysis
We will assess the normal data distribution using the Kolmogorov-Smirnov test and ggplot. Continuous variables will be presented as the mean, standard deviation, and median, whereas categorical variables will be presented as percentages/proportions. Statistical analysis will include univariate and multivariate analysis for primary and secondary outcomes assessed as a delta change from baseline per individual and group and compared with controls. We will use the Pearson correlation for relationships between continuous variables, Pearson Chi-square and Fisher exact test for associations between binary variables, and independent samples t-test for associations between binary and continuous variables. We will also utilize paired t-test as needed. All enrolled participants will be included in the analysis, excluding those lost to follow-up. Appropriate adjustments for multiple comparisons will be used for all statistical tests.
Discussion
The AFIB aims to provide new data supporting the use of a unique snack bar supplying 57 mg of iron made from millet, Moringa, and Amla ingredients (100 g of Moringa Amla snack bar contains 57 mg of iron) as a supplement intervention along with the weekly iron supplementation program in preventing anemia. It seeks to provide iron supplementation in a snack more appealing to adolescents than routine elemental iron therapy (60 mg). The study incorporates life skill training intervention, mindful mandala art therapy, and snack bar supplements in a comprehensive strategy at the CCIs. The study design seeks to identify a significant difference in the selected health promotion outcomes among adolescents in their institutional settings. This study differs from previous ones as it utilizes a bundle approach to select evidence-based interventions in its design. The study includes an initial evaluation of HB levels in adolescents residing in selected CCIs in Chennai and surrounding areas such as Chengalpattu and Madhavaram.
Conclusion
In conclusion, the study protocol for evaluating the effectiveness of an intervention bundle focused on adolescents in CCIs, specifically in terms of anemia, emotional-behavioral problems, and improving resilience. This research can potentially address the complex issues and challenges that at-risk population living in CCIs encounter. Significant improvement in emotional, physical, and mental well-being is expected upon strategic implementation of this bundle. Through a rigorous research methodology and a comprehensive analysis of the data collected, this study aims to offer valuable insights into enhancing the overall quality of care and support provided to adolescents in childcare institutional settings. Eventually, the findings have the potential to inform evidence-based practices, thus leading to more effective interventions and better outcomes for adolescents in similar contexts worldwide.
The challenge and limitation of the study is that it cannot assess the efficacy of AFIB directly due to the absence of a placebo snack or placebo for mindful mandala art and life skill training. The study examines the effectiveness of AFIB compared with standard care practices only. Efficacy trials involving placebo have the potential to yield compelling evidence of enhanced efficacy.
Research implications and limitations
Adolescents residing in CCIs are susceptible to physical and mental health issues. Specifically, anemia, EBPs, and poor resilience are notably prevalent at a comparatively higher rate. School health nurses serve as the primary personnel in identifying learning disabilities, depression, and malnutrition among school children based on the state policy and protocol. However, those residing in CCIs require a dual focus due to inconsistent caretakers and collective care giving by the wardens. The individual attention received by those in family care settings is compromised for those residing in childcare institutions. The present comprehensive approach attempts to address the widespread issue of anemia, often combined with malnutrition, as well as the EBPs that are more common among such adolescents. This approach consists of evidence-based interventions, including Moringa iron-rich snack supplementation, life skill training, and mindful mandala, which have individually proven effective in addressing anemia, emotional, and behavioral problems, and enhancing resilience. These interventions are often tested individually in school settings. However, the bundle approach tackles these issues holistically and simultaneously within this study design. The evidence gathered from the randomized control trial will provide insights into the prevalence of anemia and emotional-behavioral problems in the selected settings included in the study. This study uses POC methods to conduct anemia screening in a larger sample. The recruited sample is then subjected to laboratory testing, specifically a CBC, to detect IDA based on red blood cell indices. The correlation between POC measures and laboratory measures will help identify the effectiveness of employing POC methods for screening purposes within the community. Furthermore, the study attempts to derive a conceptual mapping of emotional behavioral problems, life skills, mindfulness, and resilience from the study findings.
