Sat, Aug 8, 2026
[Archive]
Volume 12, Issue 1 (Winter 2026)
JCCNC 2026, 12(1): 19-32 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Asonye C, Ojewole F. Sociodemographic and Clinical Correlates of Health-related Quality of Life in Patients With Type 2 Diabetes Mellitus Living in Nigeria. JCCNC 2026; 12 (1) :19-32
URL: http://jccnc.iums.ac.ir/article-1-663-en.html
URL: http://jccnc.iums.ac.ir/article-1-663-en.html



1- Department of Adult Health (Med-Surg) Nursing, Babcock University School of Nursing, Ilishan Remo, Nigeria. , christianasonye1@gmail.com
2- Department of Adult Health (Med-Surg) Nursing, Babcock University School of Nursing, Ilishan Remo, Nigeria.
2- Department of Adult Health (Med-Surg) Nursing, Babcock University School of Nursing, Ilishan Remo, Nigeria.
Keywords: Diabetes mellitus, Health-related quality of life (HRQOL), World Health Organization quality of life short form (WHOQOL-BREF), Correlates of health-related quality of life, Nigeria
Full-Text [PDF 702 kb]
(335 Downloads)
| Abstract (HTML) (682 Views)
Full-Text: (66 Views)
Introduction
Diabetes is a long-term physical condition that develops when the body either fails to produce sufficient insulin or cannot use the insulin it produces effectively. This disorder, referred to as diabetes mellitus (DM), has emerged as a pressing global health challenge and is classified among the 4 leading noncommunicable diseases demanding urgent intervention. Over the past few decades, the number of people affected has risen sharply (WHO, 2016).
According to the 2021 International Diabetes Federation (IDF), about 537 million adults worldwide—equivalent to 10.5% of those aged 20 to 79 years—are living with diabetes, and nearly half remain undiagnosed. Projections indicate that this number will rise to 643 million by 2030 and further to 783 million by 2045 (Sun et al., 2021). Type 2 DM (T2DM) represents more than 90% of all cases globally (Magliano & Boyko, 2021). Strikingly, about three-quarters of adults with diabetes reside in low- and middle-income nations, including Nigeria (IDF, 2022). Diabetes is also a major contributor to mortality, responsible for roughly 12.2% of deaths among adults aged 20 to 79 years (Sun et al., 2021).
In Nigeria, the first national survey on diabetes, conducted in 1992, reported a prevalence of 2.2%. More recent figures from the IDF estimate a prevalence of 3.7% among adults aged 20 to 69 years, translating to over 3.6 million people (Asonye & Ojewole, 2023). However, these estimates may not fully capture the burden of the disease, as they often rely on extrapolated data. Local and regional studies within Nigeria have reported prevalence rates ranging from 2% to 12% (Gezawa et al., 2015; Uloko et al., 2018). In Ogun State specifically, the prevalence is estimated at around 5% (World Diabetes Foundation, 2018).
DM is regarded as one of the most pressing health emergencies of the 21st century, not only because of its rapid global rise and the high proportion of undiagnosed cases, but also because of the serious complications it causes and the heavy social and economic burden it imposes. When poorly managed, it can lead to serious complications such as blindness, kidney failure, and limb amputation, all of which severely affect quality of life (QoL) (Saeedi et al., 2020). Importantly, the relationship between diabetes and QoL is bidirectional: Not only does the disease impact a person’s QoL, but their QoL also influences how well they manage their condition. Poor QoL can lead to reduced self-care and poor blood sugar control, increasing the risk of complications (Garratt et al., 2002). Conversely, when patients experience satisfaction and wellbeing, including managing their diabetes, they tend to be more motivated to maintain effective self-care routines. This condition fosters better daily wellbeing and long-term health outcomes, creating a positive feedback loop that further enhances their QoL (Fadli, 2022; Malini, 2022; Roglic, 2016).
The World Health Organization (WHO) defines QOL as an individual’s perception of their position in life within the context of their culture and value systems, relative to their goals, expectations, and concerns. It encompasses various dimensions, including physical health, psychological state, personal beliefs, social relationships, and environmental factors (WHO Group, 1994). Measures of health-related QoL (HRQOL) provide a scientific way to assess how health affects overall QoL, moving well beyond traditional approaches focused solely on clinical or laboratory findings (Taylor, 2000).
In people with T2DM, several sociodemographic and disease-related factors influence HRQOL. Research has shown that variables such as age, gender, marital status, education, occupation, and income are linked to differences in HRQOL (Al Hayek et al., 2014; Altınok et al., 2016). Despite the importance of evaluating HRQOL to inform healthcare decisions and improve clinical guidelines, studies exploring the determinants of QoL in T2DM patients remain limited. This study, therefore, aims to determine the sociodemographic and clinical correlates of HRQOL among T2DM patients attending diabetes clinics at teaching hospitals in Ogun State, Nigeria.
Null hypothesis (H₀): There is no significant association between sociodemographic and clinical factors and the HRQOL among patients with T2DM.
Materials and Methods
Design, setting, and sample
An institution-based cross-sectional study was conducted at the Olabisi Onabanjo University Teaching Hospital (OOUTH), Sagamu, and the Babcock University Teaching Hospital (BUTH), Ilisan Remo, Ogun State. BUTH has over 250 beds and a well-established, well-equipped department, including the Endocrinology, Diabetes, and Metabolism (E.D.M.) Department, which cares for patients with DM from towns and cities across the Southwest region of Nigeria on referral. OOUTH, established in 1986, is located in Sagamu, a town 50 miles north of Lagos, South West, Nigeria. The OOUTH is a tertiary hospital with 250 beds. It serves as a major referral center for healthcare facilities across all the Remo Local Government Areas of Ogun State. The OOUTH has many well-established, well-equipped departments, including the Endocrinology/Diabetes department.
The population for this research study was all patients diagnosed with DM attending diabetes clinics in BUTH and OOUTH. The target population was 260 patients diagnosed with T2DM who met the inclusion criteria.
Inclusion criteria were patients aged 21 years or older, diagnosed with T2DM for at least 3 months, and who consented to participate in the study.
Exclusion criteria were chronically ill patients admitted into the hospitals, those with other types of diabetes, and patients with hyperglycemia resulting from gestational diabetes mellitus, Cushing syndrome, and paraneoplastic syndrome.
A sample size of 219 (10% attrition included) was determined using the Leslie Kish (1965) formula for a single proportion, with an absolute error of 5% allowed and a prevalence of 15.3% from a study conducted in Lagos (Kayode et al., 2015). The sample size formula for a single proportion is stated below (Equation 1):
A stratified, proportionate-to-size sampling method was used to allocate the total sample size of 219 across the two hospitals: BUTH (60 patients) and OOUTH (200 patients). Based on proportional allocation, approximately 51 participants were selected from BUTH and 168 from OOUTH. Within each hospital, total enumeration was employed, meaning all eligible and consenting patients were recruited until the required number for each stratum was achieved.
Instruments for data collection
A 36-item self-administered questionnaire was used to retrieve information from the patients. The questionnaire was divided into two sections. The researcher designed section A, while section B was adopted from a validated scale.
Section A investigated sociodemographic and clinical factors. It contains 10 items, including age, gender, religion, level of education, monthly income, ethnicity, marital status, duration of diabetes, smoking status, and alcohol consumption status.
Section B was the WHO quality of life–short form (WHOQOL-BREF). This validated, internationally recognized tool is designed to assess individuals’ perceptions of their QoL within the context of their culture, value systems, personal goals, standards, and concerns. It is particularly useful in chronic disease populations, including those with diabetes. The WHOQOL-BREF consists of 26 items divided into 4 domains: physical health (7 items), psychological health (6 items), social relationships (3 items), and environment (8 items). Each domain captures specific dimensions of an individual’s QoL. The physical health domain includes aspects such as pain and discomfort, energy and fatigue, sleep and rest, and work capacity. The psychological domain covers positive and negative feelings, self-esteem, body image, and personal beliefs. The social relationships domain evaluates personal relationships, social support, and sexual activity. The environment domain includes financial resources, safety, home environment, access to health and social care, and the physical living environment.
