Sat, Jan 31, 2026
[Archive]
Volume 11, Issue 3 (Summer 2025)
JCCNC 2025, 11(3): 229-236 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Izadi-Avanji F S, Mohseni-Asl R, Gilasi H. Psychometric Properties of the Persian Version of the Social Health Scale for the Elderly. JCCNC 2025; 11 (3) :229-236
URL: http://jccnc.iums.ac.ir/article-1-705-en.html
URL: http://jccnc.iums.ac.ir/article-1-705-en.html



1- Department of Medical Surgical Nursing, Faculty of Nursing & Midwifery, Kashan University of Medical Sciences, Kashan, Iran. , fs.izadi@gmail.com
2- Trauma Nursing Research Center, Kashan University of Medical Sciences, Kashan, Iran.
3- Department of Biostatistics & Epidemiology, Faculty of Health, Kashan University of Medical Sciences, Kashan, Iran.
2- Trauma Nursing Research Center, Kashan University of Medical Sciences, Kashan, Iran.
3- Department of Biostatistics & Epidemiology, Faculty of Health, Kashan University of Medical Sciences, Kashan, Iran.
Full-Text [PDF 585 kb]
(590 Downloads)
| Abstract (HTML) (1021 Views)
● The SHSE supports healthcare interventions, allowing providers to assess social health and encourage active aging.
● Three items were removed from the scale through rigorous psychometric analysis to align with the Iranian context.
● High reliability (the Cronbach α of 0.92) and stability (intra-class correlation coefficient of 0.79) were achieved.
● The three dimensions of scale (social support, social adjustment, and perceived environmental resources) enable a comprehensive social health assessment for older adults.
● Three items were removed from the scale through rigorous psychometric analysis to align with the Iranian context.
● High reliability (the Cronbach α of 0.92) and stability (intra-class correlation coefficient of 0.79) were achieved.
● The three dimensions of scale (social support, social adjustment, and perceived environmental resources) enable a comprehensive social health assessment for older adults.
Plain Language Summary
This study validated a Persian version of the social health scale for the elderly (SHSE) to assess social health among Iranian older adults. The study confirmed the scale’s reliability and validity after removing three items to improve accuracy. The finalized 22-item SHSE effectively measures social support, social adjustment, and perceived environmental resources. The Persian version of SHSE is a reliable tool for evaluating social health in Iranian older adults.
Full-Text: (272 Views)
Introduction
Social health refers to an individual’s ability to form and maintain positive interpersonal relationships, actively participate in social groups, and feel supported and valued in society. It extends beyond personal connections to encompass social infrastructure, including access to social programs and safe environmental resources. In other words, social health is a critical dimension of overall well-being, focusing on meaningful relationships, social participation, and a sense of belonging (Doyle & Link, 2024).
Social health, as a fundamental dimension of overall health, is crucial for maintaining a balanced social life and fostering social development (Izadi-Avanji et al., 2023). A study in Iran found that older adults with stronger social health exhibited better self-care behaviors (Mohammadi et al., 2017). Older adults with higher social health can adapt better to changing social roles, participate in group activities, and conform to social norms (Hassanpour et al., 2021). Furthermore, higher psychological and social well-being are associated with a lower risk of age-related decline in physical function (Saadeh et al., 2020). A positive correlation has been found between social support and happiness in older adults (Beygi et al., 2023). These findings highlight the significance of social health, psychological support, and the development of an elderly-friendly city (Lalegani, 2024). Therefore, evaluating social health in older people seems crucial.
The literature review identified two existing questionnaires developed to assess social health. The first is the Iranian social health questionnaire, which comprises 7 subscales: Social interaction, social responsibility, conscientiousness, attitude toward society, empathy, family relations, and social participation (Rafiey et al., 2017). The second is the Keyes social well-being questionnaire (Keyes, 1998). Both instruments are general and do not specifically target the social health of older adults. Considering the distinctive characteristics of aging and the critical role of social health in this population, it is essential to use specialized and comprehensive tools for measuring social health in older adults.
Bao et al. (2018) developed the social health scale for the elderly (SHSE), a 25-item tool with 3 subscales: Social adjustment, social support, and perceived environmental resources. This scale demonstrated acceptable validity and reliability. Considering the global growth of the elderly population and the diverse social, economic, and cultural conditions facing Iranian elderly individuals, as well as their impact on their social health, the present study aimed to determine the psychometric properties of the Persian version of the SHSE.
Materials and Methods
This methodological study aimed to examine the psychometric properties of the Persian version of SHSE. The inclusion criteria included being over 60 years old, providing informed consent, demonstrating cognitive health based on the abbreviated mental test (AMT score ≥8), and being capable of answering questions. AMT evaluates elderly patients for possible dementia (Hodkinson, 1972). It has 10 items, and one point is given for each correct answer. In this test, 0–3 is suggestive of severe impairment, 4–7 indicates moderate impairment, and 8 and above is indicative of normal cognitive function.
Multistage cluster sampling was used in this study. Bao et al. (2018), as the instrument developers, assessed the social health of older adults in their research in China using the 25-item SHSE scale. The scale comprises 3 subscales: Social support (12 items), social adjustment (6 items), and perceived environment resources (7 items). The scores range from 5 to 125, with higher scores indicating greater social health. The scale developer has reported optimal validity and reliability for the questionnaire. The Cronbach α coefficient was estimated at 0.79, and the weighted kappa for inter-rater reliability was 0.75. In addition, the root mean square error of approximation (RMSEA), goodness of fit index (GFI), and adjusted GFI (AGFI) were reported as 0.09, 0.97, and 0.93, respectively (Bao et al., 2018).
Fahimian et al. (2023) translated SHSE into Persian based on the model of Wild et al. (2005). In their study, exploratory factor analysis (EFA) confirmed the scale’s three-factor structure, accounting for 39.47% of the total variance in social health. Regarding the face validity, all items had an acceptable impact score. The content validity ratio (CVR) for each item was 0.72, and the content validity index (CVI) for each item was 0.968, both of which were acceptable. Two items had a CVR of less than 0.62, which was retained in the scale to maintain its integrity, given that the scale was translated. Additionally, the Cronbach α of the scale was 0.841, and for the subscales of social adjustment, social support, and perceived environmental resources, the values were 0.771, 0.338, and 0.62, respectively (Fahimian et al., 2023). The low internal consistency of the perceived environment resources subscale and the explained variance warranted a confirmatory factor analysis (CFA).
With permission from the tool developer (Bao et al., 2018), this study evaluated the psychometric properties of the SHSE, including face and content validity, construct validity via EFA and CFA, internal consistency, and stability.
