Tue, Apr 28, 2026
[Archive]
Volume 12, Issue 1 (Winter 2026)
JCCNC 2026, 12(1): 1-18 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Izzati Salim F, Hariati S, Masyitha Irwan A, Erfina E. Shared Decision-making for Cancer Treatment: A Scoping Review. JCCNC 2026; 12 (1) :1-18
URL: http://jccnc.iums.ac.ir/article-1-740-en.html
URL: http://jccnc.iums.ac.ir/article-1-740-en.html



1- Department of Nursing, Faculty of Nursing, Hasanuddin University, Makassar, Indonesia.
2- Department of Pediatric Nursing, Faculty of Nursing, Hasanuddin University, Makassar, Indonesia. ,sunihariati@unhas.ac.id
3- Department of Gerontological Nursing, Faculty of Nursing, Hasanuddin University, Makassar, Indonesia.
4- Department of Maternal Health Nursing, Faculty of Nursing, Hasanuddin University, Makassar, Indonesia.
2- Department of Pediatric Nursing, Faculty of Nursing, Hasanuddin University, Makassar, Indonesia. ,
3- Department of Gerontological Nursing, Faculty of Nursing, Hasanuddin University, Makassar, Indonesia.
4- Department of Maternal Health Nursing, Faculty of Nursing, Hasanuddin University, Makassar, Indonesia.
Full-Text [PDF 930 kb]
(395 Downloads)
| Abstract (HTML) (412 Views)
Full-Text: (19 Views)
Introduction
Cancer is a critical global health challenge among non-communicable diseases, characterized by uncontrolled cellular proliferation that may invade surrounding tissues and metastasize (Magnusson, 2020; American Cancer Society, 2024). The incidence of new cancer cases worldwide rose from 18.1 million in 2018 to 19.3 million in 2020, resulting in nearly 10 million deaths across all age groups, and projections indicate an increase of 61.3% by 2040 (WHO, 2022). Given the high and escalating prevalence of cancer, making informed treatment decisions is imperative. A cancer diagnosis profoundly affects patients and their families, impacting not only physical health but also emotional, social, and financial wellbeing (Khullar et al., 2018). Patients must navigate numerous uncertainties related to diagnostic procedures, complex treatment regimens, remission, palliative care, and unpredictable disease outcomes, a process that can recur throughout their lives (Stone & Olsen, 2022). These challenges significantly influence the patient's quality of life (QoL) and can lead to heightened levels of stress, anxiety, and depression (Pitman et al., 2018). Therefore, the decision-making process surrounding treatment options is a vital component of the patient's journey through illness.
The decision-making process in healthcare involves a collaborative effort among the patient, their family, and the medical team to identify treatment options that align with the patient's preferences and needs, based on available information (Tariman et al., 2012). An increasing recognition of its significance drives this shift towards a more patient-centered approach (Zucca et al., 2014). Engaging patients more actively in clinical decision-making can enable healthcare providers to accept choices that may not align with their professional judgments but that the patient is willing to pursue (Légaré & Witteman, 2013). Consequently, adopting effective decision-making models in clinical settings could be a beneficial strategy for helping cancer patients evaluate their treatment options.
Previous reviews of decision-making in cancer care have typically focused on specific aspects of the process, such as particular age groups or healthcare providers. For instance, Dijkman et al. (2022) examined treatment preferences among older adults, and Spronk et al. (2018) investigated the availability and effectiveness of shared decision-making (SDM) tools. However, this study was limited to metastatic breast cancer patients. Neither review addressed cancer patients more broadly. Meanwhile, Pinker and Pilleron (2023) focused on the role of healthcare providers in patient decision-making. Similarly, Covvey et al. (2019) explored the barriers and facilitators of SDM in oncology, identifying factors such as patient characteristics, physician roles, and health system influences. However, a comprehensive review that integrates the involvement of patients, families, and healthcare professionals (HCPs) in the SDM process has not yet been conducted.
In contrast to previous studies, this scoping review focuses on cancer patients in general, across diverse clinical settings, rather than limiting its scope to a specific cancer type or treatment phase. Specifically, it aims to explore and synthesize the roles and components of SDM in cancer treatment by examining how patients, family members (FMs), and HCPs participate in and collaborate on the decision-making process. By adopting a broader, more holistic perspective, the review seeks to address gaps in the existing literature and generate insights applicable across various cancer care contexts.
Materials and Methods
This scoping review was conducted using the Arksey and O’Malley framework, in accordance with the Joana Briggs Institute (JBI) (Aromataris & Munn, 2020). The process included (a) identifying the research questions; (b) identifying relevant articles; (c) selecting articles; (d) mapping data; and (e) collating, summarizing, and reporting results. Additionally, the PRISMA-ScR (preferred reporting items for systematic reviews and meta-analyses extension for scoping reviews) was used to optimize reporting and increase validity (Tricco et al., 2018). This research protocol has been registered in the Open Science Framework (OSF Ltd. 2026).
Identifying research questions
We aim to scope the existing literature and specifically answer the research question: how does the treatment decision-making process in cancer care integrate patient participation, family involvement, and HCPs’ roles?
Identifying relevant studies and search terms
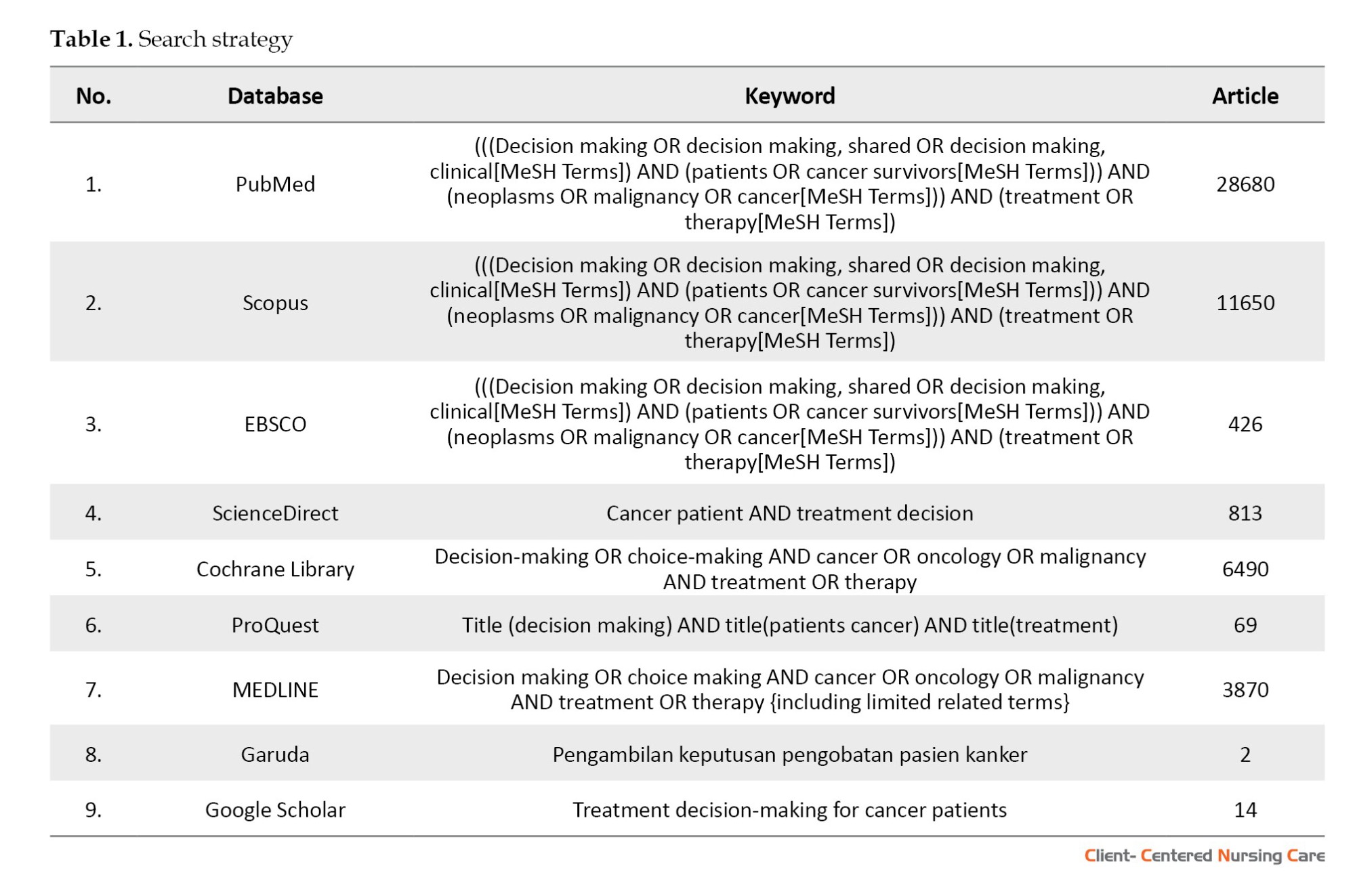
A comprehensive literature search was conducted across 8 prominent databases, including Scopus, PubMed, ProQuest, EBSCO, Cochrane Library, ScienceDirect, MEDLINE, and Garuda (an Indonesian database), as well as Google Scholar, a supplementary search engine. The search strategy employed MeSH terms and key phrases to identify relevant publications. The primary search terms included variations of "decision-making" or "choice-making," combined with cancer-related terms such as "neoplasms" or "malignancy," and treatment-related terms such as "therapy." For the Garuda database (Indonesian database), the search utilized the keyword "pengambilan keputusan pengobatan pasien kanker." These terms were applied to the title and abstract fields using appropriate Boolean operators (e.g. AND, OR) to combine concepts and improve the precision and sensitivity of the search. An initial exploratory search was performed to identify additional relevant keywords and their variations across different languages and cultural contexts. The identified terms were then incorporated into the main search strategy (Table 1). To ensure comprehensive coverage, the reference lists of articles retrieved from Google Scholar were also examined to identify potentially relevant studies that may have been overlooked in the database searches.