In addition to the 4 domains, the instrument also contains two general questions: one assessing the individual’s overall perception of QoL, and the other evaluating their overall perception of their health. These two items are analyzed independently and are not included in the domain scores.
Each item is rated on a 5-point Likert scale, with responses ranging from 1 (very poor/dissatisfied) to 5 (very good/satisfied). Domain scores are calculated by first computing the mean of all items within a domain and then multiplying the mean score by 4 to make it comparable to the WHOQOL-100. These raw domain scores are subsequently transformed to a 0–100 scale, with higher scores indicating better QoL. The interpretation of domain scores follows this guideline: Scores of 0–45 indicate poor QoL, 46–65 moderate QoL, and 66–100 high QoL. The overall HRQoL score for each participant is derived as the average of the 4 domain scores. The Cronbach α values for the 4 domain scores ranged from 0.66 to 0.84, indicating good internal consistency (Harper et al., 1998).
Method of data collection
Research assistants (RAs) were recruited and trained to help in the distribution and collection of the questionnaire. The complete details of the study’s aims and implications were explained to the participants. The questionnaires were distributed to eligible respondents who were willing to participate in the study. The researcher and the RAs retrieved all the questionnaires from the respondents. The study lasted for about 12 weeks.
Data analysis
The data were first sorted and cleaned, and analysis was done using SPSS software, version 23. Descriptive statistics, including frequencies, percentages, Mean±SD, were used to summarize the participants’ sociodemographic characteristics and HRQOL domain scores. Skewness and standard error were computed to assess the normality of the score distributions. The related factors were determined using the linear regression model. Before analysis, key assumptions were evaluated. Linearity and homoscedasticity were assessed using scatter plots; normality of residuals was verified using histograms and Q-Q plots. Multicollinearity was assessed using the variance inflation factor (VIF), with all VIF values below 10. The Durbin-Watson statistic was used to confirm residual independence, with values between 1.5 and 2.5 indicating acceptable independence. A P<0.05 in the multiple linear regression analysis was considered an independent factor associated with HRQOL.
Results
A total of 219 participants were recruited for this study, and 209 participated, yielding a 95% response rate.
Table 1 shows that most of the respondents were Yoruba (91.9%), aged 61 years and above (42%), and female (71.3%). Most of them (63.2%) were Christians, 39.7% had tertiary education, and about 92.3% were married. Most participants (54.5%) had a monthly income above the minimum wage (30000 Naira [₦] and above). In addition, 92.3% of the respondents did not smoke or consume alcohol, and 57.4% were living with T2DM for less than 10 years.

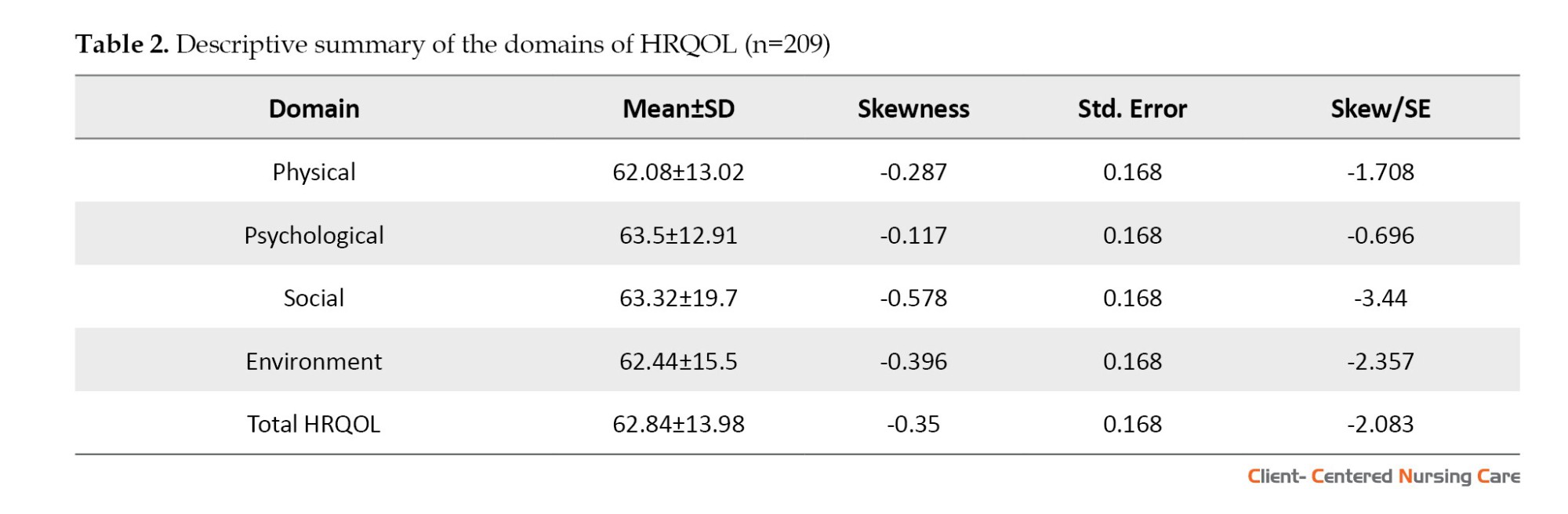
The total mean HRQOL score was 62.84±13.98. All of the individual domain mean scores were above the middle (i.e. 50) of the possible score range (0–100 for WHOQOL-BREF at a scale of 100) (Table 2). The skewness and standard error values for all 4 domains were <1.96; hence, the data distributions are normal.
Study participants were asked to provide their perception of their HRQOL and health satisfaction. Based on their perception, about 179 patients (85.6%) reported that their HRQOL was good and very good. Regarding their perceived health, 122 patients (58.4%) were satisfied or very satisfied (Table 3).

Multivariate linear regression was used to examine the association between respondents’ sociodemographic characteristics and their HRQOL (Table 4). Patients’ age was positively associated with all HRQOL domains. Older age was significantly associated with better physical health (P<0.001), psychological health (P=0.026), social relationships (P=0.022), and environmental health (P=0.024).

Gender was positively associated with HRQOL across all four domains. Being female was associated with higher scores in physical health (P=0.014), psychological health (P=0.012), social relationships (P=0.037), and environmental health (P=0.022).
Religion was significantly associated only with the social domain of HRQOL. Being Muslim was associated with higher social relationship scores (P=0.016), while no significant associations were found with physical, psychological, or environmental domains. Educational status, particularly having a tertiary education, was positively associated with all HRQOL domains. Significant associations were observed for physical health (P=0.019), psychological health (P=0.028), social relationships (P=0.026), and environmental health (P=0.011). Marital status was positively associated with HRQOL in all domains. Being married was associated with higher scores in physical health (P<0.001), psychological health (P=0.025), social relationships (P=0.002), and environmental health (P=0.018). Monthly income was positively associated with all four HRQOL domains. Earning above ₦30000 was significantly associated with better physical health (P=0.035), psychological health (P=0.035), social relationships (P=0.026), and environmental health (P=0.020).
Smoking status was negatively associated with HRQOL in all domains. Smoking was associated with lower scores in physical health (P=0.014), psychological health (P=0.041), social relationships (P=0.020), and environmental health (P=0.009). Alcohol consumption was negatively associated with all domains of HRQOL. Alcohol use was associated with lower physical health (P=0.006), psychological health (P=0.034), social relationships (P=0.017), and environmental health (P=0.010). Duration of diabetes also demonstrated a negative association with HRQOL. Participants who had lived with T2DM for over 10 years reported lower scores in physical health (P=0.007), psychological health (P=0.009), social relationships (P=0.014), and environmental health (P=0.021).
Discussion
The findings showed a mean age of 56.1±9.7 years, with the majority of participants being females (71.3%) and married (92.3%). The prevalence of T2DM is increasing in both men and women. Men have usually been diagnosed at a younger age and have lower body fat than women at the time of diagnosis. Worldwide, about 17.7 million more men than women have DM (Kautzky-Willer et al., 2023). Despite this, women often present with a higher burden of risk factors—particularly obesity—when diagnosed with T2DM.