Face validity
To assess face validity, the instrument was administered to 12 older individuals, and their opinions regarding the ambiguity, difficulty in understanding the items, and the relevance of the items to the instrument’s purpose were solicited. In addition, the older adults were asked to rate each item in terms of importance based on a 5-point Likert scale (very important, important, moderately important, somewhat important, and not at all important). An impact score was calculated using the Equation 1:
1. Importance×Frequency (%)=Impact score
Additionally, item scores exceeding 1.5 were subjected to further analysis (Thomas & Harrison, 2020). In this study, all items had an impact score >1.5
Content validity
The CVR and CVI were used to evaluate the content validity of the scale. The instrument was given to 12 experts, including geriatric nurses, gerontologists, and experts in instrument development and evaluation. They were asked to provide their opinions regarding the necessity of each item (CVR) on a 3-point Likert scale (1=not necessary, 2=useful but not necessary, and 3=necessary). The responses were calculated using the related formula and Lawshe table (Ayre & Scally, 2014; Lawshe, 1975). A higher score indicates stronger expert agreement on the items (Marie et al., 2021). In addition, the experts rated the relevance of each item on a four-point Likert scale (CVI). The results showed that only the CVR scores of items 13 and 24 were less than 0.56 based on the Lawshe scale. However, the two items were retained in the instrument. The CVI value for all items was greater than 0.80 (Ebadi et al., 2016; Polit & Beck, 2008).
Construct validity
Construct validity was assessed using CFA. The sample consisted of 200 older adults selected from Ardabil comprehensive health centers in 2023. While there is no definitive consensus on the minimum sample size for structural equation modeling (SEM) and CFA, 200 subjects is a commonly considered benchmark (Munro, 2005; Kline, 2023).
The sample was selected from older adults with a file in urban comprehensive health service centers through multistage cluster sampling. Ardabil has 30 urban comprehensive health centers. First, 35% of centers were selected using simple random sampling, and the number of samples in each center was determined based on the total number of older adults covered, also selected using a simple random method. Then, the older adults were contacted by phone and invited to participate in the study.
After obtaining informed consent, a cognitive test was administered, and participants with an AMT score of 8 or higher were recruited for the study. In the next stage, the SHSE items and the background information questionnaire (with 8 questions on age, sex, marital status, underlying disease, occupation, education, income, and number of children) were read aloud to the older adults, and their responses were recorded.
Internal consistency was assessed by calculating Cronbach α coefficients of the samples in the CFA. To examine stability, the test re-test method was employed with 20 older adults selected by convenience sampling. Participants completed the questionnaire at two-week intervals (Dutil et al., 2017). The intraclass correlation coefficient (ICC) between scores from the two assessments was calculated, and the internal consistency score above 0.7 was considered satisfactory (Polit & Beck, 2020). Additionally, the standard error of measurement (SEM) was calculated based on the type of agreement and the smallest detectable change (SDC) (van Kampen et al., 2013).
Data analysis
Data analysis was conducted using SPSS software, version 16 and AMOS software, version 23.0. The construct validity was tested by applying EFA and CFA. The Kaiser–Meyer–Olkin (KMO) test was used to determine the sampling adequacy of the data. Bartlett’s test of sphericity revealed a correlation in the data. EFA was run using the principal component analysis (PCA) method and the varimax rotation technique to extract factors. The eigenvalue >1.0 was considered to explain the total variance. Factor loadings <0.3 were suppressed. The Cronbach α coefficient was used to assess internal consistency, while the intra-class correlation coefficient was employed to evaluate inter-rater reliability. SEM and SDC were calculated with the Equation 2:
2. SEM=SD×(1-ICC), SDC=1.96×√2×SEM)
Fit indices included the chi-square distribution, normed fit index (NFI), non-NFI (NNFI), comparative fit index (CFI), GFI, RMSEA, Akaike information criterion (AIC), and expected cross-validation index (ECVI). A significance level of <0.05 was considered statistically significant.
Results
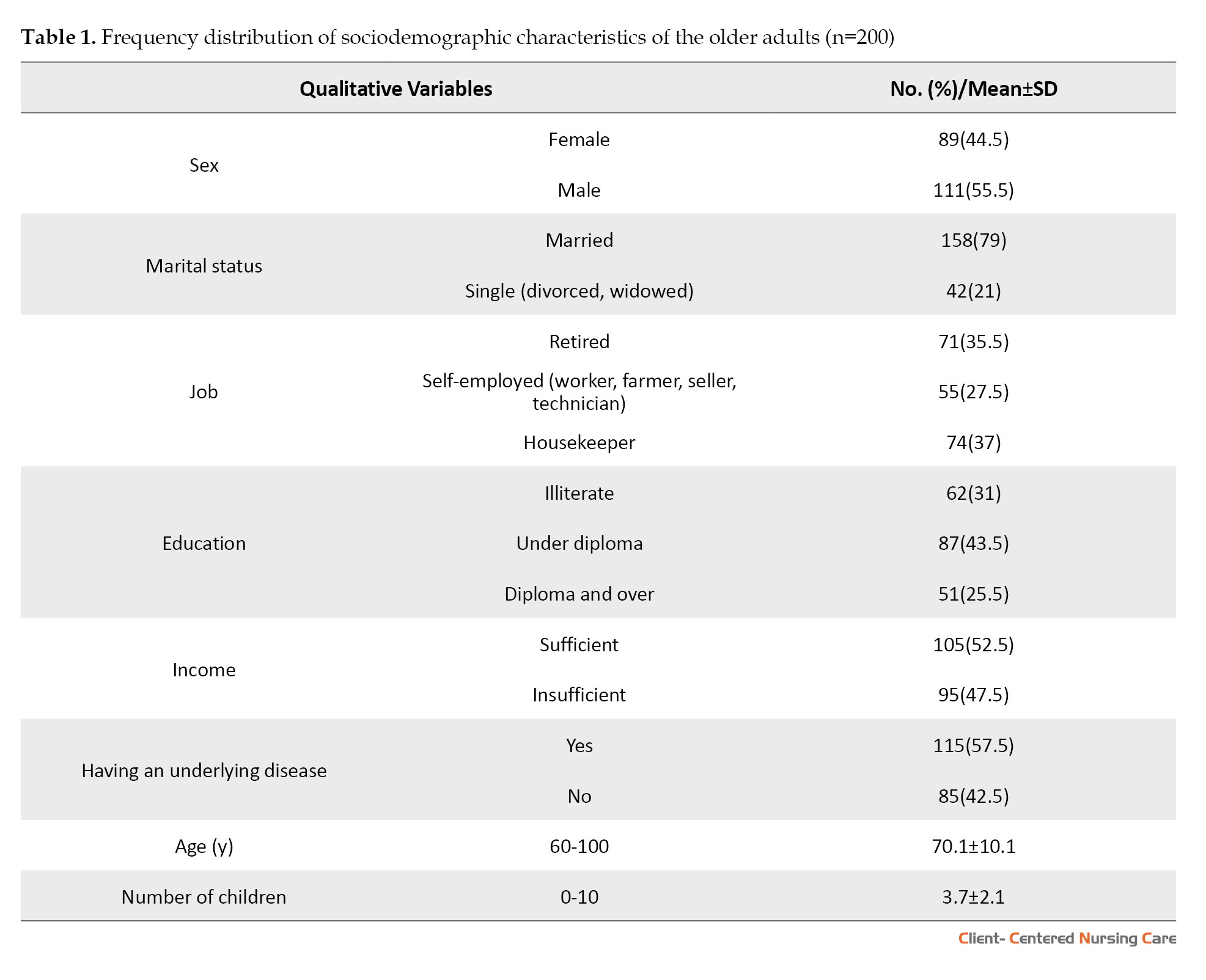
The mean age of the older adults was 70.1±10.1 years, with a range of 60 to 100 years. Furthermore, 115 participants (57.5%) had at least one chronic disease. Table 1 summarizes the demographic characteristics of the sample.