Ethical Considerations
Compliance with ethical guidelines
This study is registered at the Clinical Trial Registry India (Code: CTRI/2023/10/059027). Ethical approval was obtained from the Institutional Review Board and Institutional Ethical Committee under SRM Medical College Hospital and Research Centre (Code: 8372/IEC/ 2022). Written informed consent and required permissions are obtained from all the participants and responsible persons before the study procedures begin.
Funding
This paper is an output of the cross-sectional survey among institutionalized adolescents in Chennai conducted as part of PhD dissertation of Joy Sandhya Joseph by a research scholar at SRM College of Nursing in SRM Institute of Science and Technology (SRMIST).
Authors' contributions
Conceptualization: Joy Sandhya Joseph; Supervision: Kanniammal Chinnathambi; Methodology: Joy Sandhya Joseph and Kanniammal Chinnathambi; Investigation: Joy Sandhya Joseph; Writing: Joy Sandhya Joseph; Review & Editing: Kanniammal Chinnathambi; Data collection: Joy Sandhya Joseph and Kanniammal Chinnathambi; Data analysis: Joy Sandhya Joseph and Kanniammal Chinnathambi.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
We are grateful to Ms, Vania Olivia, UK Nurse Researcher, for giving expertise in the field of study protocol framing.
References
Anitha, S., et al., 2021. Millets can have a major impact on improving iron status, hemoglobin level, and in reducing iron deficiency anemia-a systematic review and meta-analysis. Frontiers in Nutrition, 8, pp. 725529. [DOI:10.3389/fnut.2021.725529] [PMID]
Arya, S. S., Salve, A. R. & Chauhan, S., 2016. Peanuts as functional food: A review. Journal of Food Science and Technology, 53(1), pp. 31-41. [DOI:10.1007/s13197-015-2007-9]
Chen, M. H., et al., 2013. Association between psychiatric disorders and iron deficiency anemia among children and adolescents: A nationwide population-based study. BMC Psychiatry, 13, pp. 161. [DOI:10.1186/1471-244X-13-161] [PMID]
Connor, K. M. & Davidson, J. R., 2003. Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depression and Anxiety, 18(2), pp. 76–82. [DOI:10.1002/da.10113] [PMID]
Dahlberg, A., et al., 2020. Strengths and Difficulties Questionnaire (SDQ) as an assessment tool for measuring emotional and behavioral problems in young children. European Journal of Public Health, 30( Issue Supplement_5). [DOI:10.1093/eurpub/ckaa165.418]
DeLacey, E., et al., 2020. The nutritional status of children living within institutionalized care: A systematic review. PeerJ, 8, pp. e8484. [DOI:10.7717/peerj.8484] [PMID]
Edlina, K., et al., 2020. Prevalence of emotional, behavioral problems and ego resilience among tea tribe adolescents living in Dibrugarh district of Assam. Clinical Epidemiology and Global Health, 8(1), pp. 190-3. [DOI:10.1016/j.cegh.2019.06.012]
Goodman, R., 1997. The Strengths and Difficulties Questionnaire: A research note. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 38(5), pp. 581–6. [DOI:10.1111/j.1469-7610.1997.tb01545.x] [PMID]
Gosdin, L., et al., 2020. Barriers to and facilitators of iron and folic acid supplementation within a school-based integrated nutrition and health promotion program among Ghanaian Adolescent Girls. Current Developments in Nutrition, 4(9), pp. nzaa135. [DOI:10.1093/cdn/nzaa135] [PMID]
Hosseinian, S. & Nooripour, R., 2019. Effectiveness of mindfulness-based intervention on risky behaviors, resilience, and distress tolerance in adolescents. International Journal of High Risk Behaviors and Addiction, 8(4), pp. e93481. [DOI:10.5812/ijhrba.93481]
Huang, C. C., et al., 2020. Mindfulness, life skills, resilience, and emotional and behavioral problems for gifted low-income adolescents in China. Frontiers in Psychology, 11, pp. 594. [DOI:10.3389/fpsyg.2020.00594] [PMID]