Additionally, psychosocial stress may contribute more significantly to diabetes risk in women than in men. Women experience more pronounced hormonal fluctuations and bodily changes related to reproductive events throughout their lives. For instance, pregnancy can unmask latent metabolic dysfunction, resulting in gestational diabetes, a condition regarded as one of the most significant risk factors for the future development of T2DM in women (Ciarambino et al., 2022; Kautzky-Willer et al., 2023).
The present study revealed that the participants had an average mean score of 62.84±13.98 as regards their HRQOL, and this is similar to previous studies that used the same tool (WHOQOL-BREF) by Gebremedhin et al. (2019), who revealed a mean score of 51.50±15.78 for overall HRQOL, and Ababio et al. (2017), who revealed scores of the overall QOL in both Ghana (56.19±8.23) and Nigeria (64.34±7.34). Another study conducted in Nigeria by Nwatu et al. (2019) reported a mean overall QoL score of 75.6±19.4. Further analysis of the present study revealed that all domain scores of the WHOQOL-BREF scale were above the midpoint (i.e. 50) of the possible score range (0–100 for WHOQOL-BREF at a scale of 100). A similar finding was reported in Nepal by Mishra et al. (2015), who also used the WHOQOL-BREF scale among patients with T2DM. In contrast, Amin et al. (2022) reported below-average domain scores among diabetic patients in Bangladesh using the same scale.
Research conducted in West Java (Puspasari & Farera, 2021) and Iran (Abbasi-Ghahramanloo et al., 2020) found that many people living with T2DM experience poor QoL, particularly in the physical, psychological, and environmental domains. The comparatively higher QoL scores reported in this study may be linked to participants’ characteristics, many of whom had a tertiary education and received subsidized treatment at one of the hospitals involved. Education and financial support—especially assistance with the cost of medicines—can make a critical difference by enabling patients to engage more consistently with treatment. This finding is highly relevant in Nigeria, where patients usually pay for healthcare directly out of pocket. Education itself is widely recognized as a key determinant of health. For example, the Incheon declaration (UNESCO, 2015) emphasizes that education fosters informed decision-making and healthier lifestyles, while research from high-income settings has shown that adults with lower levels of education consistently report poorer health outcomes (Zajacova & Lawrence, 2018).
In this study, several variables, including age, gender, religion, education, marital status, income, smoking, alcohol intake, and the length of time since diagnosis, significantly correlate with HRQOL. These findings are consistent with previous evidence that has linked HRQOL to sociodemographic and clinical factors such as age (Obosi & Fatunbi, 2018; Lu et al., 2017; Gebremedhin et al., 2019), gender (Manjunath et al., 2014; Obosi & Fatunbi, 2018), religion (Obosi & Fatunbi, 2018), education (Obosi & Fatunbi, 2018), marital status (Obosi & Fatunbi, 2018; Pandey et al., 2020), income (Esin et al., 2016), alcohol use (Daeppen et al., 2014; Ortolá et al., 2016), and duration of T2DM (Obosi & Fatunbi, 2018; de Lima et al., 2018). Also, Trikkalinou et al. (2017) emphasized that the QOL of individuals with diabetes is shaped by a combination of social and clinical factors, which may differ across study designs, populations, and methodologies. Altogether, the results highlight the importance of detailed history-taking during patient assessment. For nurses, this means considering not only clinical symptoms but also social context to deliver individualized care and set appropriate priorities for interventions.
In the present study, participants’ age emerged as a notable predictor of HRQOL. This finding is supported by previous research from Egypt (Ibrahim, 2016), which suggests that psychological well-being can improve with advancing age. However, studies in Serbia (Spasić et al., 2014) and Ethiopia (Gebremedhin et al., 2019) show the opposite trend, with younger patients reporting better QoL. This inconsistency likely reflects the complex interplay among aging, perceptions of health, and comorbidities. While aging often brings physiological decline and greater susceptibility to complications such as cardiovascular or renal disease (Al-Aboudi et al., 2015; Gebremariam et al., 2022), the relatively older participants in this study—most of whom had secondary or tertiary education—may have benefited from health literacy and prior experience managing their illness. This finding may explain why age was positively linked with QoL here, a finding also supported by Nwatu et al. (2019), who reported lower QoL scores among younger patients.
Gender differences were also evident, with female participants reporting higher HRQOL across all domains. This observation is consistent with findings from Oman (D’Souza et al., 2016) and Nigeria (Nwatu et al., 2019). However, studies from Botswana (Rwegerera et al., 2017) and Ethiopia (Wonde et al., 2022) reported the reverse. Cultural norms may help explain these differences, as women in many African settings are more likely than men to seek medical help, partly due to their repeated interactions with health services during pregnancy and childbirth. Men, on the other hand, may delay seeking care because of cultural expectations that equate masculinity with strength and independence. Religion was significantly associated only with the social domain of HRQOL. Muslim participants in this study reported higher scores on social relationships, a finding consistent with research from Saudi Arabia (Ali et al., 2013) and systematic reviews suggesting that religious participation can positively influence self-care and glycemic control (Weber & Doolittle, 2023). Faith-based practices may enhance social support networks and foster a sense of community belonging, which, in turn, can improve QoL outcomes.
Furthermore, educational status, particularly having a tertiary education, was positively associated with all HRQOL domains, and this is supported by previous studies in India, Ethiopia, and Turkey, showing that education enhances both psychological and social wellbeing while contributing to better disease management (Sreedevi et al., 2016; Reba et al., 2018; Esen & Aktürk, 2020; Aschalew et al., 2020). Educated patients understand key information about DM and appropriately comply with self-management advice. This knowledge may help prevent deterioration in glycemic control, prompt early medical advice, detect and manage psychiatric symptomatology, and improve HRQOL. Thus, higher educational status can significantly improve patients’ HRQOL (Pandey et al., 2020). Since education is also closely tied to income, higher educational attainment may provide patients with the financial means to access and sustain appropriate treatment, thereby further enhancing their QoL.
Marital status was positively associated with HRQOL across all domains, consistent with previous studies that posit that social and emotional support from a partner can buffer the psychological and economic burdens of living with a chronic condition (Papazafiropoulou et al., 2015; Aschalew et al., 2020). Likewise, participants with higher monthly income (above ₦30000) reported better HRQOL across all 4 HRQOL domains, a finding supported by previous studies (Esin et al., 2016; Amin et al., 2022), reflecting the role of financial stability in enabling access to care in resource-constrained settings like Nigeria.
Lifestyle factors such as smoking and alcohol consumption were strongly linked to poorer HRQOL. Smoking has a consistent and statistically significant negative effect on all measured aspects of QoL in this study population. The negative beta values mean smokers report poorer physical, mental, social, and environmental health compared to non-smokers. These findings align with previous studies linking cigarette smoking to self-reported reductions in overall health, including deteriorated mental and physical wellbeing and increased limitations in daily activities (Mody & Smith, 2006; Habib et al., 2024). Panahi et al. (2024), using the SF-12 questionnaire, found that current smokers had significantly poorer mental health scores. Likewise, earlier studies have shown that smoking and alcohol use can lead to feelings of social stigma among patients, which may further diminish QoL. These social factors likely contribute to the overall reduction in wellbeing observed among affected individuals (Aschalew et al., 2020; Feyisa et al., 2020).
The present study revealed that alcohol consumption is negatively associated with all domains of the HRQOL scale. The result connotes that the more a patient consumes alcohol, the poorer the HRQOL. This finding aligns with earlier research showing that people who drink moderately to heavily tend to have poorer HRQOL (mental health) compared to those who do not drink or only drink occasionally (Daeppen et al., 2014; Ortolá et al., 2016). The researcher opined that the sociocultural pattern of alcohol use among the study participants may have affected their HRQOL. Alcohol consumption can potentially impair cognition and alter an individual’s consciousness. It impairs glycemic control, which may result in worrying about glucose levels, depression, complications, and reduced satisfaction with an individual’s HRQOL (Aschalew et al., 2020).