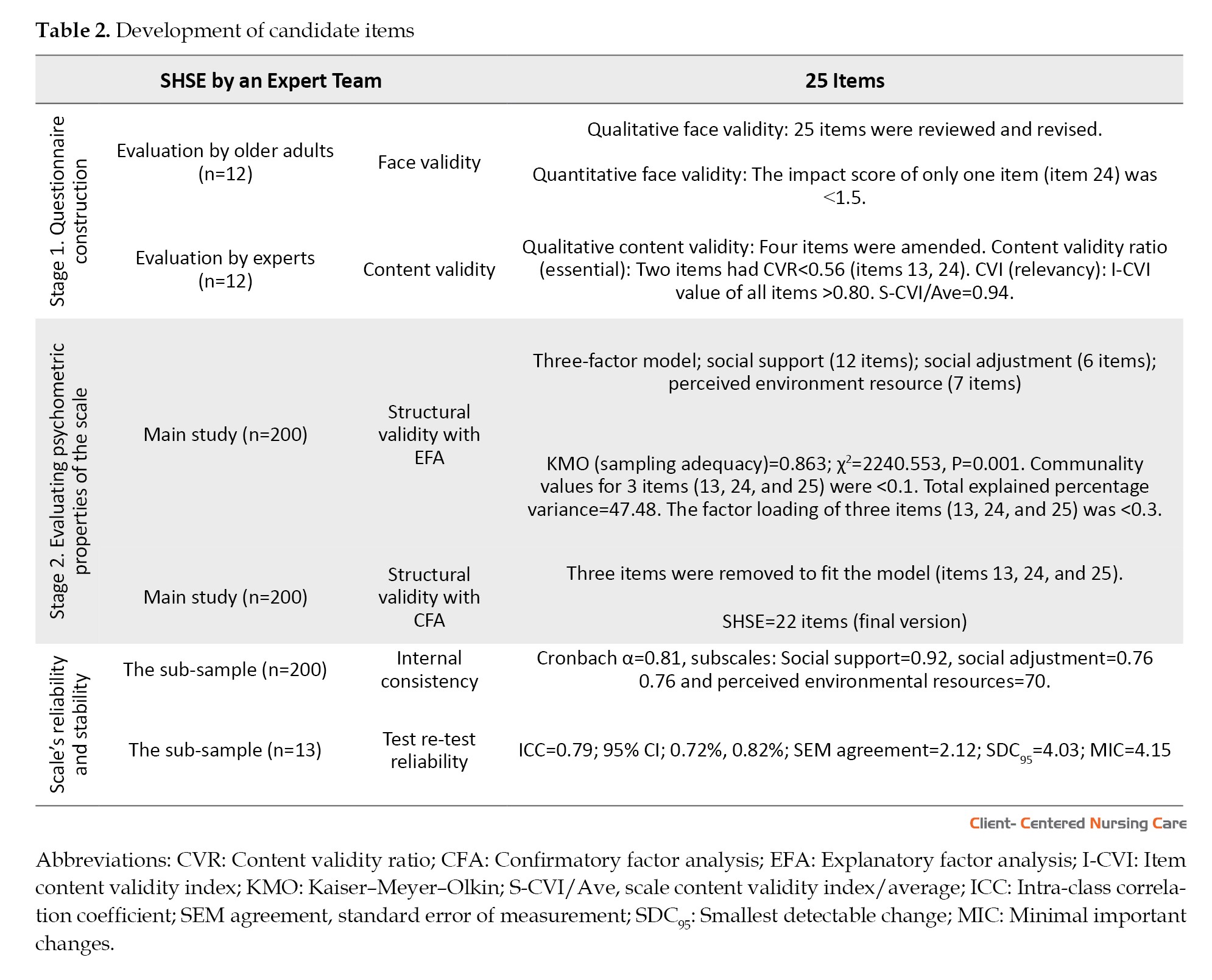
CVR analysis, using the Lawshe table and expert review, revealed a minimum item score of 0.56. The scale-CVI (S-CVI) was 0.94, with individual scores of 0.80 for fluency, 0.86 for clarity, and 0.89 for relevance.
Before performing CAF, EFA was conducted using the PCA method and varimax rotation. The KMO measure and Bartlett’s test confirmed the sampling adequacy. An eigenvalue <1 was used to determine the number of factors in the scale. EFA identified three factors that explained 47% of the total variance of the scale (Table 2).
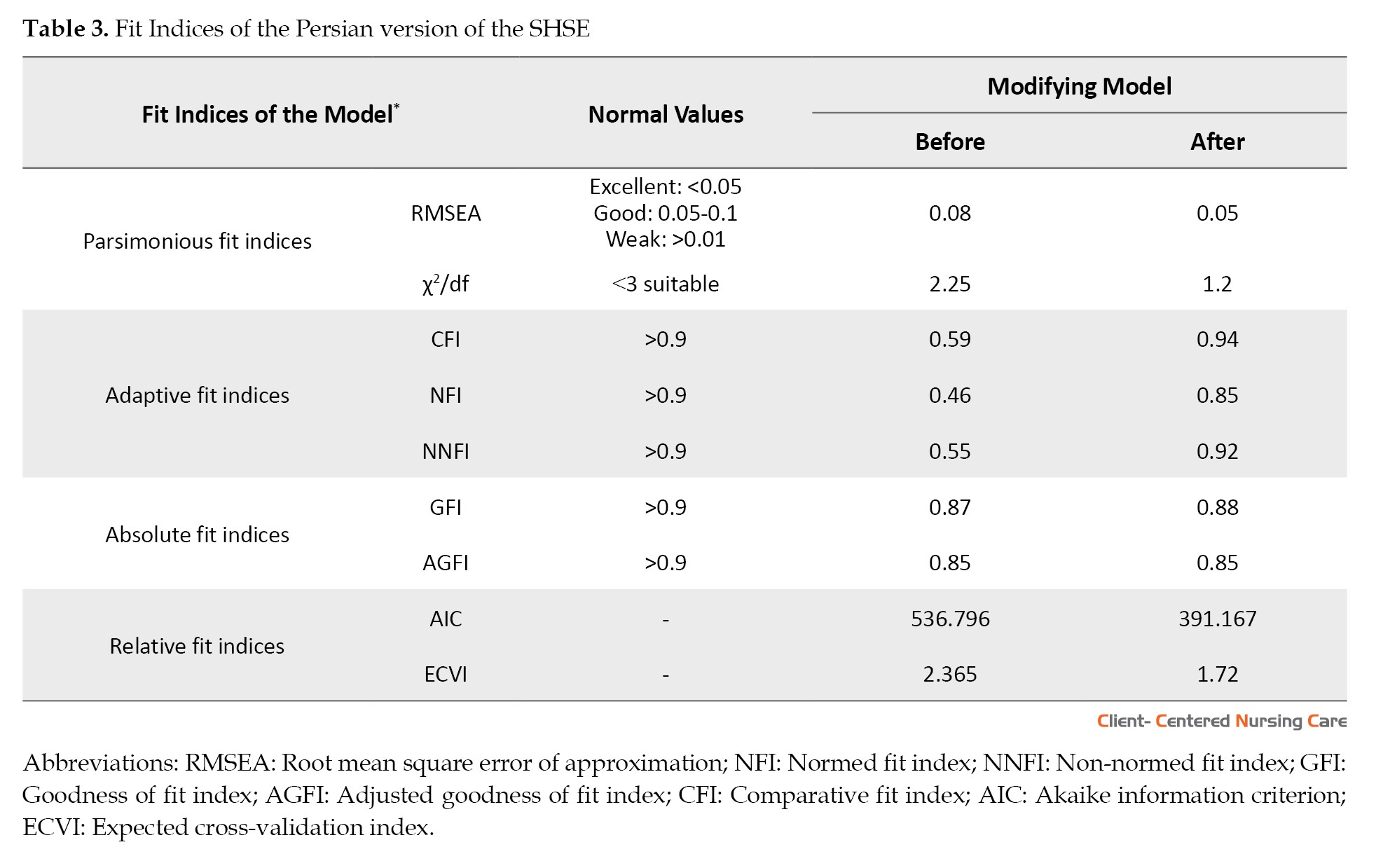
Construct validity was assessed using CFA, with results indicating a moderately good model fit as evidenced by a CFI of 0.59 and RMSEA of 0.08 (Table 3).