Selecting studies
All studies retrieved from the database searches were rigorously screened using predetermined inclusion and exclusion criteria. The initial phase involved reviewing the titles and abstracts of identified studies to assess their relevance, specifically regarding decision-making processes among adult cancer patients in clinical settings. To enhance the efficiency and accuracy of this screening process, Qatar Computing Research Institute (Rayyan QCRI) software was utilized (Ouzzani et al., 2016) and no single method fulfills the principal requirements of speed with accuracy. Automation of systematic reviews is driven by a necessity to expedite the availability of current best evidence for policy and clinical decision-making. We developed Rayyan (Rayyan, 2024). Two independent reviewers, a researcher and a nursing lecturer, conducted the selection process, resolving any conflicts through collaborative discussion to ensure consistency and accuracy in the final selection of studies.
The inclusion and exclusion criteria for this scoping review were established using the population concept context (PCC) model (Table 2).
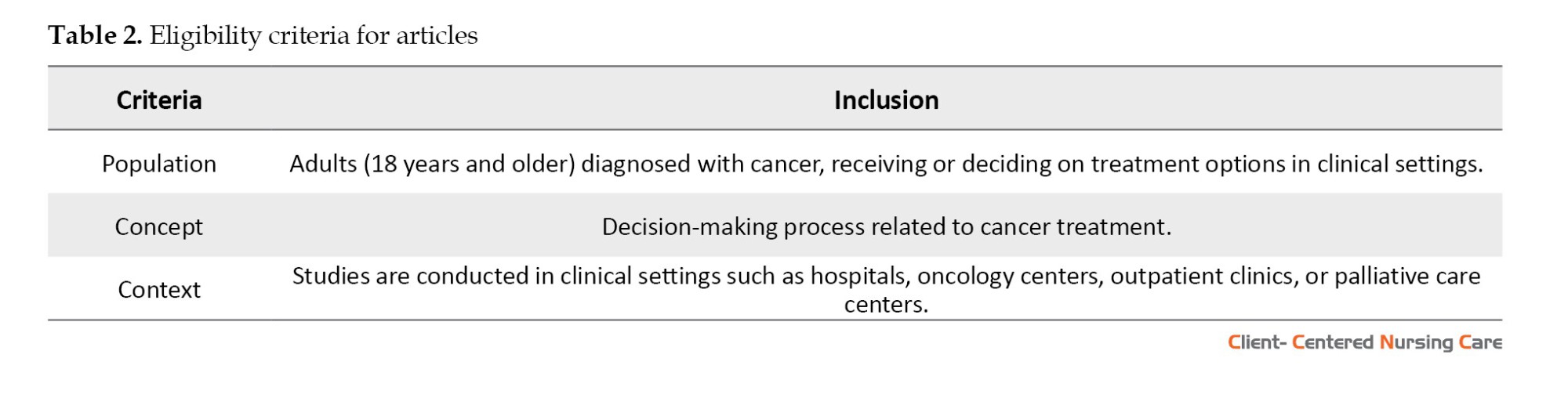
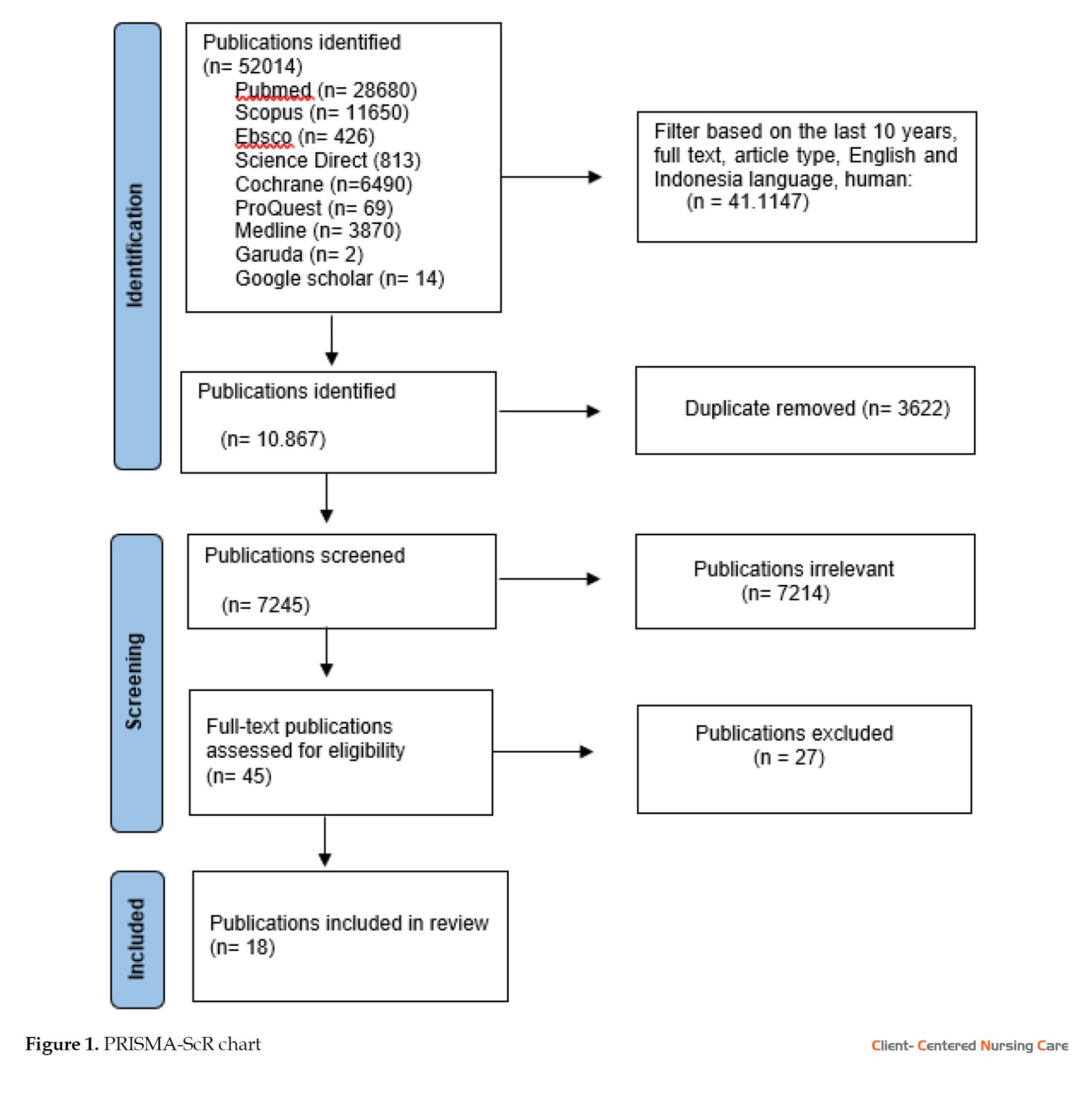
Qualitative, quantitative, and mixed-method studies presenting empirical data related to treatment decision-making were considered. However, opinions, editorials, commentaries, case reports, letters, literature studies (review studies), parts of books (book chapters), and articles originating from proceedings that do not provide full text, and single-patient studies without broader relevance to decision-making processes were excluded. Additionally, studies that focused solely on cancer prevention, early detection, or technical aspects of treatment, without addressing decision-making, were removed. Only studies published in English and Indonesian within the last 10 years were included, unless they were seminal works offering significant contributions to the field. Through a comprehensive search across eight databases and a supplementary search engine, 52014 relevant articles were initially collected in Mendeley reference manager. After removing duplicates and screening titles and abstracts, 31 publications were selected for full-text review. Ultimately, 18 articles were deemed relevant for data extraction and analysis (Figure 1).