Finally, disease duration negatively impacted HRQOL, with patients living with T2DM for more than a decade reporting poorer outcomes across domains. This finding aligns with research from Ethiopia (Gebremedhin et al., 2019), Serbia (Spasić et al., 2014), and Malaysia (Chew et al., 2015), which found that longer disease duration was associated with increased complications and treatment fatigue. In contrast, a study from Nepal (Mishra et al., 2015) suggested longer disease duration might allow patients to adapt, though such findings may reflect contextual differences. Nonetheless, the progressive complications associated with diabetes often weigh heavily on patients’ physical and psychological health over time.
Limitations of this study may affect the generalizability of the findings. These limitations include the study’s cross-sectional design, which limits the ability to establish causal relationships, and reliance on self-report data, which increases the risk of bias. The relatively small sample size and limited geographic scope may also limit the generalizability of the findings to a broader population of patients with T2DM.
Conclusion
The present study’s results revealed moderately high HRQOL among patients with T2DM, with mean scores above the midpoint across all domains—physical health, psychological health, social relationships, and environmental health—indicating generally positive perceptions of wellbeing and satisfaction with their HRQOL and health status. Significant positive sociodemographic correlates of HRQOL were age, gender (female), religion (Islam), educational status (tertiary), marital status (married), and monthly income (>₦30000). Conversely, smoking, alcohol consumption, and longer duration of living with T2DM were consistently associated with poorer HRQOL across all domains. Overall, these results emphasize the multifaceted nature of QoL among people with T2DM and underscore the importance of addressing sociodemographic and clinical factors in comprehensive diabetes care. Interventions tailored to improve lifestyle behaviors and support vulnerable groups need to be studied to enhance overall HRQOL in this population.
Ethical Considerations
Compliance with ethical guidelines
Ethical approval was obtained from the Babcock University Health Research Ethics Committee (BUHREC) (Code: BUHREC667/22), and from the Olabisi Onabanjo University Teaching Hospital (OOUTH)Health Research Ethics Committee (Code: OOUTH/HREC/557/2022AP). Participation in the study was voluntary, and participants had the right to withdraw at any time without feeling pressured to continue, with no negative consequences. Participants gave their informed consent before the study began. The principle of confidentiality and anonymity of all participants was respected. Only researchers approved by BUHREC and OOUTH-HREC were allowed to access the study data. The researcher also ensured that all institutional data privacy protocols were strictly followed.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Data collection, analysis, and interpretation: Christian Asonye; Review and editing: Foluso Ojewole; Conceptualization, study design, writing the original draft and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank the participants, RAs, and the staff of Babcock University Teaching Hospital (BUTH), Ilisan Remo, Ogun State, Nigeria, and Olabisi Onabanjo University Teaching Hospital (OOUTH), Sagamu, Nigeria, for their cooperation and assistance throughout this study.
References
Diabetes is a long-term physical condition that develops when the body either fails to produce sufficient insulin or cannot use the insulin it produces effectively. This disorder, referred to as diabetes mellitus (DM), has emerged as a pressing global health challenge and is classified among the 4 leading noncommunicable diseases demanding urgent intervention. Over the past few decades, the number of people affected has risen sharply (WHO, 2016).
According to the 2021 International Diabetes Federation (IDF), about 537 million adults worldwide—equivalent to 10.5% of those aged 20 to 79 years—are living with diabetes, and nearly half remain undiagnosed. Projections indicate that this number will rise to 643 million by 2030 and further to 783 million by 2045 (Sun et al., 2021). Type 2 DM (T2DM) represents more than 90% of all cases globally (Magliano & Boyko, 2021). Strikingly, about three-quarters of adults with diabetes reside in low- and middle-income nations, including Nigeria (IDF, 2022). Diabetes is also a major contributor to mortality, responsible for roughly 12.2% of deaths among adults aged 20 to 79 years (Sun et al., 2021).
In Nigeria, the first national survey on diabetes, conducted in 1992, reported a prevalence of 2.2%. More recent figures from the IDF estimate a prevalence of 3.7% among adults aged 20 to 69 years, translating to over 3.6 million people (Asonye & Ojewole, 2023). However, these estimates may not fully capture the burden of the disease, as they often rely on extrapolated data. Local and regional studies within Nigeria have reported prevalence rates ranging from 2% to 12% (Gezawa et al., 2015; Uloko et al., 2018). In Ogun State specifically, the prevalence is estimated at around 5% (World Diabetes Foundation, 2018).
DM is regarded as one of the most pressing health emergencies of the 21st century, not only because of its rapid global rise and the high proportion of undiagnosed cases, but also because of the serious complications it causes and the heavy social and economic burden it imposes. When poorly managed, it can lead to serious complications such as blindness, kidney failure, and limb amputation, all of which severely affect quality of life (QoL) (Saeedi et al., 2020). Importantly, the relationship between diabetes and QoL is bidirectional: Not only does the disease impact a person’s QoL, but their QoL also influences how well they manage their condition. Poor QoL can lead to reduced self-care and poor blood sugar control, increasing the risk of complications (Garratt et al., 2002). Conversely, when patients experience satisfaction and wellbeing, including managing their diabetes, they tend to be more motivated to maintain effective self-care routines. This condition fosters better daily wellbeing and long-term health outcomes, creating a positive feedback loop that further enhances their QoL (Fadli, 2022; Malini, 2022; Roglic, 2016).
The World Health Organization (WHO) defines QOL as an individual’s perception of their position in life within the context of their culture and value systems, relative to their goals, expectations, and concerns. It encompasses various dimensions, including physical health, psychological state, personal beliefs, social relationships, and environmental factors (WHO Group, 1994). Measures of health-related QoL (HRQOL) provide a scientific way to assess how health affects overall QoL, moving well beyond traditional approaches focused solely on clinical or laboratory findings (Taylor, 2000).
In people with T2DM, several sociodemographic and disease-related factors influence HRQOL. Research has shown that variables such as age, gender, marital status, education, occupation, and income are linked to differences in HRQOL (Al Hayek et al., 2014; Altınok et al., 2016). Despite the importance of evaluating HRQOL to inform healthcare decisions and improve clinical guidelines, studies exploring the determinants of QoL in T2DM patients remain limited. This study, therefore, aims to determine the sociodemographic and clinical correlates of HRQOL among T2DM patients attending diabetes clinics at teaching hospitals in Ogun State, Nigeria.
Null hypothesis (H₀): There is no significant association between sociodemographic and clinical factors and the HRQOL among patients with T2DM.
Materials and Methods
Design, setting, and sample
An institution-based cross-sectional study was conducted at the Olabisi Onabanjo University Teaching Hospital (OOUTH), Sagamu, and the Babcock University Teaching Hospital (BUTH), Ilisan Remo, Ogun State. BUTH has over 250 beds and a well-established, well-equipped department, including the Endocrinology, Diabetes, and Metabolism (E.D.M.) Department, which cares for patients with DM from towns and cities across the Southwest region of Nigeria on referral. OOUTH, established in 1986, is located in Sagamu, a town 50 miles north of Lagos, South West, Nigeria. The OOUTH is a tertiary hospital with 250 beds. It serves as a major referral center for healthcare facilities across all the Remo Local Government Areas of Ogun State. The OOUTH has many well-established, well-equipped departments, including the Endocrinology/Diabetes department.
The population for this research study was all patients diagnosed with DM attending diabetes clinics in BUTH and OOUTH. The target population was 260 patients diagnosed with T2DM who met the inclusion criteria.
Inclusion criteria were patients aged 21 years or older, diagnosed with T2DM for at least 3 months, and who consented to participate in the study.
Exclusion criteria were chronically ill patients admitted into the hospitals, those with other types of diabetes, and patients with hyperglycemia resulting from gestational diabetes mellitus, Cushing syndrome, and paraneoplastic syndrome.
A sample size of 219 (10% attrition included) was determined using the Leslie Kish (1965) formula for a single proportion, with an absolute error of 5% allowed and a prevalence of 15.3% from a study conducted in Lagos (Kayode et al., 2015). The sample size formula for a single proportion is stated below (Equation 1):
A stratified, proportionate-to-size sampling method was used to allocate the total sample size of 219 across the two hospitals: BUTH (60 patients) and OOUTH (200 patients). Based on proportional allocation, approximately 51 participants were selected from BUTH and 168 from OOUTH. Within each hospital, total enumeration was employed, meaning all eligible and consenting patients were recruited until the required number for each stratum was achieved.