Given the low correlations of items 13 (social support), 24 (social adjustment), and 25 (perceived environmental resources), these items were removed from the CFA model, leading to improved model fit indices. In addition, the impact score of item 13 was less than 1.5, and the CVR values of items 13 and 24 were unacceptable according to the Lawshe table. Therefore, their exclusion from the model was predictable. The scale reliability, as measured by Cronbach α, was 0.81. Subscale reliabilities ranged from 0.70 to 0.92 (Table 2).
The ICC value was also 0.79 (95% CI; 0.72%, 0.82%). This reveals the strong stability of the SHSE over time and the excellent reliability of the scale (Table 2). The SEM value indicated that if the test is repeated for an individual, the resulting score may change by ±2.12, which can be attributed to measurement error. The SDC, measured by the SHSE at a 95% confidence level, was estimated to be 4.03. This figure represents the smallest change in an individual’s scores. The values of SEM and SDC indicate the scale’s ability to detect meaningful changes over time. Thus, the responsiveness of the scale is desirable, as calculated by the minimal important change (MIC) of 4.15. Comparing this value with the SDC, it was determined that the scale is capable of detecting minimally important changes in measuring social health (Table 2).
Scoring
Scoring of the SHSE scale is based on a 5-point Likert scale, as per the instrument developer’s instructions. None of the items is reverse-scored. A higher score indicates greater social health. The score range of the scale is between 22 and 110.
Discussion
The study aimed to psychometrically evaluate the Persian version of the SHSE in an Iranian population. The face validity evaluation, which included expert reviews and feedback from the target group, confirmed the quality of the scale items. The content validity score for each item exceeded 0.80, indicating that the SHSE comprehensively measures the intended construct. The high CVI scores suggest a rigorous process of content and face validation by both experts and the research team (Hemmati Maslak Pak & Hashemlo, 2015).
Bao et al. (2018) focused on face and content validity, this study explored construct validity using CFA. The initial Persian version of the SHSE, comprising 25 items and 3 subscales, exhibited poor fit, with a total variance explained of less than 50%. It has been stated that newly developed instruments should account for at least 60% of the total variance (Beck et al., 2010). Accordingly, three items were excluded to improve model fit. These items included: Item 13, “In the past year, how often have you done chores?” from the social adjustment subscale; item 24, “In the past year, how often have you participated in organized community activities?”; and item 25, “Which public services have been provided to you free of charge in the past year?” from the perceived environment resource subscale. Item 13 was removed due to its very low correlation coefficient, which may reflect prevailing cultural norms whereby males are less likely to engage in chores, while female older adults often rely on support from their children due to physical limitations.
Moreover, retirement often coincides with a decline in physical and mental capabilities, making it more challenging for older adults to engage in daily activities, such as housework (Carmona-Torres et al., 2019). Therefore, the removal of item 13 may be justified.
Items 24 and 25, both related to perceived environmental resources, were also removed due to low correlations. It has been reported that changes in economic and social structures can lead to a decrease in social interaction among older adults, particularly those who have retired and experienced job loss, resulting in a sense of isolation and loneliness. Given the reduced social engagement among older adults and the economic challenges faced by many in Iran, the removal of items 24 and 25, which relate to organized activities and public services, seems reasonable (Farzane & Alizadeh, 2013; Lashkarboloki et al., 2015). The economic sanctions and financial hardships in Iran have limited access to healthcare and other resources for older adults, making these questions less relevant to their experiences (Kim et al., 2020; Miri et al., 2019).
The removal of items 13, 24, and 25 resulted in a well-fitting model for the Persian version of SHSE. This finding is consistent with findings from a similar study by Keyes (Keyes, 1998). His study’s CFA supported our EFA results, and most of the fit indices were deemed optimal. The reliability analysis of the Persian version of the SHSE yielded a coefficient of 0.80 after removing three items. Literature review suggests that an alpha coefficient below 0.60 indicates weak internal consistency. Conversely, values closer to 1.0 suggest stronger internal consistency (Kim et al., 2020). The stability reliability results (ICC=0.79) demonstrated an adequate correlation among the remaining statements. Polit and Beck (2020) generally considered a reliability coefficient above 0.70 satisfactory, while coefficients exceeding 0.8 and 0.9 were considered very good and ideal, respectively (Ebadi et al., 2016). The study by Fahimian et al (2023) on the Persian version of SHSE reported an overall internal consistency of 0.62 and a perceived environment resource subscale score of 0.338, suggesting the need for revision of items related to perceived environment resources. This finding aligns with a previous Iranian study that identified the lowest score for the perceived resources subscale in the current tool (Izadi-Avanji et al., 2023). In our study, removing items with low correlation coefficients (13, 24, and 25) improved internal consistency, likely due to the scale’s original design in China, which may not fully align with the economic and social services available in Iran. The correlation coefficients calculated in our study indicate good stability and repeatability.
Conclusion
The Persian version of the SHSE was confirmed as a valid and reliable instrument in Iranian society by removing 3 items. The SHSE can play a significant role in guiding nursing interventions by providing a comprehensive assessment of the social health of older adults. The scale can help nurses detect the levels of social isolation and loneliness, which are critical risk factors for mental health issues like depression and anxiety. With this information, nurses can design interventions such as social support programs or community engagement activities. Regularly using the scale can help track changes in an older adult’s social health over time. This enables timely interventions if social health deteriorates, ensuring proactive care that leads to improved physical health outcomes, reduced healthcare costs, and a higher quality of life for older adults. It is recommended that a study be conducted to evaluate the validity and reliability of the Persian version of the SHSE in older adults with chronic diseases.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Ethics Committee of Kashan University of Medical Sciences, Kashan, Iran (Code: IR.KAUMS.NUHEPM.REC.1400.005). Participation was voluntary, and all participants signed an informed consent after being informed about the research objectives. Participants were assured that their information would be kept confidential and that they could withdraw from the study at any time. They had the opportunity to be informed about the study’s results.
Funding
This study was extracted from master’s thesis of Rasoul Mohseni-Asl, approved by the Department of Medical Surgical Nursing, Faculty of Nursing & Midwifery, Kashan University of Medical Sciences, Kashan, Iran.