Mapping data
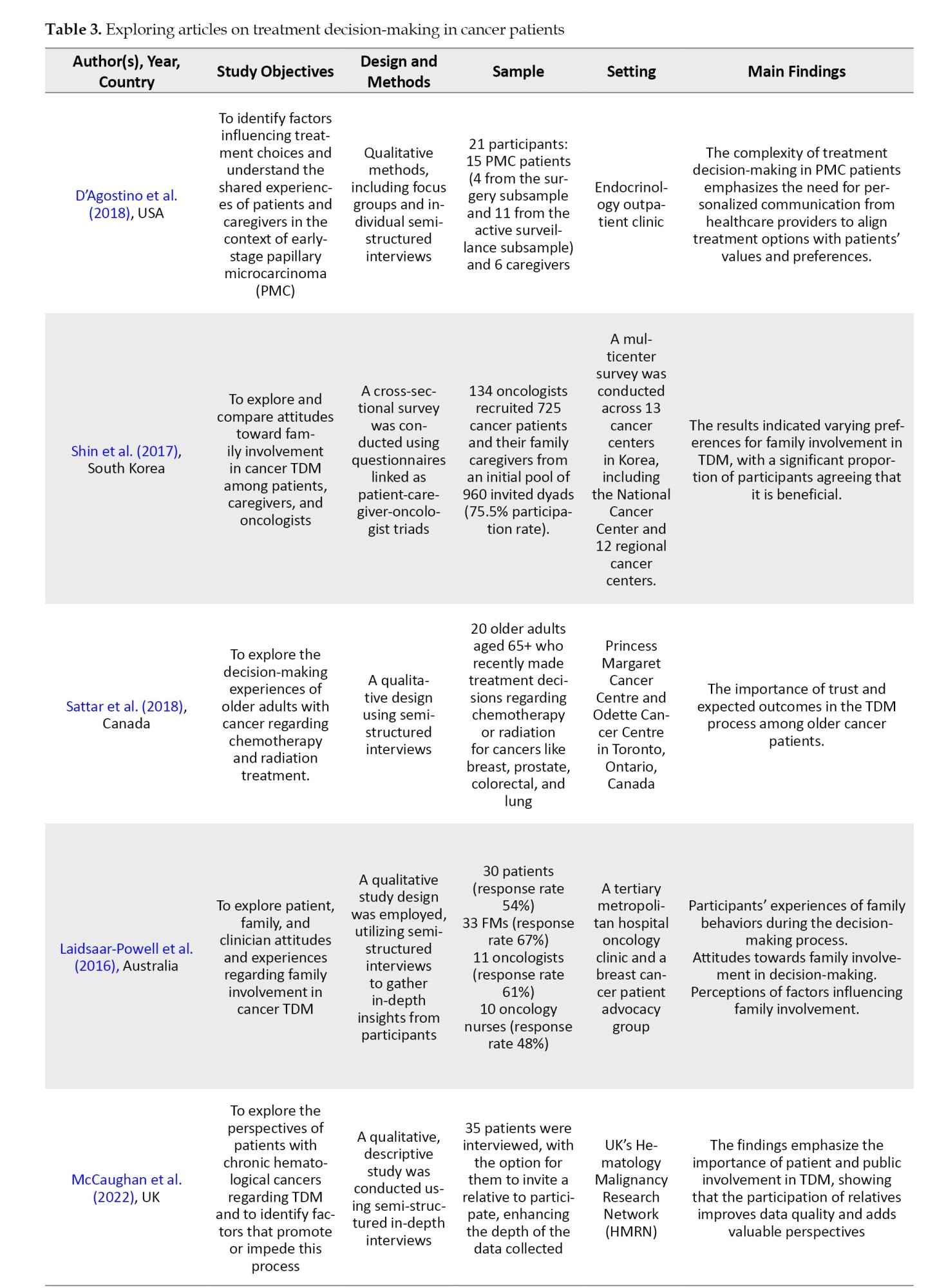
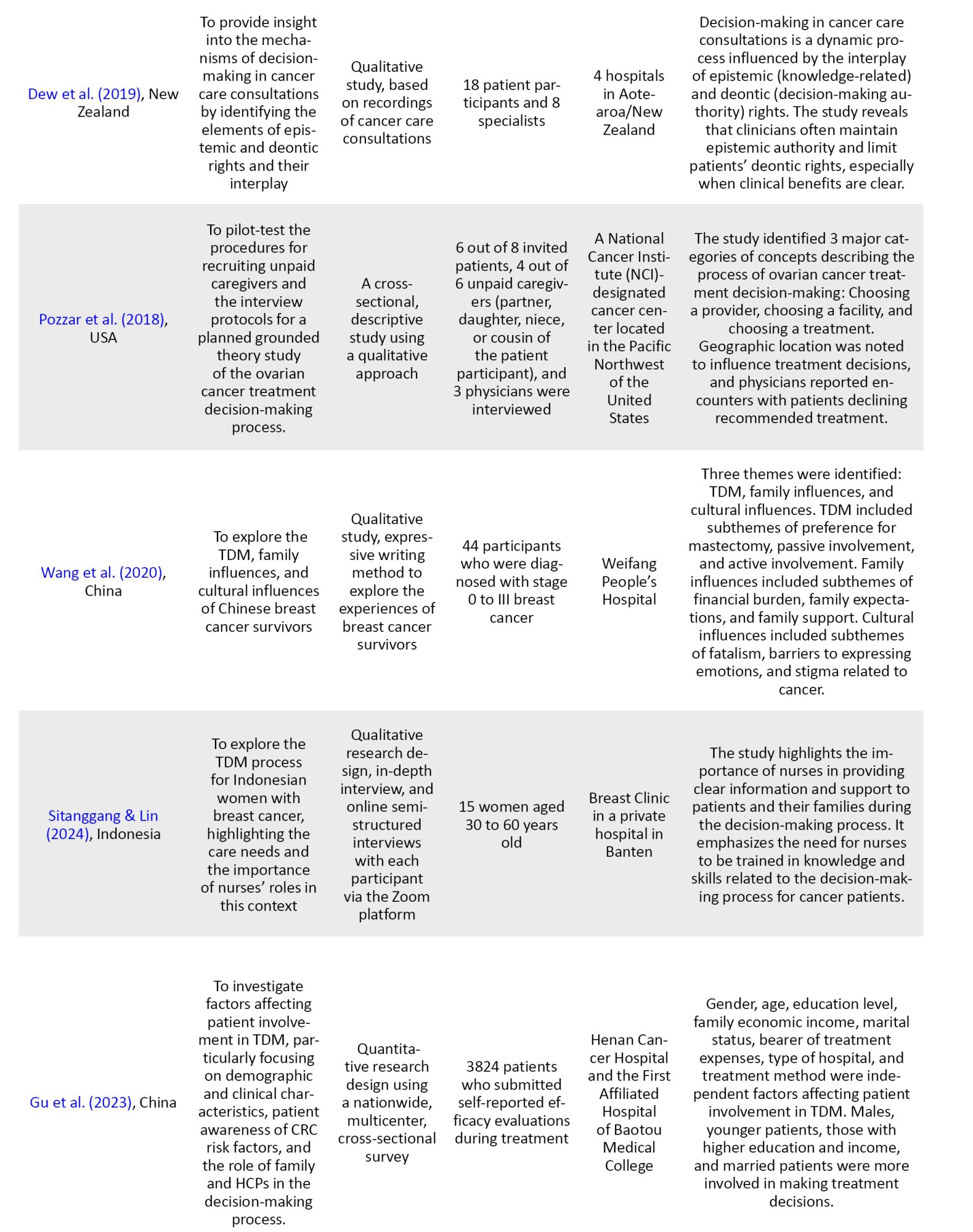
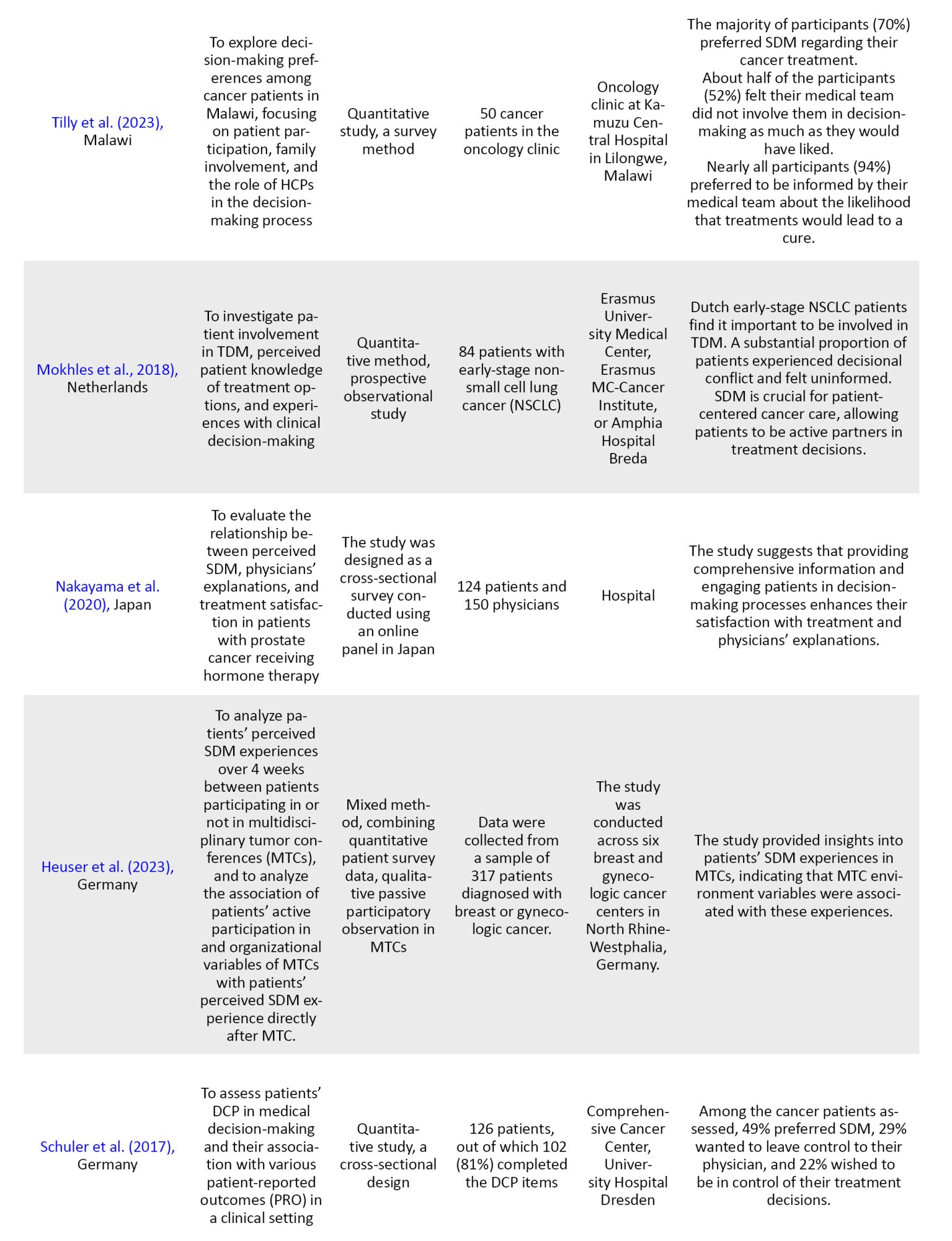
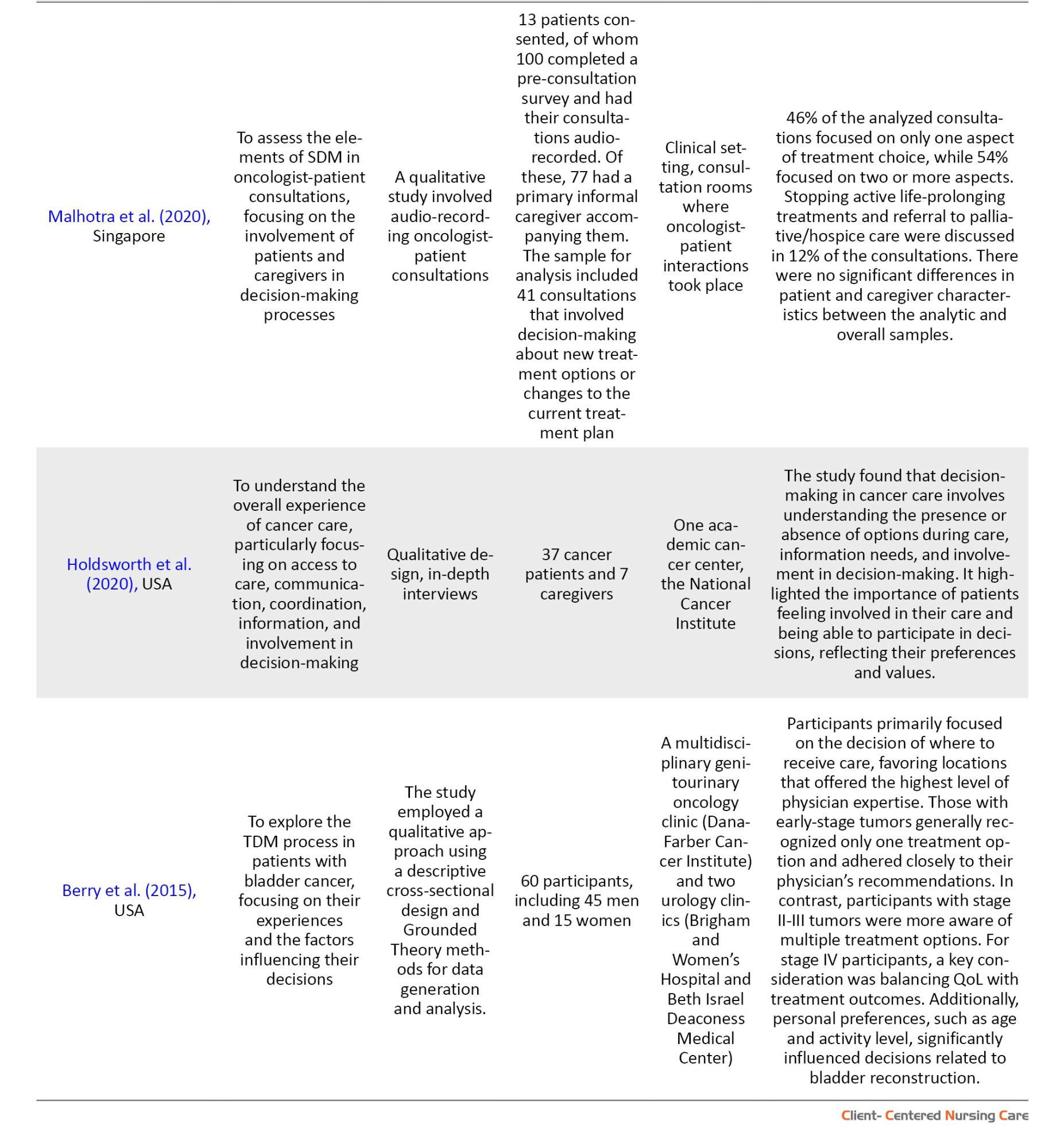
Data were systematically extracted by recording key information on authors, research purposes, study methods, participant characteristics, research context, and major findings. A detailed description of the analyzed variables is provided in Table 3.
Collating, summarizing, and reporting results
After delineating the research focus, SDM in cancer treatment within clinical settings, we systematically gathered data from pertinent articles examining patient participation, family involvement, and the roles of HCPs in this context. Statements and findings relevant to the study’s aims were then coded into predefined thematic categories, including patient engagement, family support, and HCP influence on treatment decision-making. Following the coding phase, the data were subjected to a thematic analysis to identify overarching patterns and insights related to these core themes. The results of this analysis were then organized into a structured, comprehensive report to offer an in-depth understanding of the levels and roles within SDM in cancer care, while addressing gaps identified in the existing literature.