Instruments for data collection
A 36-item self-administered questionnaire was used to retrieve information from the patients. The questionnaire was divided into two sections. The researcher designed section A, while section B was adopted from a validated scale.
Section A investigated sociodemographic and clinical factors. It contains 10 items, including age, gender, religion, level of education, monthly income, ethnicity, marital status, duration of diabetes, smoking status, and alcohol consumption status.
Section B was the WHO quality of life–short form (WHOQOL-BREF). This validated, internationally recognized tool is designed to assess individuals’ perceptions of their QoL within the context of their culture, value systems, personal goals, standards, and concerns. It is particularly useful in chronic disease populations, including those with diabetes. The WHOQOL-BREF consists of 26 items divided into 4 domains: physical health (7 items), psychological health (6 items), social relationships (3 items), and environment (8 items). Each domain captures specific dimensions of an individual’s QoL. The physical health domain includes aspects such as pain and discomfort, energy and fatigue, sleep and rest, and work capacity. The psychological domain covers positive and negative feelings, self-esteem, body image, and personal beliefs. The social relationships domain evaluates personal relationships, social support, and sexual activity. The environment domain includes financial resources, safety, home environment, access to health and social care, and the physical living environment.
In addition to the 4 domains, the instrument also contains two general questions: one assessing the individual’s overall perception of QoL, and the other evaluating their overall perception of their health. These two items are analyzed independently and are not included in the domain scores.
Each item is rated on a 5-point Likert scale, with responses ranging from 1 (very poor/dissatisfied) to 5 (very good/satisfied). Domain scores are calculated by first computing the mean of all items within a domain and then multiplying the mean score by 4 to make it comparable to the WHOQOL-100. These raw domain scores are subsequently transformed to a 0–100 scale, with higher scores indicating better QoL. The interpretation of domain scores follows this guideline: Scores of 0–45 indicate poor QoL, 46–65 moderate QoL, and 66–100 high QoL. The overall HRQoL score for each participant is derived as the average of the 4 domain scores. The Cronbach α values for the 4 domain scores ranged from 0.66 to 0.84, indicating good internal consistency (Harper et al., 1998).
Method of data collection
Research assistants (RAs) were recruited and trained to help in the distribution and collection of the questionnaire. The complete details of the study’s aims and implications were explained to the participants. The questionnaires were distributed to eligible respondents who were willing to participate in the study. The researcher and the RAs retrieved all the questionnaires from the respondents. The study lasted for about 12 weeks.
Data analysis
The data were first sorted and cleaned, and analysis was done using SPSS software, version 23. Descriptive statistics, including frequencies, percentages, Mean±SD, were used to summarize the participants’ sociodemographic characteristics and HRQOL domain scores. Skewness and standard error were computed to assess the normality of the score distributions. The related factors were determined using the linear regression model. Before analysis, key assumptions were evaluated. Linearity and homoscedasticity were assessed using scatter plots; normality of residuals was verified using histograms and Q-Q plots. Multicollinearity was assessed using the variance inflation factor (VIF), with all VIF values below 10. The Durbin-Watson statistic was used to confirm residual independence, with values between 1.5 and 2.5 indicating acceptable independence. A P<0.05 in the multiple linear regression analysis was considered an independent factor associated with HRQOL.
Results
A total of 219 participants were recruited for this study, and 209 participated, yielding a 95% response rate.
Table 1 shows that most of the respondents were Yoruba (91.9%), aged 61 years and above (42%), and female (71.3%). Most of them (63.2%) were Christians, 39.7% had tertiary education, and about 92.3% were married. Most participants (54.5%) had a monthly income above the minimum wage (30000 Naira [₦] and above). In addition, 92.3% of the respondents did not smoke or consume alcohol, and 57.4% were living with T2DM for less than 10 years.
The total mean HRQOL score was 62.84±13.98. All of the individual domain mean scores were above the middle (i.e. 50) of the possible score range (0–100 for WHOQOL-BREF at a scale of 100) (Table 2). The skewness and standard error values for all 4 domains were <1.96; hence, the data distributions are normal.
Study participants were asked to provide their perception of their HRQOL and health satisfaction. Based on their perception, about 179 patients (85.6%) reported that their HRQOL was good and very good. Regarding their perceived health, 122 patients (58.4%) were satisfied or very satisfied (Table 3).
Multivariate linear regression was used to examine the association between respondents’ sociodemographic characteristics and their HRQOL (Table 4). Patients’ age was positively associated with all HRQOL domains. Older age was significantly associated with better physical health (P<0.001), psychological health (P=0.026), social relationships (P=0.022), and environmental health (P=0.024).
Gender was positively associated with HRQOL across all four domains. Being female was associated with higher scores in physical health (P=0.014), psychological health (P=0.012), social relationships (P=0.037), and environmental health (P=0.022).
Religion was significantly associated only with the social domain of HRQOL. Being Muslim was associated with higher social relationship scores (P=0.016), while no significant associations were found with physical, psychological, or environmental domains. Educational status, particularly having a tertiary education, was positively associated with all HRQOL domains. Significant associations were observed for physical health (P=0.019), psychological health (P=0.028), social relationships (P=0.026), and environmental health (P=0.011). Marital status was positively associated with HRQOL in all domains. Being married was associated with higher scores in physical health (P<0.001), psychological health (P=0.025), social relationships (P=0.002), and environmental health (P=0.018). Monthly income was positively associated with all four HRQOL domains. Earning above ₦30000 was significantly associated with better physical health (P=0.035), psychological health (P=0.035), social relationships (P=0.026), and environmental health (P=0.020).
Smoking status was negatively associated with HRQOL in all domains. Smoking was associated with lower scores in physical health (P=0.014), psychological health (P=0.041), social relationships (P=0.020), and environmental health (P=0.009). Alcohol consumption was negatively associated with all domains of HRQOL. Alcohol use was associated with lower physical health (P=0.006), psychological health (P=0.034), social relationships (P=0.017), and environmental health (P=0.010). Duration of diabetes also demonstrated a negative association with HRQOL. Participants who had lived with T2DM for over 10 years reported lower scores in physical health (P=0.007), psychological health (P=0.009), social relationships (P=0.014), and environmental health (P=0.021).
Discussion
The findings showed a mean age of 56.1±9.7 years, with the majority of participants being females (71.3%) and married (92.3%). The prevalence of T2DM is increasing in both men and women. Men have usually been diagnosed at a younger age and have lower body fat than women at the time of diagnosis. Worldwide, about 17.7 million more men than women have DM (Kautzky-Willer et al., 2023). Despite this, women often present with a higher burden of risk factors—particularly obesity—when diagnosed with T2DM.
Additionally, psychosocial stress may contribute more significantly to diabetes risk in women than in men. Women experience more pronounced hormonal fluctuations and bodily changes related to reproductive events throughout their lives. For instance, pregnancy can unmask latent metabolic dysfunction, resulting in gestational diabetes, a condition regarded as one of the most significant risk factors for the future development of T2DM in women (Ciarambino et al., 2022; Kautzky-Willer et al., 2023).
The present study revealed that the participants had an average mean score of 62.84±13.98 as regards their HRQOL, and this is similar to previous studies that used the same tool (WHOQOL-BREF) by Gebremedhin et al. (2019), who revealed a mean score of 51.50±15.78 for overall HRQOL, and Ababio et al. (2017), who revealed scores of the overall QOL in both Ghana (56.19±8.23) and Nigeria (64.34±7.34). Another study conducted in Nigeria by Nwatu et al. (2019) reported a mean overall QoL score of 75.6±19.4. Further analysis of the present study revealed that all domain scores of the WHOQOL-BREF scale were above the midpoint (i.e. 50) of the possible score range (0–100 for WHOQOL-BREF at a scale of 100). A similar finding was reported in Nepal by Mishra et al. (2015), who also used the WHOQOL-BREF scale among patients with T2DM. In contrast, Amin et al. (2022) reported below-average domain scores among diabetic patients in Bangladesh using the same scale.