Jilek, E., et al., 2022. Predictors of behavioral and emotional outcomes in toddlers with congenital heart disease. Cardiology in the Young, 32(8), pp. 1216-21. [DOI:10.1017/S1047951121003942] [PMID]
Kim, J. & Wessling-Resnick, M., 2014. Iron and mechanisms of emotional behavior. The Journal of Nutritional Biochemistry, 25(11), pp. 1101–7. [DOI:10.1016/j.jnutbio.2014.07.003] [PMID]
Loa, M., et al., 2021. Moringa oleifera leaf flour biscuits increase the index of erythrocytes in pregnant women with anemia. Gaceta Sanitaria, 35 (Suppl 2), pp. S206–10. [DOI:10.1016/j.gaceta.2021.10.022] [PMID]
Mantadakis, E., 2020. Iron Deficiency anemia in children residing in high and low-income countries: Risk factors, prevention, diagnosis and therapy. Mediterranean Journal of Hematology and Infectious Diseases, 12(1), pp. e2020041. [DOI:10.4084/mjhid.2020.041] [PMID]
Mesías, M., Seiquer, I. & Navarro, M. P., 2013. Iron nutrition in adolescence. Critical Reviews in Food Science and Nutrition, 53(11), pp. 1226-37. [DOI:10.1080/10408398.2011.564333] [PMID]
Mieloo, C., et al., 2012. Validity and reliability of the strengths and difficulties questionnaire in 5-6 year olds: Differences by gender or by parental education? Plos One, 7(5), e36805. [DOI:10.1371/journal.pone.0036805] [PMID]
Mohan Srivastava, N., 2016. Adolescent health in India: Need for more interventional research. Clinical Epidemiology and Global Health, 4(3), pp. 101-2. [DOI:10.1016/S2213-3984(16)30048-3]
National Institute of Nutrition., 2020. Recommended Dietary Allowances (RDA) & Estimated Average Requirements (EAR) for Indians-2020. Hyderabad:National Institute of Nutrition. [Link]
Nath Agarwal, K. & Agarwal, D. K., 2020. Adolescence in Indian Children. Annals of Pediatric Research, 4(3), pp. 1040. [Link]
Patil, P., Singh, S. P. & Patel, P., 2023. Functional properties and health benefits of finger millet (Eleusine coracana L.): A review. The Journal of Phytopharmacology, 12(3), pp. 196-202. [DOI:10.31254/phyto.2023.12308]
Salam, R. A., et al., 2016. Adolescent health interventions: Conclusions, evidence gaps, and research priorities. The Journal of Adolescent Health, 59(4 Suppl), pp. S88-92. [DOI:10.1016/j.jadohealth.2016.05.006] [PMID]
Shafiee, S., Mesgarani, M. & Begum, K., 2015. Assessment of nutritional status among adolescent boys in an urban population of South India. Global Journal of Health Science, 7(3), PP. 335–44. [DOI:10.5539/gjhs.v7n3p335] [PMID]
Sidheek, K. P. F., et al., 2017. Using the Kannada version of the Connor Davidson Resilience Scale to assess resilience and its relationship with psychological distress among adolescent girls in Bangalore, India. Asian Journal of Psychiatry, 30, pp. 169-72. [DOI:10.1016/j.ajp.2017.10.015] [PMID]
Singh, P. & Raghuvanshi, R., 2012. Finger millet for food and nutritional security. African Journal of Food Science, 6(4), pp. 77-84. [Link]
Singh, K. & Choubisa, R., 2009. Effectiveness of self-focused intervention for enhancing students’ well-being. Journal of Indian Academy of Applied Psychology, 35( Special Issue), pp. 23-32. [Link]
Srivastava, S., et al., 2022. Effect of change in individual and household level characteristics on anemia prevalence among adolescent boys and girls in India. BMC Public Health, 22(1), pp. 1478. [DOI:10.1186/s12889-022-13863-w] [PMID]
Tarasova, I. & Chernov, V., 2012. 769 excessive menstrual bleeding is a risk factor of anemia in adolescent schoolgirls. Archives of Disease in Childhood, 97(Suppl 2). [DOI:10.1136/archdischild-2012-302724.0769]
Type of Study: Research |
Subject:
General
Received: 2024/03/1 | Accepted: 2024/05/27 | Published: 2024/11/1
Received: 2024/03/1 | Accepted: 2024/05/27 | Published: 2024/11/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