Results
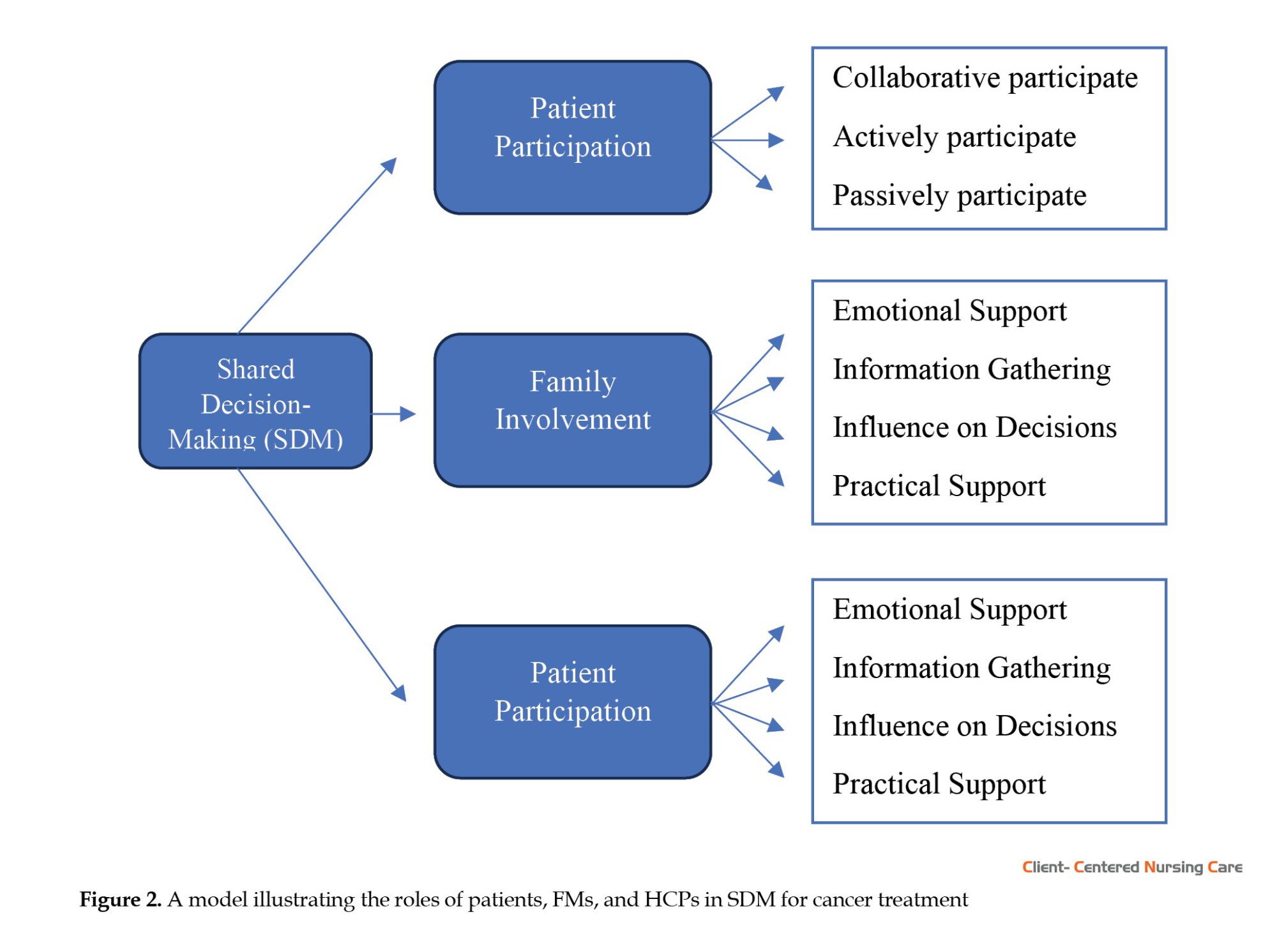
A total of 18 articles were deemed relevant for data extraction and analysis (Figure 1). Of 18 articles reviewed, 6 utilized quantitative research designs (Schuler et al., 2017; Shin et al., 2017; Mokhles et al., 2018; Nakayama et al., 2020; Gu et al., 2023; Tilly et al., 2023) family caregiver, and their treating oncologist view the risks and benefits of family involvement in cancer treatment decision making (TDM), 11 employed qualitative approaches (Berry et al., 2015; Laidsaar-Powell et al., 2016; D’Agostino et al., 2018; Pozzar et al., 2018; Sattar et al., 2018; Dew et al., 2019; Wang et al., 2020; Holdsworth et al., 2020; Malhotra et al., 2020; McCaughan et al., 2022; Sitanggang & Lin, 2024) and 1 used mixed methods designs (Heuser et al., 2023). The studies were conducted across various countries worldwide: 4 studies were from the United States (Berry et al., 2015; D’Agostino et al., 2018; Pozzar et al., 2018; Holdsworth et al., 2020), 2 each from Germany (Schuler et al., 2017; Heuser et al., 2023) and China (Wang et al., 2020; Gu et al., 2023), 1 study each from South Korea (Shin et al., 2017), Australia (Laidsaar-Powell et al., 2016), Netherlands (Mokhles et al., 2018), Japan (Nakayama et al., 2020), Singapore (Malhotra et al., 2020), Indonesia (Sitanggang & Lin, 2024), New Zealand (Dew et al., 2019), Canada (Sattar et al., 2018), Malawi (Tilly et al., 2023), UK (McCaughan et al., 2022). The results are organized into three interrelated components that shape SDM in cancer care: Patient participation, family involvement, and the role of HCPs. These components operate interactively across clinical and sociocultural contexts, rather than following a fixed sequential process. As illustrated in Figure 2, each stakeholder contributes distinct but complementary functions. Of the included studies, 100% (n=18) addressed elements of patient participation, 78% (n=14) addressed family involvement, and 89% (n=16) explored the role of HCPs.
Patient participation in decision-making
This review highlights the diverse ways in which patients participate in SDM, ranging from active, collaborative engagement to more passive roles. Studies across various cancer types indicate that SDM has increasingly become a primary approach in treatment-related decision-making. Across various countries, including the Netherlands, Japan, Germany, Malawi, Singapore, the UK, and Canada, patients demonstrated a strong preference for collaborative models, actively engaging in discussions alongside HCPs (Schuler et al., 2017; Mokhles et al., 2018; Sattar et al., 2018; Malhotra et al., 2020; Nakayama et al., 2020; McCaughan et al., 2022; Tilly et al., 2023) little is known on factors, which may influence cancer patients’ decision control preferences (DCP). Effective triadic communication and patient inclusion in multidisciplinary consultations were identified as enablers of significant SDM (Laidsaar-Powell et al., 2016; Heuser et al., 2023).
Active patient participation in cancer TDM often depends on the availability of adequate information and the patient’s confidence in evaluating the available treatment options. Evidence from multiple studies highlights variations in how patients engage in decision-making, reflecting individual preferences and contextual influences. Research conducted in South Korea has confirmed that patients tend to take an active role in treatment decisions (Shin et al., 2017). Similarly, early-stage papillary thyroid cancer patients were found to be more proactive in choosing surgical interventions, driven by concerns about disease progression (D’Agostino et al., 2018). Furthermore, personal preferences have been shown to significantly influence treatment choices among bladder cancer patients, affecting decisions about treatment locations and reconstruction options and reflecting high levels of patient engagement (Berry et al., 2015). However, variability in engagement patterns has also been observed, with some patients choosing active participation while others preferred to defer decisions to their HCPs (Holdsworth et al., 2020).
Conversely, passive participation is more common in specific cultural contexts, where social norms shape patients’ attitudes towards decision-making. For instance, in China and Indonesia, breast and colorectal cancer (CRC) patients often entrusted decisions to family or physicians, influenced by sociocultural norms and limited health literacy (Wang et al., 2020; Gu et al., 2023; Sitanggang & Lin, 2024). Even in Western countries, such as the United States, there are cases where ovarian cancer patients rely more on their physicians’ expertise to make urgent treatment decisions (Pozzar et al., 2018). Likewise, a study found that some patients favor a passive stance, placing full trust in their HCPs’ clinical knowledge (Dew et al., 2019).
Family involvement
Family involvement constitutes a foundational element in enhancing the quality of care and overall wellbeing of cancer patients. This scoping review identifies four primary dimensions of family engagement: Emotional support, information gathering, influence in decision-making, and practical support. Firstly, emotional support from FMs contributes significantly to the patient’s psychological resilience, as their presence, empathy, and moral support alleviate the anxiety and stress often associated with cancer treatment (Shin et al., 2017; Sattar et al., 2018; Nakayama et al., 2020) family caregiver, and their treating oncologist view the risks and benefits of family involvement in cancer TDM. Secondly, families frequently serve as advocates, proactively seeking information on diagnoses, treatment options, and care plans, thereby facilitating more informed and meaningful decision-making by the patient (Berry et al., 2015; McCaughan et al., 2022). Moreover, FMs play a critical role in influencing treatment decisions, especially when patients experience cognitive or physical limitations, thereby ensuring that chosen interventions align with the patient’s values and preferences, which ultimately enhances the appropriateness of clinical care (Dew et al., 2019; Malhotra et al., 2020; Wang et al., 2020). Finally, practical support, ranging from assistance with mobility and daily living tasks to medication management, plays a pivotal role in alleviating patients’ burdens, thereby enabling them to focus on recovery (Berry et al., 2015; Dew et al., 2019; Sitanggang & Lin, 2024). In summary, these aspects underscore the integral and multidimensional role of family involvement in supporting patients through the complexities of cancer treatment.