Research conducted in West Java (Puspasari & Farera, 2021) and Iran (Abbasi-Ghahramanloo et al., 2020) found that many people living with T2DM experience poor QoL, particularly in the physical, psychological, and environmental domains. The comparatively higher QoL scores reported in this study may be linked to participants’ characteristics, many of whom had a tertiary education and received subsidized treatment at one of the hospitals involved. Education and financial support—especially assistance with the cost of medicines—can make a critical difference by enabling patients to engage more consistently with treatment. This finding is highly relevant in Nigeria, where patients usually pay for healthcare directly out of pocket. Education itself is widely recognized as a key determinant of health. For example, the Incheon declaration (UNESCO, 2015) emphasizes that education fosters informed decision-making and healthier lifestyles, while research from high-income settings has shown that adults with lower levels of education consistently report poorer health outcomes (Zajacova & Lawrence, 2018).
In this study, several variables, including age, gender, religion, education, marital status, income, smoking, alcohol intake, and the length of time since diagnosis, significantly correlate with HRQOL. These findings are consistent with previous evidence that has linked HRQOL to sociodemographic and clinical factors such as age (Obosi & Fatunbi, 2018; Lu et al., 2017; Gebremedhin et al., 2019), gender (Manjunath et al., 2014; Obosi & Fatunbi, 2018), religion (Obosi & Fatunbi, 2018), education (Obosi & Fatunbi, 2018), marital status (Obosi & Fatunbi, 2018; Pandey et al., 2020), income (Esin et al., 2016), alcohol use (Daeppen et al., 2014; Ortolá et al., 2016), and duration of T2DM (Obosi & Fatunbi, 2018; de Lima et al., 2018). Also, Trikkalinou et al. (2017) emphasized that the QOL of individuals with diabetes is shaped by a combination of social and clinical factors, which may differ across study designs, populations, and methodologies. Altogether, the results highlight the importance of detailed history-taking during patient assessment. For nurses, this means considering not only clinical symptoms but also social context to deliver individualized care and set appropriate priorities for interventions.
In the present study, participants’ age emerged as a notable predictor of HRQOL. This finding is supported by previous research from Egypt (Ibrahim, 2016), which suggests that psychological well-being can improve with advancing age. However, studies in Serbia (Spasić et al., 2014) and Ethiopia (Gebremedhin et al., 2019) show the opposite trend, with younger patients reporting better QoL. This inconsistency likely reflects the complex interplay among aging, perceptions of health, and comorbidities. While aging often brings physiological decline and greater susceptibility to complications such as cardiovascular or renal disease (Al-Aboudi et al., 2015; Gebremariam et al., 2022), the relatively older participants in this study—most of whom had secondary or tertiary education—may have benefited from health literacy and prior experience managing their illness. This finding may explain why age was positively linked with QoL here, a finding also supported by Nwatu et al. (2019), who reported lower QoL scores among younger patients.
Gender differences were also evident, with female participants reporting higher HRQOL across all domains. This observation is consistent with findings from Oman (D’Souza et al., 2016) and Nigeria (Nwatu et al., 2019). However, studies from Botswana (Rwegerera et al., 2017) and Ethiopia (Wonde et al., 2022) reported the reverse. Cultural norms may help explain these differences, as women in many African settings are more likely than men to seek medical help, partly due to their repeated interactions with health services during pregnancy and childbirth. Men, on the other hand, may delay seeking care because of cultural expectations that equate masculinity with strength and independence. Religion was significantly associated only with the social domain of HRQOL. Muslim participants in this study reported higher scores on social relationships, a finding consistent with research from Saudi Arabia (Ali et al., 2013) and systematic reviews suggesting that religious participation can positively influence self-care and glycemic control (Weber & Doolittle, 2023). Faith-based practices may enhance social support networks and foster a sense of community belonging, which, in turn, can improve QoL outcomes.
Furthermore, educational status, particularly having a tertiary education, was positively associated with all HRQOL domains, and this is supported by previous studies in India, Ethiopia, and Turkey, showing that education enhances both psychological and social wellbeing while contributing to better disease management (Sreedevi et al., 2016; Reba et al., 2018; Esen & Aktürk, 2020; Aschalew et al., 2020). Educated patients understand key information about DM and appropriately comply with self-management advice. This knowledge may help prevent deterioration in glycemic control, prompt early medical advice, detect and manage psychiatric symptomatology, and improve HRQOL. Thus, higher educational status can significantly improve patients’ HRQOL (Pandey et al., 2020). Since education is also closely tied to income, higher educational attainment may provide patients with the financial means to access and sustain appropriate treatment, thereby further enhancing their QoL.
Marital status was positively associated with HRQOL across all domains, consistent with previous studies that posit that social and emotional support from a partner can buffer the psychological and economic burdens of living with a chronic condition (Papazafiropoulou et al., 2015; Aschalew et al., 2020). Likewise, participants with higher monthly income (above ₦30000) reported better HRQOL across all 4 HRQOL domains, a finding supported by previous studies (Esin et al., 2016; Amin et al., 2022), reflecting the role of financial stability in enabling access to care in resource-constrained settings like Nigeria.
Lifestyle factors such as smoking and alcohol consumption were strongly linked to poorer HRQOL. Smoking has a consistent and statistically significant negative effect on all measured aspects of QoL in this study population. The negative beta values mean smokers report poorer physical, mental, social, and environmental health compared to non-smokers. These findings align with previous studies linking cigarette smoking to self-reported reductions in overall health, including deteriorated mental and physical wellbeing and increased limitations in daily activities (Mody & Smith, 2006; Habib et al., 2024). Panahi et al. (2024), using the SF-12 questionnaire, found that current smokers had significantly poorer mental health scores. Likewise, earlier studies have shown that smoking and alcohol use can lead to feelings of social stigma among patients, which may further diminish QoL. These social factors likely contribute to the overall reduction in wellbeing observed among affected individuals (Aschalew et al., 2020; Feyisa et al., 2020).
The present study revealed that alcohol consumption is negatively associated with all domains of the HRQOL scale. The result connotes that the more a patient consumes alcohol, the poorer the HRQOL. This finding aligns with earlier research showing that people who drink moderately to heavily tend to have poorer HRQOL (mental health) compared to those who do not drink or only drink occasionally (Daeppen et al., 2014; Ortolá et al., 2016). The researcher opined that the sociocultural pattern of alcohol use among the study participants may have affected their HRQOL. Alcohol consumption can potentially impair cognition and alter an individual’s consciousness. It impairs glycemic control, which may result in worrying about glucose levels, depression, complications, and reduced satisfaction with an individual’s HRQOL (Aschalew et al., 2020).
Finally, disease duration negatively impacted HRQOL, with patients living with T2DM for more than a decade reporting poorer outcomes across domains. This finding aligns with research from Ethiopia (Gebremedhin et al., 2019), Serbia (Spasić et al., 2014), and Malaysia (Chew et al., 2015), which found that longer disease duration was associated with increased complications and treatment fatigue. In contrast, a study from Nepal (Mishra et al., 2015) suggested longer disease duration might allow patients to adapt, though such findings may reflect contextual differences. Nonetheless, the progressive complications associated with diabetes often weigh heavily on patients’ physical and psychological health over time.
Limitations of this study may affect the generalizability of the findings. These limitations include the study’s cross-sectional design, which limits the ability to establish causal relationships, and reliance on self-report data, which increases the risk of bias. The relatively small sample size and limited geographic scope may also limit the generalizability of the findings to a broader population of patients with T2DM.
Conclusion
The present study’s results revealed moderately high HRQOL among patients with T2DM, with mean scores above the midpoint across all domains—physical health, psychological health, social relationships, and environmental health—indicating generally positive perceptions of wellbeing and satisfaction with their HRQOL and health status. Significant positive sociodemographic correlates of HRQOL were age, gender (female), religion (Islam), educational status (tertiary), marital status (married), and monthly income (>₦30000). Conversely, smoking, alcohol consumption, and longer duration of living with T2DM were consistently associated with poorer HRQOL across all domains. Overall, these results emphasize the multifaceted nature of QoL among people with T2DM and underscore the importance of addressing sociodemographic and clinical factors in comprehensive diabetes care. Interventions tailored to improve lifestyle behaviors and support vulnerable groups need to be studied to enhance overall HRQOL in this population.