Authors' contributions
Conceptualization, study design, and writing the original draft: Fatemeh Sadat Izadi-Avanji; Data collection: Rasoul Mohseni-Asl; Data analysis and interpretation: Hamidreza Gilasi; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The researchers thank Kashan University of Medical Sciences and all the older adults who participated in the study.
References
Ayre, C. & Scally, A. J., 2014. Critical values for Lawshe’s content validity ratio: Revisiting the original methods of calculation. Measurement and Evaluation in Counseling and Development, 47(1), pp. 79-86. [DOI:10.1177/0748175613513808]
Bao, C., et al., 2018. The development of the social health scale for the elderly. Health and Quality of Life Outcomes, 16(1), pp. 67. [DOI:10.1186/s12955-018-0899-6] [PMID]
Beck, S. L., et al., 2010. Initial psychometric properties of the pain care quality survey (PainCQ). The Journal of Pain, 11(12), pp. 1311-9. [DOI:10.1016/j.jpain.2010.03.008] [PMID]
Beygi, Z., et al., 2023. The relationship between social support and happiness in older adults referred to health centers in Zarrin Shahr, Iran. Heliyon, 9(9), pp. e19529 [DOI:10.1016/j.heliyon.2023.e19529] [PMID]
Carmona-Torres, J. M., et al., 2019. Disability for basic and instrumental activities of daily living in older individuals. Plos One, 14(7), pp. e0220157. [DOI:10.1371/journal.pone.0220157] [PMID]
Doyle, D. M. & Link, B. G., 2024. On social health: History, conceptualization, and population patterning. Health Psychology Review, 18(3), pp. 619–48. [PMID]
Dutil, É., Bottari, C. & Auger, C., 2017. Test‐retest reliability of a measure of Independence in everyday activities: The ADL profile. Occupational Therapy International, 2017, pp. 3014579. [DOI:10.1155/2017/3014579] [PMID]
Ebadi, A., et al., 2017. Principles of scale development in health science. Tehran: Jame-e-Negar, 6(1), pp. 402. [Link]
Fahimian, M., et al., 2023. [Translation and Psychometric Evaluation of the Social Health Scale for the Elderly (SHSE) (Persian)]. Journal of Isfahan Medical School, 41(705), pp. 1-8. [DOI.10.48305/jims.v41.i705.0001]
Farzane, S. & Alizadeh, S., 2013. [Study in social determinants on social health among older people in Babol Town (Persian)]. Journal of Studies of Socio Cultural Development, 2(1), pp. 183-208. [Link]
Hassanpour, T., et al., 2021. Social support and social health. Iranian Journal of War and Public Health, 13(3), pp. 189-93. [Link]
Hemmati Maslak Pak, M. & Hashemlo, L., 2015. [Design and psychometric properties of a self-care questionnaire for the elderly (Persian)]. Iranian Journal of Ageing, 10(3), pp. 120-30. [Link]
Hodkinson, H. M., 1972. Evaluation of a mental test score for assessment of mental impairment in the elderly. Age and Ageing, 1(4), pp. 233-8. [DOI:10.1093/ageing/1.4.233] [PMID]
Izadi-Avanji, F. S., Mohseni-Asl, R. & Gilasi, H., 2023. Social health status and its related factors in older adults. Journal of Holistic Nursing and Midwifery, 33(3), pp. 222-9. [DOI:10.32598/jhnm.33.3.2518]
Keyes, C. L. M., 1998. Social well-being. Social Psychology Quarterly, pp. 121-40. [DOI:10.1037/t13598-000]
Kim, M. J., et al., 2020. Global assessment instrument for quality of nursing doctoral education with a research focus: Validity and reliability study. Nurse Education Today, 91, pp. 104475. [DOI:10.1016/j.nedt.2020.104475] [PMID]
Kline, R. B., 2023. Principles and practice of structural equation modeling. New York: Guilford publications. [Link]
Lalegani, A. 2024. Assessing the social health of the elderly in Tehran: Challenges and strategic solutions. Archives of Gerontology and Geriatrics Plus, 1(4), pp. 100091. [DOI:10.1016/j.aggp.2024.100091]
Lashkarboloki, F., et al., 2015. [Association of demographic, socio-economic features and some health problems with nutritional status in elderly (Persian)]. Iranian Journal of Nutrition Sciences and Food Technology, 9(4), pp. 27-34. [Link]
Lawshe, C., 1975. A quantitative approach to content validity. Personnel Psychology, 28(4), pp. 563-75. [DOI:10.1111/j.1744-6570.1975.tb01393.x]
Miri, N., Maddah, M. & Raghfar, H., 2019. [Aging and economic growth (Persian)]. Iranian Journal of Ageing, 13(5), pp. 626-37. [DOI:10.32598/SIJA.13.Special-Issue.626]
Mohammadi, M., et al., 2017. Assessment of the relationship between spiritual and social health and the self-care ability of elderly people referred to community health centers. Iranian Journal of Nursing and Midwifery Research, 22(6), pp. 471-5. [DOI:10.4103/ijnmr.IJNMR_171_16] [PMID]
Munro, B. H., 2005. Statistical methods for health care research. Philadelphia: Lippincott Williams & Wilkins. [Link]
Polit, D. & Beck, C., 2020. Essentials of nursing research: Appraising evidence for nursing practice. Philadelphia: Lippincott Williams & Wilkins. [Link]
Polit, D. F. & Beck, C. T., 2008. Nursing research: Generating and assessing evidence for nursing practice. Philadelphia: Lippincott Williams & Wilkins. [Link]
Rafiey, H., et al., 2017. Development and validation of the Iranian social health questionnaire (IrSHQ). Journal of Health and Social Sciences, 2(1), pp. 19-30. [Link]
Saadeh, M., et al., 2020. The role of psychological and social well-being on physical function trajectories in older adults. The Journals of Gerontology: Series A, 75(8), pp. 1579-85. [DOI:10.1093/gerona/glaa114] [PMID]
Marie, B., et al., 2021. Developing and establishing content validity of vignettes for health care education and research. Western Journal of Nursing Research, 43(7), pp. 677-85. [DOI:10.1177/0193945920969693] [PMID]
Thomas, K. & Harrison, D. A., 2020. Improving the face validity of a composite endpoint. Critical Care Medicine, 48(2), pp. 257-8. [DOI:10.1097/CCM.0000000000004150] [PMID]
van Kampen, D. A., et al., 2013. Determination and comparison of the smallest detectable change (SDC) and the minimal important change (MIC) of four-shoulder patient-reported outcome measures (PROMs). Journal of Orthopaedic Surgery and Research, 8, pp. 40. [DOI:10.1186/1749-799X-8-40] [PMID]
Wild, D., et al., 2005. Principles of good practice for the translation and cultural adaptation process for patient-reported outcomes (PRO) measures: report of the ISPOR task force for translation and cultural adaptation. Value in Health, 8(2), pp. 94-104. [DOI:10.1111/j.1524-4733.2005.04054.x] [PMID]
Social health refers to an individual’s ability to form and maintain positive interpersonal relationships, actively participate in social groups, and feel supported and valued in society. It extends beyond personal connections to encompass social infrastructure, including access to social programs and safe environmental resources. In other words, social health is a critical dimension of overall well-being, focusing on meaningful relationships, social participation, and a sense of belonging (Doyle & Link, 2024).