HCPs’ roles
HCPs play a pivotal role in supporting cancer patients and their families by serving as primary sources of information, facilitators of decision-making, providers of emotional support, and experts in clinical care. To begin with, HCPs serve as crucial information providers, ensuring that patients and families receive clear and comprehensive explanations regarding diagnoses, treatment options, and care plans (Berry et al., 2015; Laidsaar-Powell et al., 2016; Shin et al., 2017; Schuler et al., 2017; D’Agostino et al., 2018; Pozzar et al., 2018; Sattar et al., 2018; Dew et al., 2019; Wang et al., 2020; Malhotra et al., 2020; Nakayama et al., 2020; McCaughan et al., 2022; Sitanggang and Lin, 2024). As noted by several studies, effective communication from HCPs encourages patient and family engagement and promotes active participation in the care process (Schuler et al., 2017; Malhotra et al., 2020; Nakayama et al., 2020). In addition to this role, HCPs facilitate decision-making by guiding patients and families through complex choices, thereby reducing ambiguity and fostering confidence in treatment pathways (Heuser et al., 2023; Tilly et al., 2023). A further role is the provision of emotional support, in which HCPs contribute to a calm, empathetic environment that helps reduce anxiety and enhance emotional resilience among patients (Laidsaar-Powell et al., 2016; Sattar et al., 2018; Wang et al., 2020). Finally, the clinical expertise of HCPs is essential to delivering safe, evidence-based, and high-quality care. This expertise allows HCPs to accurately diagnose, assess, and implement clinical interventions aligned with current best practices, contributing to optimal care outcomes (Pozzar et al., 2018; Dew et al., 2019; McCaughan et al., 2022). Taken together, these roles underscore the integral role of HCPs in holistic patient and family wellbeing in cancer care.
Discussion
Based on the findings of this review (Table 4), there are three main themes regarding SDM levels in cancer treatment in clinical settings: Patient participation, family involvement, and the role of HCPs.
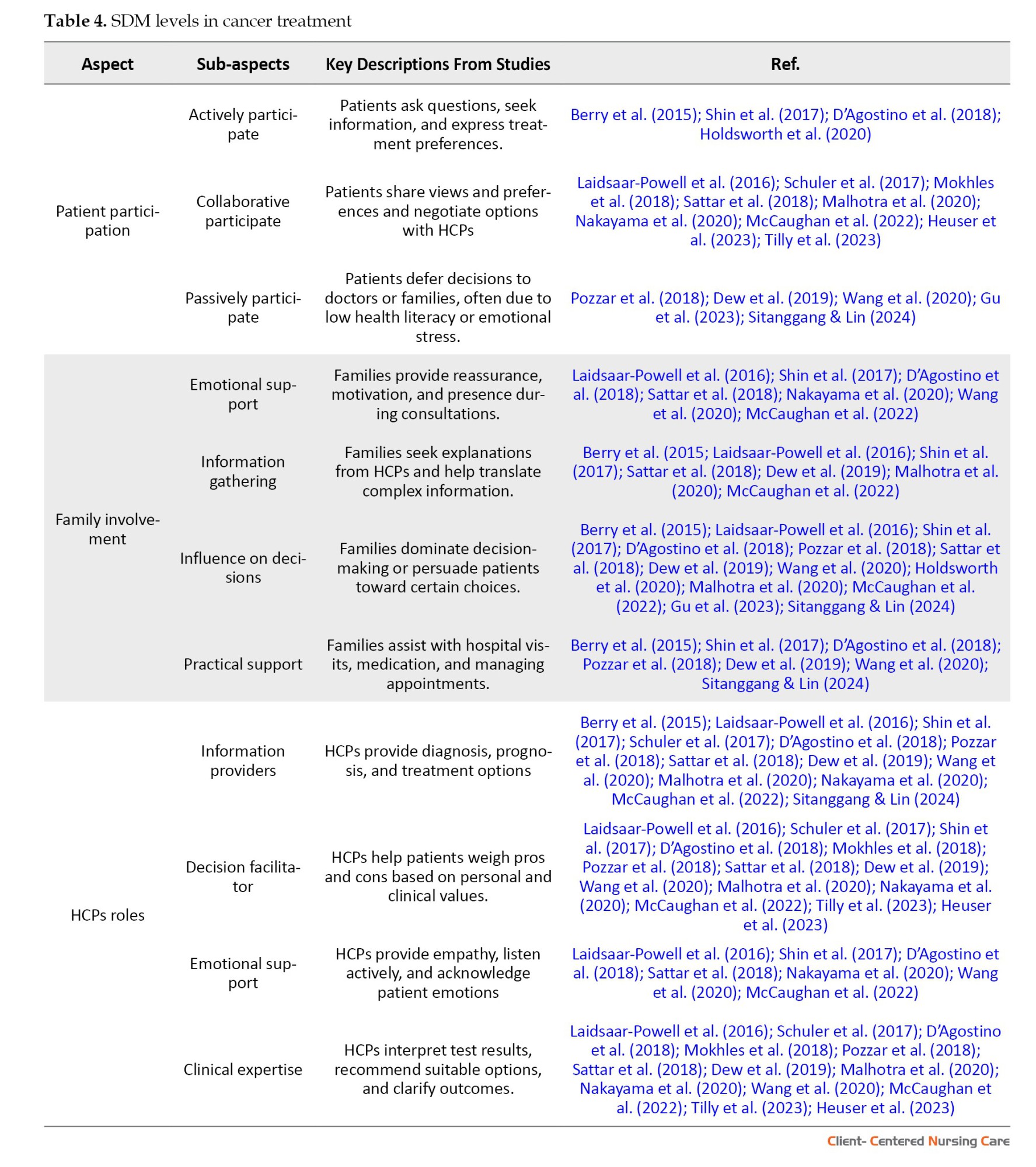
Patient participation in decision-making
Patient involvement in decision-making is a fundamental component of effective SDM, reflecting a broader shift toward patient-centered care. Evidence from the literature indicates a strong trend toward adopting collaborative, or SDM approaches in various clinical settings (Laidsaar-Powell et al., 2016; Schuler et al., 2017; Mokhles et al., 2018; Sattar et al., 2018; Malhotra et al., 2020; Nakayama et al., 2020; McCaughan et al., 2022; Heuser et al., 2023; Tilly et al., 2023). SDM has emerged as a well-established strategy in healthcare settings, designed to involve patients actively in decision-making. This approach is instrumental in enhancing patient autonomy and promoting a more patient-centered model of care (Barry & Edgman-Levitan, 2012; Stiggelbout et al., 2012). In oncology, SDM is particularly crucial, fostering collaborative communication between patients and healthcare providers, which is essential for optimizing treatment outcomes and patient satisfaction in complex therapeutic decisions (Shickh et al., 2023).
Despite its recognized benefits, SDM implementation is not uniform across settings, with variations influenced by patient demographics, such as age, education level, and cultural background. Research indicates that younger, more educated patients are more likely to actively engage in treatment decisions, while older patients often prefer a more passive role, relying predominantly on medical guidance (Gieseler et al., 2019; Pyke-Grimm et al., 2020). Factors such as health literacy, decision-making dynamics, and the intricacies of cancer treatment modalities play a significant role in shaping these engagement patterns (Chang et al., 2019; Gieseler et al., 2019). In many cultural contexts, particularly in Asian countries, prevailing social norms often lead patients to defer decision-making responsibilities to FMs or HCPs (Wang et al., 2020; Sitanggang & Lin, 2024). These considerations highlight the need for a more nuanced approach that respects diverse cultural norms while upholding patient autonomy in the SDM process.
The movement towards SDM in clinical practice represents a significant advancement in modern healthcare, particularly in oncology, where treatment adherence and clinical outcomes are closely linked to patient engagement. Engaging patients in therapeutic decision-making enhances the personalization of care, enabling healthcare providers to more effectively respond to individual patient needs and preferences. However, many patients remain reliant on professional expertise, and a growing inclination toward active participation underscores the need for a balanced approach that integrates patient autonomy with professional guidance in cancer care.
Given the complexity of implementing SDM, there are considerable implications for practice, policy, and research. Clinically, HCPs must adopt communication frameworks that support SDM, incorporating decision aids and culturally tailored resources to meet local and individual needs. Health education programs would benefit from incorporating SDM-focused training, with emphasis on cross-cultural sensitivity and ethical decision-making. At the policy level, healthcare systems should advocate for patient-centered policies that incentivize SDM practices, alongside supporting the development of digital and informational infrastructures that facilitate informed decision-making. Future research should aim to validate SDM models that address cultural variability and assess their impact on long-term outcomes and patient satisfaction. This multifaceted approach holds significant promise for improving the quality of patient care, satisfaction, and health outcomes, particularly in diverse patient populations and complex care settings.
Family involvement
The findings of this review highlight the crucial role of family involvement in SDM in cancer treatment, where families often provide emotional, informational, decisional, and practical support to patients. Studies consistently show that FMs act as key advocates, helping patients navigate complex medical information and making more informed treatment decisions (Shin et al., 2017; Malhotra et al., 2020; McCaughan et al., 2022). This active involvement of families can significantly influence the patient's treatment pathway by offering a support system that reduces anxiety and enhances the patient's confidence in their choices (Shin et al., 2017; Sattar et al., 2018).
Family involvement in medical decision-making aligns with the principles of patient-centered care, which emphasize collaborative relationships between patients, families, and healthcare providers. According to the theory of relational autonomy, patients’ decisions are not made in isolation but are influenced by their relationships and the social context in which they live. This concept supports the idea that FMs' roles in decision-making contribute to a shared understanding of the patient's values and treatment goals, thus enhancing the decision-making process (Elwyn et al., 2012).