Ethical Considerations
Compliance with ethical guidelines
Ethical approval was obtained from the Babcock University Health Research Ethics Committee (BUHREC) (Code: BUHREC667/22), and from the Olabisi Onabanjo University Teaching Hospital (OOUTH)Health Research Ethics Committee (Code: OOUTH/HREC/557/2022AP). Participation in the study was voluntary, and participants had the right to withdraw at any time without feeling pressured to continue, with no negative consequences. Participants gave their informed consent before the study began. The principle of confidentiality and anonymity of all participants was respected. Only researchers approved by BUHREC and OOUTH-HREC were allowed to access the study data. The researcher also ensured that all institutional data privacy protocols were strictly followed.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Data collection, analysis, and interpretation: Christian Asonye; Review and editing: Foluso Ojewole; Conceptualization, study design, writing the original draft and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank the participants, RAs, and the staff of Babcock University Teaching Hospital (BUTH), Ilisan Remo, Ogun State, Nigeria, and Olabisi Onabanjo University Teaching Hospital (OOUTH), Sagamu, Nigeria, for their cooperation and assistance throughout this study.
References
Ababio, G. K., et al., 2017. Predictors of quality of life in patients with diabetes mellitus in two tertiary health institutions in Ghana and Nigeria. The Nigerian Postgraduate Medical Journal, 24(1), pp. 48-55. [DOI:10.4103/npmj.npmj_3_17] [PMID]
Abbasi-Ghahramanloo, A., et al., 2020. Comparison of SF-36 and WHOQoL-BREF in Measuring Quality of Life in Patients with Type 2 Diabetes. International Journal of General Medicine, 13, pp. 497-506. [DOI:10.2147/IJGM.S258953] [PMID]
Al-Aboudi, I. S., et al., 2015. A cross-sectional assessment of health-related quality of life among type 2 diabetes patients in Riyadh, Saudi Arabia. SAGE Open Medicine, 3, pp. 2050312115610129. [DOI:10.1177/2050312115610129] [PMID]
Al Hayek, A. A., et al., 2014. Factors Associated with Health-Related Quality of Life among Saudi Patients with Type 2 Diabetes Mellitus: A cross-sectional survey. Diabetes & Metabolism Journal, 38(3), pp. 220-9. [DOI:10.4093/dmj.2014.38.3.220] [PMID]
Ali Alzahrani, H. & Sehlo, M. G., 2013. The impact of religious connectedness on health-related quality of life in patients with diabetic foot ulcers. Journal of Religion and Health, 52(3), pp. 840-50. [DOI:10.1007/s10943-011-9529-x] [PMID]
Altınok, A., Marakoğlu, K. & Kargın, N., 2016. Evaluation of quality of life and depression levels in individuals with Type 2 diabetes. Journal of Family Medicine and Primary Care, 5(2), pp. 302-8. [DOI:10.4103/2249-4863.192358] [PMID]
Amin, M. F., et al., 2022. Assessment of quality of life and its determinants in type-2 diabetes patients using the WHOQOL-BREF instrument in Bangladesh. BMC Endocrine Disorders, 22(1), pp. 162. [DOI:10.1186/s12902-022-01072-w] [PMID]
Aschalew, A. Y., Yitayal, M. & Minyihun, A., 2020. Health-related quality of life and associated factors among patients with diabetes mellitus at the University of Gondar referral hospital. Health and Quality of Life Outcomes, 18(1), pp. 62. [DOI:10.1186/s12955-020-01311-5] [PMID]
Asonye, C. C. & Ojewole, F., 2023. Self-Care Behaviour: The Life-Changing Magic in Type 2 Diabetes Mellitus Care. African Journal of Health, Nursing and Midwifery, 6(2), pp. 112-22. [DOI:10.52589/ajhnm]
Chew, B. H., Mohd-Sidik, S. & Shariff-Ghazali, S., 2015. Negative effects of diabetes-related distress on health-related quality of life: an evaluation among the adult patients with type 2 diabetes mellitus in three primary healthcare clinics in Malaysia. Health and Quality of Life Outcomes, 13, pp. 187. [DOI:10.1186/s12955-015-0384-4] [PMID]
Ciarambino, T., et al., 2022. Influence of Gender in Diabetes Mellitus and Its Complication. International Journal of Molecular Sciences, 23(16), pp. 8850. [DOI:10.3390/ijms23168850] [PMID]
Daeppen, J. B., et al., 2014. Quality of life depends on the drinking pattern in alcohol-dependent patients. Alcohol and alcoholism (Oxford, Oxfordshire), 49(4), pp. 457-65. [DOI:10.1093/alcalc/agu027] [PMID]
de Lima, L. R., et al., 2018. Quality of life and time since diagnosis of Diabetes Mellitus among the elderly. Revista Brasileira Geriatrics Gerontol, 21, pp. 176-85. [DOI:10.1590/1981-22562018021.170187]
D’Souza, M. S., et al., 2016. Health-related quality of life among Omani men and women with Type 2 Diabetes. Journal of Diabetes Research, 2016, pp. 8293579. [DOI:10.1155/2016/8293579] [PMID]
Esen, İ. & Aktürk, Esen. S., 2020. Health Literacy and Quality of Life in Patients With Type 1 Diabetes Mellitus. Cureus, 12(10), pp. e10860. [DOI:10.7759/cureus.10860] [PMID]
Esin, R., et al., 2016. Quality of life in patients with type 2 diabetes mellitus. Bionanoscience, 6, pp. 502-7. [DOI:10.1007/s12668-016-0261-6]
Fadli, A., 2022. The impact of self-management-based care interventions on quality of life in Type 2 Diabetes mellitus patients: A philosophical perspective. medRxiv, pp. 2022-06. [Link]
Feyisa, B. R., Yilma, M. T. & Tolessa, B. E., 2020. Predictors of health-related quality of life among patients with diabetes on follow-up at Nekemte specialised Hospital, Western Ethiopia: A cross-sectional study. BMJ open, 10(7), pp. e036106. [DOI:10.1136/bmjopen-2019-036106] [PMID]
Garratt, A. M., Schmidt, L. & Fitzpatrick, R., 2002. Patient-assessed health outcome measures for diabetes: A structured review. Diabetic Medicine, 19(1), pp. 1-11. [DOI:10.1046/j.1464-5491.2002.00650.x] [PMID]
Gebremedhin, T., Workicho, A. & Angaw, D. A., 2019. Health-related quality of life and its associated factors among adult patients with type II diabetes attending Mizan Tepi University Teaching Hospital, Southwest Ethiopia. BMJ Open Diabetes Research & Care, 7(1), pp. e000577. [DOI:10.1136/bmjdrc-2018-000577] [PMID]
Gebremariam, G. T., et al., 2022. Health-related quality of life of patients with type 2 diabetes mellitus at a tertiary care hospital in Ethiopia. Plos One, 17, pp. 1-15. [PMID]
Gezawa, I. D., et al., 2015. Socio-demographic and anthropometric risk factors for type 2 diabetes in Maiduguri, North-Eastern Nigeria. Sahel Medical Journal, 18(Suppl 1), pp. S1-7. [Link]
Habib, M. A., et al., 2024. Exploring the impact of smoking on mental health: A cross-sectional analysis in a district-level university in Bangladesh. Public Health and Toxicology, 4(1), pp. 5. [DOI:10.18332/pht/189225]
Harper, A, Power, M & WHOQOL Group, X., 1998. Development of the World Health Organization WHOQOL-BREF quality of life assessment. The WHOQOL Group. Psychological Medicine, 28(3), pp. 551–8. [DOI:10.1017/s0033291798006667] [PMID]
Ibrahim, F., 2016. Physical and psychological health domains of QOL in relation to clinical factors of diabetes mellitus in Egypt. International Research Journal of Medical medicine Sciences, 4, pp. 7-16. [Link]