Social health, as a fundamental dimension of overall health, is crucial for maintaining a balanced social life and fostering social development (Izadi-Avanji et al., 2023). A study in Iran found that older adults with stronger social health exhibited better self-care behaviors (Mohammadi et al., 2017). Older adults with higher social health can adapt better to changing social roles, participate in group activities, and conform to social norms (Hassanpour et al., 2021). Furthermore, higher psychological and social well-being are associated with a lower risk of age-related decline in physical function (Saadeh et al., 2020). A positive correlation has been found between social support and happiness in older adults (Beygi et al., 2023). These findings highlight the significance of social health, psychological support, and the development of an elderly-friendly city (Lalegani, 2024). Therefore, evaluating social health in older people seems crucial.
The literature review identified two existing questionnaires developed to assess social health. The first is the Iranian social health questionnaire, which comprises 7 subscales: Social interaction, social responsibility, conscientiousness, attitude toward society, empathy, family relations, and social participation (Rafiey et al., 2017). The second is the Keyes social well-being questionnaire (Keyes, 1998). Both instruments are general and do not specifically target the social health of older adults. Considering the distinctive characteristics of aging and the critical role of social health in this population, it is essential to use specialized and comprehensive tools for measuring social health in older adults.
Bao et al. (2018) developed the social health scale for the elderly (SHSE), a 25-item tool with 3 subscales: Social adjustment, social support, and perceived environmental resources. This scale demonstrated acceptable validity and reliability. Considering the global growth of the elderly population and the diverse social, economic, and cultural conditions facing Iranian elderly individuals, as well as their impact on their social health, the present study aimed to determine the psychometric properties of the Persian version of the SHSE.
Materials and Methods
This methodological study aimed to examine the psychometric properties of the Persian version of SHSE. The inclusion criteria included being over 60 years old, providing informed consent, demonstrating cognitive health based on the abbreviated mental test (AMT score ≥8), and being capable of answering questions. AMT evaluates elderly patients for possible dementia (Hodkinson, 1972). It has 10 items, and one point is given for each correct answer. In this test, 0–3 is suggestive of severe impairment, 4–7 indicates moderate impairment, and 8 and above is indicative of normal cognitive function.
Multistage cluster sampling was used in this study. Bao et al. (2018), as the instrument developers, assessed the social health of older adults in their research in China using the 25-item SHSE scale. The scale comprises 3 subscales: Social support (12 items), social adjustment (6 items), and perceived environment resources (7 items). The scores range from 5 to 125, with higher scores indicating greater social health. The scale developer has reported optimal validity and reliability for the questionnaire. The Cronbach α coefficient was estimated at 0.79, and the weighted kappa for inter-rater reliability was 0.75. In addition, the root mean square error of approximation (RMSEA), goodness of fit index (GFI), and adjusted GFI (AGFI) were reported as 0.09, 0.97, and 0.93, respectively (Bao et al., 2018).
Fahimian et al. (2023) translated SHSE into Persian based on the model of Wild et al. (2005). In their study, exploratory factor analysis (EFA) confirmed the scale’s three-factor structure, accounting for 39.47% of the total variance in social health. Regarding the face validity, all items had an acceptable impact score. The content validity ratio (CVR) for each item was 0.72, and the content validity index (CVI) for each item was 0.968, both of which were acceptable. Two items had a CVR of less than 0.62, which was retained in the scale to maintain its integrity, given that the scale was translated. Additionally, the Cronbach α of the scale was 0.841, and for the subscales of social adjustment, social support, and perceived environmental resources, the values were 0.771, 0.338, and 0.62, respectively (Fahimian et al., 2023). The low internal consistency of the perceived environment resources subscale and the explained variance warranted a confirmatory factor analysis (CFA).
With permission from the tool developer (Bao et al., 2018), this study evaluated the psychometric properties of the SHSE, including face and content validity, construct validity via EFA and CFA, internal consistency, and stability.
Face validity
To assess face validity, the instrument was administered to 12 older individuals, and their opinions regarding the ambiguity, difficulty in understanding the items, and the relevance of the items to the instrument’s purpose were solicited. In addition, the older adults were asked to rate each item in terms of importance based on a 5-point Likert scale (very important, important, moderately important, somewhat important, and not at all important). An impact score was calculated using the Equation 1:
1. Importance×Frequency (%)=Impact score
Additionally, item scores exceeding 1.5 were subjected to further analysis (Thomas & Harrison, 2020). In this study, all items had an impact score >1.5
Content validity
The CVR and CVI were used to evaluate the content validity of the scale. The instrument was given to 12 experts, including geriatric nurses, gerontologists, and experts in instrument development and evaluation. They were asked to provide their opinions regarding the necessity of each item (CVR) on a 3-point Likert scale (1=not necessary, 2=useful but not necessary, and 3=necessary). The responses were calculated using the related formula and Lawshe table (Ayre & Scally, 2014; Lawshe, 1975). A higher score indicates stronger expert agreement on the items (Marie et al., 2021). In addition, the experts rated the relevance of each item on a four-point Likert scale (CVI). The results showed that only the CVR scores of items 13 and 24 were less than 0.56 based on the Lawshe scale. However, the two items were retained in the instrument. The CVI value for all items was greater than 0.80 (Ebadi et al., 2016; Polit & Beck, 2008).
Construct validity
Construct validity was assessed using CFA. The sample consisted of 200 older adults selected from Ardabil comprehensive health centers in 2023. While there is no definitive consensus on the minimum sample size for structural equation modeling (SEM) and CFA, 200 subjects is a commonly considered benchmark (Munro, 2005; Kline, 2023).
The sample was selected from older adults with a file in urban comprehensive health service centers through multistage cluster sampling. Ardabil has 30 urban comprehensive health centers. First, 35% of centers were selected using simple random sampling, and the number of samples in each center was determined based on the total number of older adults covered, also selected using a simple random method. Then, the older adults were contacted by phone and invited to participate in the study.
After obtaining informed consent, a cognitive test was administered, and participants with an AMT score of 8 or higher were recruited for the study. In the next stage, the SHSE items and the background information questionnaire (with 8 questions on age, sex, marital status, underlying disease, occupation, education, income, and number of children) were read aloud to the older adults, and their responses were recorded.
Internal consistency was assessed by calculating Cronbach α coefficients of the samples in the CFA. To examine stability, the test re-test method was employed with 20 older adults selected by convenience sampling. Participants completed the questionnaire at two-week intervals (Dutil et al., 2017). The intraclass correlation coefficient (ICC) between scores from the two assessments was calculated, and the internal consistency score above 0.7 was considered satisfactory (Polit & Beck, 2020). Additionally, the standard error of measurement (SEM) was calculated based on the type of agreement and the smallest detectable change (SDC) (van Kampen et al., 2013).
Data analysis
Data analysis was conducted using SPSS software, version 16 and AMOS software, version 23.0. The construct validity was tested by applying EFA and CFA. The Kaiser–Meyer–Olkin (KMO) test was used to determine the sampling adequacy of the data. Bartlett’s test of sphericity revealed a correlation in the data. EFA was run using the principal component analysis (PCA) method and the varimax rotation technique to extract factors. The eigenvalue >1.0 was considered to explain the total variance. Factor loadings <0.3 were suppressed. The Cronbach α coefficient was used to assess internal consistency, while the intra-class correlation coefficient was employed to evaluate inter-rater reliability. SEM and SDC were calculated with the Equation 2:
2. SEM=SD×(1-ICC), SDC=1.96×√2×SEM)
Fit indices included the chi-square distribution, normed fit index (NFI), non-NFI (NNFI), comparative fit index (CFI), GFI, RMSEA, Akaike information criterion (AIC), and expected cross-validation index (ECVI). A significance level of <0.05 was considered statistically significant.