In cancer treatment decisions, families serve both as supporters and influential participants. Prior research indicates that families often assume primary or SDM roles, which substantially affects treatment choices and outcomes. For instance, a national survey by Dionne-Odom et al. found that 87.6% of family caregivers engaged in treatment decisions, with 53.9% sharing decision-making responsibilities (Dionne-Odom et al., 2023). This significant role is especially prominent among adult children of older patients, who frequently facilitate SDM, leading to more informed treatment choices (Dijkman et al., 2022). However, it is essential to maintain a balance between family involvement and patient autonomy (Hobbs et al., 2015). This family role highlights the need for clear and open communication among all parties involved, ensuring that patient autonomy is upheld while valuing family contributions
Although family involvement generally enhances the SDM process by providing emotional, informational, and practical support, it is essential to maintain a patient-centered approach in which the individual's preferences and values remain central. While families often serve as advocates and sources of strength, their influence should not override the patient's autonomy, especially in decisions with significant personal implications. HCPs play a crucial mediating role in balancing these dynamics by facilitating open dialogue that respects both the patient’s choices and the family’s perspectives, aiming to reach a consensus aligned with the patient’s best interests.
The insights from this review highlight the need for healthcare systems to adopt a more structured and culturally responsive framework for incorporating family involvement into SDM. It includes equipping HCPs with communication competencies that are sensitive to diverse familial roles and expectations, particularly in collectivist cultures where family input is traditionally more dominant. Additionally, integrating guidelines and decision-support tools that explicitly address family dynamics could improve the quality and transparency of the decision-making process. Prioritizing family engagement in SDM not only promotes holistic, person-centered care but also strengthens the therapeutic alliance between patients, families, and clinicians—ultimately contributing to better treatment experiences and outcomes.
Role of HCPs
The findings of this review suggest that HCPs play multifaceted roles in SDM. Across the included studies, HCPs were consistently involved as providers of clinical information, facilitators of decision-making, sources of emotional support, and contributors of clinical expertise throughout the treatment process. These roles are essential in helping patients navigate the complexities of cancer care, ultimately enhancing their confidence and satisfaction with the chosen treatment pathway.
These roles align closely with the principles of SDM, which advocate for collaborative communication between patients and healthcare providers. Effective communication emerged as a fundamental element, enabling patients to fully comprehend their diagnoses and treatment options, thereby supporting informed, value-based decision-making (Kehl et al., 2015; Dew et al., 2019; Heuser et al., 2023). High levels of trust in HCPs also shape how patients engage, especially in complex or urgent care (Hariati et al., 2021). HCP engagement significantly influences the implementation of patient- and family-centered care (Hariati et al., 2023). This approach also reflects the core of patient-centered care, where patients’ preferences, goals, and values are integrated into clinical decision-making (Elwyn et al., 2012).
Previous studies support these findings, emphasizing the importance of HCP communication skills in improving clinical outcomes. For instance, studies have shown that patients who perceive their healthcare providers as effective communicators report lower anxiety levels and greater satisfaction with their care (Faller et al., 2016). Additionally, studies have identified barriers to implementing SDM, including time constraints and limited formal training in communication and decision-making techniques (Légaré et al., 2008). These challenges have been further explored in recent research, particularly within the context of the UK’s National Health Service, highlighting the need for ongoing initiatives to equip HCPs with the skills necessary to engage patients effectively in treatment decisions (Joseph-Williams et al., 2017), which examined the implementation of SDM in the UK's National Health Service. Similarly, a qualitative study in Indonesia found that nurses face challenges in education due to the absence of standardized policies, limited training, and a lack of educational resources (Hariati et al., 2022). Also, a qualitative study in Indonesia highlights the challenges nurses face in providing effective discharge education due to the absence of standardized guidelines and limited training (Hariati et al., 2021). These studies collectively indicate the need for ongoing efforts to equip HCPs with the skills to engage patients in their treatment decisions effectively.
In this context, structured orientation and training programs have proven effective in improving HCPs' clinical readiness and interpersonal skills. A recent scoping review emphasizes that well-designed onboarding initiatives for nurses significantly strengthen their confidence, communication skills, and role adaptation within hospital settings (Ernawaty et al., 2024). These findings support the implementation of structured training programs to prepare nurses for such interventions. As shown by Erfina et al. (2024), nurse-delivered multimodal interventions not only address physical and psychological symptoms but also enhance the therapeutic alliance between patients and providers, an essential component of effective SDM. This finding highlights the importance of equipping nurses with both clinical and communication competencies to deliver meaningful, patient-centered cancer care.
Therefore, a more structured approach is needed to strengthen HCPs' role as facilitators in patient treatment decision-making. Although HCPs are strategically positioned to guide patients in choosing treatment options, their effectiveness is often hindered by systemic barriers such as a lack of training in SDM practices and time constraints within clinical settings. Addressing these obstacles can significantly enhance patient engagement, resulting in more personalized and satisfying healthcare experiences.
The findings of this review underscore the importance of healthcare systems prioritizing the development of training programs to improve HCPs' communication and decision-making skills. By integrating SDM principles into medical education and clinical practice, healthcare providers can bridge the gap between professional recommendations and patient preferences. Additionally, the use of digital decision aids and culturally sensitive communication strategies can promote a more inclusive and patient-centered approach across diverse healthcare settings.
These findings present several implications for clinical practice. First, adopting a more holistic approach to patient care that integrates the perspectives of patients, families, and HCPs can enhance the SDM process. Implementing SDM tools that accommodate cultural nuances can improve patient engagement, particularly among diverse patient populations. Additionally, equipping HCPs with training in cultural sensitivity and communication skills will foster more effective and empathetic interactions with patients and their families.
While this scoping review provides a comprehensive overview, certain limitations should be acknowledged. The review was limited to articles published in English and Indonesian, potentially excluding relevant studies in other languages. Moreover, most of the included studies were conducted in high-income countries, which may not fully represent the experiences of patients in low- and middle-income settings.
Future research should examine the SDM process across diverse cultural contexts and healthcare systems to provide a broader perspective. Additionally, longitudinal studies examining how interactions among patients, families, and HCPs evolve could offer deeper insights into optimizing SDM in cancer care.
Conclusion
This scoping review examined the roles of patients, families, and HCPs in the SDM process for cancer patients in clinical settings. Three primary factors emerged: Patient participation, family involvement, and support from HCPs. Active patient engagement and family involvement were shown to enhance patient confidence and satisfaction, while HCPs played critical roles as information providers and decision facilitators. Balancing patient autonomy with family input was highlighted as essential, facilitated through effective communication by HCPs. Structured frameworks and culturally sensitive training for HCPs are recommended to improve SDM, ensuring decisions are both patient-centered and value-aligned across diverse healthcare settings. These findings present several implications for clinical practice. First, adopting a more holistic approach to patient care that integrates the perspectives of patients, families, and HCPs can enhance the SDM process. Implementing SDM tools that accommodate cultural nuances can improve patient engagement, particularly among diverse patient populations. Additionally, equipping HCPs with training in cultural sensitivity and communication skills will foster more effective and empathetic interactions with patients and their families.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization: Fadiah Izzati Salim and Suni Hariati;Methodology: Fadiah Izzati Salim and Andi Masyitha Irwan; Investigation and data curation: Fadiah Izzati Salim and Andi Masyitha Irwan; Data analysis, validation and visualization: Suni Hariati and Erfina Erfina; Writing the original draft: Fadiah Izzati Salim, Suni Hariati, and Andi Masyitha Irwan; Review, editing and final approval: All authors; Supervision: Suni Hariati.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank Kusrini Kadar, for her proofreading of this article.
References
Cancer is a critical global health challenge among non-communicable diseases, characterized by uncontrolled cellular proliferation that may invade surrounding tissues and metastasize (Magnusson, 2020; American Cancer Society, 2024). The incidence of new cancer cases worldwide rose from 18.1 million in 2018 to 19.3 million in 2020, resulting in nearly 10 million deaths across all age groups, and projections indicate an increase of 61.3% by 2040 (WHO, 2022). Given the high and escalating prevalence of cancer, making informed treatment decisions is imperative. A cancer diagnosis profoundly affects patients and their families, impacting not only physical health but also emotional, social, and financial wellbeing (Khullar et al., 2018). Patients must navigate numerous uncertainties related to diagnostic procedures, complex treatment regimens, remission, palliative care, and unpredictable disease outcomes, a process that can recur throughout their lives (Stone & Olsen, 2022). These challenges significantly influence the patient's quality of life (QoL) and can lead to heightened levels of stress, anxiety, and depression (Pitman et al., 2018). Therefore, the decision-making process surrounding treatment options is a vital component of the patient's journey through illness.