International Diabetes Federation., 2022. IDF Africa Members. Retrieved from: [Link]
International Diabetes Federation., 2022. Diabetes around the World in 2021. Retrieved from: [Link]
Kayode, O. O., et al., 2015. Pattern of complications and comorbidities among diabetic patients in a tertiary healthcare center in Nigeria. Journal of Clinical Science, 12, pp. 29- 35. [DOI:10.4103/1595-9587.160765]
Kautzky-Willer, A., Leutner, M. & Harreiter, J., 2023. Sex differences in type 2 diabetes. Diabetologia, 66(6), pp. 986-1002. [DOI:10.1007/s00125-023-05891-x] [PMID]
Leslie. K., 1965. Survey Sampling. New York: John Wiley & Sons, Inc. [Link]
Lu, Y., et al., 2017. Health-related quality of life in type-2 diabetes patients: a cross-sectional study in East China. BMC Endocrine Disorders, 17(1), pp. 38. [DOI:10.1186/s12902-017-0187-1] [PMID]
Magliano, D. J. & Boyko, E. J., 2021. IDF Diabetes Atlas 10th edition. Brussels: International Diabetes Federation. [Link]
Malini, H., et al. (2022). Self-Care And Quality of Life People With Type 2 Diabetes During the Covid-19: Cross-Sectional Study. Journal of Diabetes and Metabolic Disorders, 21(1), pp. 785-90. [DOI:10.1007/s40200-022-01055-7] [PMID]
Manjunath, K., et al., 2014. Quality of life of a patient with type 2 diabetes: A cross-sectional study in rural South India. Journal of Family Medicine and Primary Care, 3(4), pp. 396-9. [DOI:10.4103/2249-4863.148124] [PMID]
Mishra, S. R., et al., 2015. Depression and Health-Related Quality of Life among Patients with Type 2 Diabetes Mellitus: A Cross-Sectional Study in Nepal. Plos One, 10(11), pp. e0141385. [DOI:10.1371/journal.pone.0141385] [PMID]
Mody, R. R. & Smith, M. J., 2006. Smoking status and health-related quality of life: Findings from the 2001 Behavioral Risk Factor Surveillance System data. American Journal of Health Promotion, 20(4), pp. 251-8. [DOI:10.4278/0890-1171-20.4.251] [PMID]
Nwatu, C. B., et al., 2019. Health related quality of life in nigerians with complicated diabetes mellitus - a study from Enugu, South East Nigeria. Nigerian Journal of Medicine, 28(2), pp. 138-47. [DOI:10.4103/1115-2613.278574]
Obosi, A. C. & Fatunbi, A. M., 2018. Psychosocial Predictors of Health-Related Quality of Life among Diabetes Patient 1 and 2. Journal of Diabetes and Clinical Practice, 1, pp. 106. [Link]
Ortolá, R., et al., 2016. Patterns of alcohol consumption and health-related quality of life in older adults. Drug and alcohol dependence, 159, pp. 166-73. [DOI:10.1016/j.drugalcdep.2015.12.012] [PMID]
Panahi, N., et al., 2024. The association between quality of life and diabetes: The Bushehr Elderly Health Program. BMC Geriatrics, 24, pp. 267. [DOI:10.1186/s12877-024-04878-6] [PMID]
Pandey, S., et al., 2020. Quality of life using WHOQOL-BREF of Patients with Type 2 Diabetes mellitus attending a Primary Health Centre of Patna, India. Indian Journal of Preventive and Social Medicine, 51(3), pp. 151-7. [Link]
Papazafiropoulou, A. K., et al., 2015. Diabetes-dependent quality of life (ADDQOL) and affecting factors in patients with diabetes mellitus type 2 in Greece. BMC Research Notes, 8, pp. 786. [DOI:10.1186/s13104-015-1782-8] [PMID]
Puspasari, S. & Farera, D. R., 2021. Quality of life among patients with type 2 diabetic mellitus in outpatient department, general public hospital, West Java. International Journal Caring Science, 14, pp. 897-906. [DOI:10.18502/kls.v6i1.8767]
Reba, K., et al., 2018. Health-related quality of life of patients with diagnosed type 2 diabetes in Felege Hiwot Referral Hospital, North West Ethiopia: A cross-sectional study. BMC Research Notes, 11, pp. 544. [DOI:10.1186/s13104-018-3625-x] [PMID]
Roglic, G., 2016. WHO Global report on diabetes: A summary. International Journal of Noncommunicable Diseases, 1(1), pp. 3. [DOI:10.4103/2468-8827.184853]
Rwegerera, G. M., et al., 2017. Health-related quality of life and associated factors among patients with diabetes mellitus in Botswana. Alexandria Journal of Medicine, 54(2), pp. 111-8. [Link]
Saeedi, P., et al., 2020. Mortality attributable to diabetes in 20-79 years old adults, 2019 estimates: Results from the International Diabetes Federation Diabetes Atlas. Diabetes Research and Clinical Practice, 162, pp. 108086. [Link]
Spasić, A., et al., 2014. Quality of life in type 2 diabetic patients. Acta Facultatis Medicae Naissensis, 31(3), pp. 193-200. [DOI:10.2478/afmnai-2014-0024]
Sreedevi, A., et al., 2016. Validation of WHOQOL-BREF in Malayalam and Determinants of Quality of Life Among People With Type 2 Diabetes in Kerala, India. Asia-Pacific Journal of Public Health, 28(1 Suppl), pp. 62S-9S. [DOI:10.1177/1010539515605888] [PMID]
Sun, H., et al., 2021. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Research and Clinical Practice, 183, pp. 109119. [DOI:10.1016/j.diabres.2021.109119] [PMID]
Taylor, V. R., 2000. Measuring healthy days: Population assessment of health-related quality of life. Georgia: U.S. Department of Health And Human Services. [Link]
Trikkalinou, A., Papazafiropoulou, A. K. & Melidonis, A., 2017. Type 2 diabetes and quality of life. World Journal of Diabetes, 8(4), pp. 120-9. [DOI:10.4239/wjd.v8.i4.120] [PMID]
Uloko, A. E., et al., 2018. Prevalence and risk factors for diabetes mellitus in Nigeria: A systematic review and meta-analysis. Diabetes Therapy, 9(3), pp. 1307-16. [Link]
UNESCO., 2015. Incheon Declaration: Education 2030: Towards Inclusive and Equitable Quality Education and Lifelong Learning for All. Retrieved from: [Link]
Weber, J. M. & Doolittle, B. R., 2023. Religion, spirituality and improved glycemic control among people with type 2 diabetes: A systematic review. The International Journal of Psychiatry in Medicine, 58(6), pp. 617-36. [DOI:10.1177/00912174231176171] [PMID]
WHOQoL Group., 1994. The development of the World Health Organization quality of life assessment instrument (the WHOQOL). In Quality of Life Assessment: International Perspectives: Proceedings of the Joint-Meeting Organized by the World Health Organization and the Fondation IPSEN in Paris, July 2–3, 1993 (pp. 41-57). Berlin, Heidelberg: Springer Berlin Heidelberg. [Link]
Wonde, T. E., et al., 2022. Health-related quality of life and associated factors among type 2 diabetic adult patients in Debre Markos Referral Hospital, Northwest Ethiopia. Heliyon, 8(8), pp. e10182. [DOI:10.1016/j.heliyon.2022.e10182] [PMID]
World Diabetes Foundation (WDF)., 2018. Enhancing diabetes education and care in Ogun State, WDF15-1257. Retrieved from: [Link]
World Health Organization (WHO)., 2016. Global Report on Diabetes. Geneva:World Health Organization. [Link]
Zajacova, A. & Lawrence, E. M., 2018. The relationship between education and health: Reducing disparities through a contextual approach. Annual Review of Public Health, 39, pp. 273-89. [DOI:10.1146/annurev-publhealth-031816-044628] [PMID]
Type of Study: Research |
Subject:
General
Received: 2024/09/15 | Accepted: 2025/09/2 | Published: 2026/02/25
Received: 2024/09/15 | Accepted: 2025/09/2 | Published: 2026/02/25
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