Results
The mean age of the older adults was 70.1±10.1 years, with a range of 60 to 100 years. Furthermore, 115 participants (57.5%) had at least one chronic disease. Table 1 summarizes the demographic characteristics of the sample.
CVR analysis, using the Lawshe table and expert review, revealed a minimum item score of 0.56. The scale-CVI (S-CVI) was 0.94, with individual scores of 0.80 for fluency, 0.86 for clarity, and 0.89 for relevance.
Before performing CAF, EFA was conducted using the PCA method and varimax rotation. The KMO measure and Bartlett’s test confirmed the sampling adequacy. An eigenvalue <1 was used to determine the number of factors in the scale. EFA identified three factors that explained 47% of the total variance of the scale (Table 2).
Construct validity was assessed using CFA, with results indicating a moderately good model fit as evidenced by a CFI of 0.59 and RMSEA of 0.08 (Table 3).
Given the low correlations of items 13 (social support), 24 (social adjustment), and 25 (perceived environmental resources), these items were removed from the CFA model, leading to improved model fit indices. In addition, the impact score of item 13 was less than 1.5, and the CVR values of items 13 and 24 were unacceptable according to the Lawshe table. Therefore, their exclusion from the model was predictable. The scale reliability, as measured by Cronbach α, was 0.81. Subscale reliabilities ranged from 0.70 to 0.92 (Table 2).
The ICC value was also 0.79 (95% CI; 0.72%, 0.82%). This reveals the strong stability of the SHSE over time and the excellent reliability of the scale (Table 2). The SEM value indicated that if the test is repeated for an individual, the resulting score may change by ±2.12, which can be attributed to measurement error. The SDC, measured by the SHSE at a 95% confidence level, was estimated to be 4.03. This figure represents the smallest change in an individual’s scores. The values of SEM and SDC indicate the scale’s ability to detect meaningful changes over time. Thus, the responsiveness of the scale is desirable, as calculated by the minimal important change (MIC) of 4.15. Comparing this value with the SDC, it was determined that the scale is capable of detecting minimally important changes in measuring social health (Table 2).
Scoring
Scoring of the SHSE scale is based on a 5-point Likert scale, as per the instrument developer’s instructions. None of the items is reverse-scored. A higher score indicates greater social health. The score range of the scale is between 22 and 110.
Discussion
The study aimed to psychometrically evaluate the Persian version of the SHSE in an Iranian population. The face validity evaluation, which included expert reviews and feedback from the target group, confirmed the quality of the scale items. The content validity score for each item exceeded 0.80, indicating that the SHSE comprehensively measures the intended construct. The high CVI scores suggest a rigorous process of content and face validation by both experts and the research team (Hemmati Maslak Pak & Hashemlo, 2015).
Bao et al. (2018) focused on face and content validity, this study explored construct validity using CFA. The initial Persian version of the SHSE, comprising 25 items and 3 subscales, exhibited poor fit, with a total variance explained of less than 50%. It has been stated that newly developed instruments should account for at least 60% of the total variance (Beck et al., 2010). Accordingly, three items were excluded to improve model fit. These items included: Item 13, “In the past year, how often have you done chores?” from the social adjustment subscale; item 24, “In the past year, how often have you participated in organized community activities?”; and item 25, “Which public services have been provided to you free of charge in the past year?” from the perceived environment resource subscale. Item 13 was removed due to its very low correlation coefficient, which may reflect prevailing cultural norms whereby males are less likely to engage in chores, while female older adults often rely on support from their children due to physical limitations.
Moreover, retirement often coincides with a decline in physical and mental capabilities, making it more challenging for older adults to engage in daily activities, such as housework (Carmona-Torres et al., 2019). Therefore, the removal of item 13 may be justified.
Items 24 and 25, both related to perceived environmental resources, were also removed due to low correlations. It has been reported that changes in economic and social structures can lead to a decrease in social interaction among older adults, particularly those who have retired and experienced job loss, resulting in a sense of isolation and loneliness. Given the reduced social engagement among older adults and the economic challenges faced by many in Iran, the removal of items 24 and 25, which relate to organized activities and public services, seems reasonable (Farzane & Alizadeh, 2013; Lashkarboloki et al., 2015). The economic sanctions and financial hardships in Iran have limited access to healthcare and other resources for older adults, making these questions less relevant to their experiences (Kim et al., 2020; Miri et al., 2019).
The removal of items 13, 24, and 25 resulted in a well-fitting model for the Persian version of SHSE. This finding is consistent with findings from a similar study by Keyes (Keyes, 1998). His study’s CFA supported our EFA results, and most of the fit indices were deemed optimal. The reliability analysis of the Persian version of the SHSE yielded a coefficient of 0.80 after removing three items. Literature review suggests that an alpha coefficient below 0.60 indicates weak internal consistency. Conversely, values closer to 1.0 suggest stronger internal consistency (Kim et al., 2020). The stability reliability results (ICC=0.79) demonstrated an adequate correlation among the remaining statements. Polit and Beck (2020) generally considered a reliability coefficient above 0.70 satisfactory, while coefficients exceeding 0.8 and 0.9 were considered very good and ideal, respectively (Ebadi et al., 2016). The study by Fahimian et al (2023) on the Persian version of SHSE reported an overall internal consistency of 0.62 and a perceived environment resource subscale score of 0.338, suggesting the need for revision of items related to perceived environment resources. This finding aligns with a previous Iranian study that identified the lowest score for the perceived resources subscale in the current tool (Izadi-Avanji et al., 2023). In our study, removing items with low correlation coefficients (13, 24, and 25) improved internal consistency, likely due to the scale’s original design in China, which may not fully align with the economic and social services available in Iran. The correlation coefficients calculated in our study indicate good stability and repeatability.
Conclusion
The Persian version of the SHSE was confirmed as a valid and reliable instrument in Iranian society by removing 3 items. The SHSE can play a significant role in guiding nursing interventions by providing a comprehensive assessment of the social health of older adults. The scale can help nurses detect the levels of social isolation and loneliness, which are critical risk factors for mental health issues like depression and anxiety. With this information, nurses can design interventions such as social support programs or community engagement activities. Regularly using the scale can help track changes in an older adult’s social health over time. This enables timely interventions if social health deteriorates, ensuring proactive care that leads to improved physical health outcomes, reduced healthcare costs, and a higher quality of life for older adults. It is recommended that a study be conducted to evaluate the validity and reliability of the Persian version of the SHSE in older adults with chronic diseases.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Ethics Committee of Kashan University of Medical Sciences, Kashan, Iran (Code: IR.KAUMS.NUHEPM.REC.1400.005). Participation was voluntary, and all participants signed an informed consent after being informed about the research objectives. Participants were assured that their information would be kept confidential and that they could withdraw from the study at any time. They had the opportunity to be informed about the study’s results.
Funding
This study was extracted from master’s thesis of Rasoul Mohseni-Asl, approved by the Department of Medical Surgical Nursing, Faculty of Nursing & Midwifery, Kashan University of Medical Sciences, Kashan, Iran.
Authors' contributions
Conceptualization, study design, and writing the original draft: Fatemeh Sadat Izadi-Avanji; Data collection: Rasoul Mohseni-Asl; Data analysis and interpretation: Hamidreza Gilasi; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The researchers thank Kashan University of Medical Sciences and all the older adults who participated in the study.
References
Ayre, C. & Scally, A. J., 2014. Critical values for Lawshe’s content validity ratio: Revisiting the original methods of calculation. Measurement and Evaluation in Counseling and Development, 47(1), pp. 79-86. [DOI:10.1177/0748175613513808]
Bao, C., et al., 2018. The development of the social health scale for the elderly. Health and Quality of Life Outcomes, 16(1), pp. 67. [DOI:10.1186/s12955-018-0899-6] [PMID]
Beck, S. L., et al., 2010. Initial psychometric properties of the pain care quality survey (PainCQ). The Journal of Pain, 11(12), pp. 1311-9. [DOI:10.1016/j.jpain.2010.03.008] [PMID]
Beygi, Z., et al., 2023. The relationship between social support and happiness in older adults referred to health centers in Zarrin Shahr, Iran. Heliyon, 9(9), pp. e19529 [DOI:10.1016/j.heliyon.2023.e19529] [PMID]
Carmona-Torres, J. M., et al., 2019. Disability for basic and instrumental activities of daily living in older individuals. Plos One, 14(7), pp. e0220157. [DOI:10.1371/journal.pone.0220157] [PMID]
Doyle, D. M. & Link, B. G., 2024. On social health: History, conceptualization, and population patterning. Health Psychology Review, 18(3), pp. 619–48. [PMID]
Dutil, É., Bottari, C. & Auger, C., 2017. Test‐retest reliability of a measure of Independence in everyday activities: The ADL profile. Occupational Therapy International, 2017, pp. 3014579. [DOI:10.1155/2017/3014579] [PMID]
Ebadi, A., et al., 2017. Principles of scale development in health science. Tehran: Jame-e-Negar, 6(1), pp. 402. [Link]
Fahimian, M., et al., 2023. [Translation and Psychometric Evaluation of the Social Health Scale for the Elderly (SHSE) (Persian)]. Journal of Isfahan Medical School, 41(705), pp. 1-8. [DOI.10.48305/jims.v41.i705.0001]
Farzane, S. & Alizadeh, S., 2013. [Study in social determinants on social health among older people in Babol Town (Persian)]. Journal of Studies of Socio Cultural Development, 2(1), pp. 183-208. [Link]
Hassanpour, T., et al., 2021. Social support and social health. Iranian Journal of War and Public Health, 13(3), pp. 189-93. [Link]
Hemmati Maslak Pak, M. & Hashemlo, L., 2015. [Design and psychometric properties of a self-care questionnaire for the elderly (Persian)]. Iranian Journal of Ageing, 10(3), pp. 120-30. [Link]
Hodkinson, H. M., 1972. Evaluation of a mental test score for assessment of mental impairment in the elderly. Age and Ageing, 1(4), pp. 233-8. [DOI:10.1093/ageing/1.4.233] [PMID]
Izadi-Avanji, F. S., Mohseni-Asl, R. & Gilasi, H., 2023. Social health status and its related factors in older adults. Journal of Holistic Nursing and Midwifery, 33(3), pp. 222-9. [DOI:10.32598/jhnm.33.3.2518]
Keyes, C. L. M., 1998. Social well-being. Social Psychology Quarterly, pp. 121-40. [DOI:10.1037/t13598-000]
Kim, M. J., et al., 2020. Global assessment instrument for quality of nursing doctoral education with a research focus: Validity and reliability study. Nurse Education Today, 91, pp. 104475. [DOI:10.1016/j.nedt.2020.104475] [PMID]
Kline, R. B., 2023. Principles and practice of structural equation modeling. New York: Guilford publications. [Link]
Lalegani, A. 2024. Assessing the social health of the elderly in Tehran: Challenges and strategic solutions. Archives of Gerontology and Geriatrics Plus, 1(4), pp. 100091. [DOI:10.1016/j.aggp.2024.100091]
Lashkarboloki, F., et al., 2015. [Association of demographic, socio-economic features and some health problems with nutritional status in elderly (Persian)]. Iranian Journal of Nutrition Sciences and Food Technology, 9(4), pp. 27-34. [Link]
Lawshe, C., 1975. A quantitative approach to content validity. Personnel Psychology, 28(4), pp. 563-75. [DOI:10.1111/j.1744-6570.1975.tb01393.x]
Miri, N., Maddah, M. & Raghfar, H., 2019. [Aging and economic growth (Persian)]. Iranian Journal of Ageing, 13(5), pp. 626-37. [DOI:10.32598/SIJA.13.Special-Issue.626]
Mohammadi, M., et al., 2017. Assessment of the relationship between spiritual and social health and the self-care ability of elderly people referred to community health centers. Iranian Journal of Nursing and Midwifery Research, 22(6), pp. 471-5. [DOI:10.4103/ijnmr.IJNMR_171_16] [PMID]
Munro, B. H., 2005. Statistical methods for health care research. Philadelphia: Lippincott Williams & Wilkins. [Link]
Polit, D. & Beck, C., 2020. Essentials of nursing research: Appraising evidence for nursing practice. Philadelphia: Lippincott Williams & Wilkins. [Link]
Polit, D. F. & Beck, C. T., 2008. Nursing research: Generating and assessing evidence for nursing practice. Philadelphia: Lippincott Williams & Wilkins. [Link]
Rafiey, H., et al., 2017. Development and validation of the Iranian social health questionnaire (IrSHQ). Journal of Health and Social Sciences, 2(1), pp. 19-30. [Link]
Saadeh, M., et al., 2020. The role of psychological and social well-being on physical function trajectories in older adults. The Journals of Gerontology: Series A, 75(8), pp. 1579-85. [DOI:10.1093/gerona/glaa114] [PMID]
Marie, B., et al., 2021. Developing and establishing content validity of vignettes for health care education and research. Western Journal of Nursing Research, 43(7), pp. 677-85. [DOI:10.1177/0193945920969693] [PMID]
Thomas, K. & Harrison, D. A., 2020. Improving the face validity of a composite endpoint. Critical Care Medicine, 48(2), pp. 257-8. [DOI:10.1097/CCM.0000000000004150] [PMID]
van Kampen, D. A., et al., 2013. Determination and comparison of the smallest detectable change (SDC) and the minimal important change (MIC) of four-shoulder patient-reported outcome measures (PROMs). Journal of Orthopaedic Surgery and Research, 8, pp. 40. [DOI:10.1186/1749-799X-8-40] [PMID]
Wild, D., et al., 2005. Principles of good practice for the translation and cultural adaptation process for patient-reported outcomes (PRO) measures: report of the ISPOR task force for translation and cultural adaptation. Value in Health, 8(2), pp. 94-104. [DOI:10.1111/j.1524-4733.2005.04054.x] [PMID]
Type of Study: Research |
Subject:
General
Received: 2024/11/4 | Accepted: 2025/02/2 | Published: 2025/08/1
Received: 2024/11/4 | Accepted: 2025/02/2 | Published: 2025/08/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