The decision-making process in healthcare involves a collaborative effort among the patient, their family, and the medical team to identify treatment options that align with the patient's preferences and needs, based on available information (Tariman et al., 2012). An increasing recognition of its significance drives this shift towards a more patient-centered approach (Zucca et al., 2014). Engaging patients more actively in clinical decision-making can enable healthcare providers to accept choices that may not align with their professional judgments but that the patient is willing to pursue (Légaré & Witteman, 2013). Consequently, adopting effective decision-making models in clinical settings could be a beneficial strategy for helping cancer patients evaluate their treatment options.
Previous reviews of decision-making in cancer care have typically focused on specific aspects of the process, such as particular age groups or healthcare providers. For instance, Dijkman et al. (2022) examined treatment preferences among older adults, and Spronk et al. (2018) investigated the availability and effectiveness of shared decision-making (SDM) tools. However, this study was limited to metastatic breast cancer patients. Neither review addressed cancer patients more broadly. Meanwhile, Pinker and Pilleron (2023) focused on the role of healthcare providers in patient decision-making. Similarly, Covvey et al. (2019) explored the barriers and facilitators of SDM in oncology, identifying factors such as patient characteristics, physician roles, and health system influences. However, a comprehensive review that integrates the involvement of patients, families, and healthcare professionals (HCPs) in the SDM process has not yet been conducted.
In contrast to previous studies, this scoping review focuses on cancer patients in general, across diverse clinical settings, rather than limiting its scope to a specific cancer type or treatment phase. Specifically, it aims to explore and synthesize the roles and components of SDM in cancer treatment by examining how patients, family members (FMs), and HCPs participate in and collaborate on the decision-making process. By adopting a broader, more holistic perspective, the review seeks to address gaps in the existing literature and generate insights applicable across various cancer care contexts.
Materials and Methods
This scoping review was conducted using the Arksey and O’Malley framework, in accordance with the Joana Briggs Institute (JBI) (Aromataris & Munn, 2020). The process included (a) identifying the research questions; (b) identifying relevant articles; (c) selecting articles; (d) mapping data; and (e) collating, summarizing, and reporting results. Additionally, the PRISMA-ScR (preferred reporting items for systematic reviews and meta-analyses extension for scoping reviews) was used to optimize reporting and increase validity (Tricco et al., 2018). This research protocol has been registered in the Open Science Framework (OSF Ltd. 2026).
Identifying research questions
We aim to scope the existing literature and specifically answer the research question: how does the treatment decision-making process in cancer care integrate patient participation, family involvement, and HCPs’ roles?
Identifying relevant studies and search terms
A comprehensive literature search was conducted across 8 prominent databases, including Scopus, PubMed, ProQuest, EBSCO, Cochrane Library, ScienceDirect, MEDLINE, and Garuda (an Indonesian database), as well as Google Scholar, a supplementary search engine. The search strategy employed MeSH terms and key phrases to identify relevant publications. The primary search terms included variations of "decision-making" or "choice-making," combined with cancer-related terms such as "neoplasms" or "malignancy," and treatment-related terms such as "therapy." For the Garuda database (Indonesian database), the search utilized the keyword "pengambilan keputusan pengobatan pasien kanker." These terms were applied to the title and abstract fields using appropriate Boolean operators (e.g. AND, OR) to combine concepts and improve the precision and sensitivity of the search. An initial exploratory search was performed to identify additional relevant keywords and their variations across different languages and cultural contexts. The identified terms were then incorporated into the main search strategy (Table 1). To ensure comprehensive coverage, the reference lists of articles retrieved from Google Scholar were also examined to identify potentially relevant studies that may have been overlooked in the database searches.
Selecting studies
All studies retrieved from the database searches were rigorously screened using predetermined inclusion and exclusion criteria. The initial phase involved reviewing the titles and abstracts of identified studies to assess their relevance, specifically regarding decision-making processes among adult cancer patients in clinical settings. To enhance the efficiency and accuracy of this screening process, Qatar Computing Research Institute (Rayyan QCRI) software was utilized (Ouzzani et al., 2016) and no single method fulfills the principal requirements of speed with accuracy. Automation of systematic reviews is driven by a necessity to expedite the availability of current best evidence for policy and clinical decision-making. We developed Rayyan (Rayyan, 2024). Two independent reviewers, a researcher and a nursing lecturer, conducted the selection process, resolving any conflicts through collaborative discussion to ensure consistency and accuracy in the final selection of studies.
The inclusion and exclusion criteria for this scoping review were established using the population concept context (PCC) model (Table 2).
Qualitative, quantitative, and mixed-method studies presenting empirical data related to treatment decision-making were considered. However, opinions, editorials, commentaries, case reports, letters, literature studies (review studies), parts of books (book chapters), and articles originating from proceedings that do not provide full text, and single-patient studies without broader relevance to decision-making processes were excluded. Additionally, studies that focused solely on cancer prevention, early detection, or technical aspects of treatment, without addressing decision-making, were removed. Only studies published in English and Indonesian within the last 10 years were included, unless they were seminal works offering significant contributions to the field. Through a comprehensive search across eight databases and a supplementary search engine, 52014 relevant articles were initially collected in Mendeley reference manager. After removing duplicates and screening titles and abstracts, 31 publications were selected for full-text review. Ultimately, 18 articles were deemed relevant for data extraction and analysis (Figure 1).
Mapping data
Data were systematically extracted by recording key information on authors, research purposes, study methods, participant characteristics, research context, and major findings. A detailed description of the analyzed variables is provided in Table 3.
Collating, summarizing, and reporting results
After delineating the research focus, SDM in cancer treatment within clinical settings, we systematically gathered data from pertinent articles examining patient participation, family involvement, and the roles of HCPs in this context. Statements and findings relevant to the study’s aims were then coded into predefined thematic categories, including patient engagement, family support, and HCP influence on treatment decision-making. Following the coding phase, the data were subjected to a thematic analysis to identify overarching patterns and insights related to these core themes. The results of this analysis were then organized into a structured, comprehensive report to offer an in-depth understanding of the levels and roles within SDM in cancer care, while addressing gaps identified in the existing literature.
Results
A total of 18 articles were deemed relevant for data extraction and analysis (Figure 1). Of 18 articles reviewed, 6 utilized quantitative research designs (Schuler et al., 2017; Shin et al., 2017; Mokhles et al., 2018; Nakayama et al., 2020; Gu et al., 2023; Tilly et al., 2023) family caregiver, and their treating oncologist view the risks and benefits of family involvement in cancer treatment decision making (TDM), 11 employed qualitative approaches (Berry et al., 2015; Laidsaar-Powell et al., 2016; D’Agostino et al., 2018; Pozzar et al., 2018; Sattar et al., 2018; Dew et al., 2019; Wang et al., 2020; Holdsworth et al., 2020; Malhotra et al., 2020; McCaughan et al., 2022; Sitanggang & Lin, 2024) and 1 used mixed methods designs (Heuser et al., 2023). The studies were conducted across various countries worldwide: 4 studies were from the United States (Berry et al., 2015; D’Agostino et al., 2018; Pozzar et al., 2018; Holdsworth et al., 2020), 2 each from Germany (Schuler et al., 2017; Heuser et al., 2023) and China (Wang et al., 2020; Gu et al., 2023), 1 study each from South Korea (Shin et al., 2017), Australia (Laidsaar-Powell et al., 2016), Netherlands (Mokhles et al., 2018), Japan (Nakayama et al., 2020), Singapore (Malhotra et al., 2020), Indonesia (Sitanggang & Lin, 2024), New Zealand (Dew et al., 2019), Canada (Sattar et al., 2018), Malawi (Tilly et al., 2023), UK (McCaughan et al., 2022). The results are organized into three interrelated components that shape SDM in cancer care: Patient participation, family involvement, and the role of HCPs. These components operate interactively across clinical and sociocultural contexts, rather than following a fixed sequential process. As illustrated in Figure 2, each stakeholder contributes distinct but complementary functions. Of the included studies, 100% (n=18) addressed elements of patient participation, 78% (n=14) addressed family involvement, and 89% (n=16) explored the role of HCPs.
Patient participation in decision-making
This review highlights the diverse ways in which patients participate in SDM, ranging from active, collaborative engagement to more passive roles. Studies across various cancer types indicate that SDM has increasingly become a primary approach in treatment-related decision-making. Across various countries, including the Netherlands, Japan, Germany, Malawi, Singapore, the UK, and Canada, patients demonstrated a strong preference for collaborative models, actively engaging in discussions alongside HCPs (Schuler et al., 2017; Mokhles et al., 2018; Sattar et al., 2018; Malhotra et al., 2020; Nakayama et al., 2020; McCaughan et al., 2022; Tilly et al., 2023) little is known on factors, which may influence cancer patients’ decision control preferences (DCP). Effective triadic communication and patient inclusion in multidisciplinary consultations were identified as enablers of significant SDM (Laidsaar-Powell et al., 2016; Heuser et al., 2023).
Active patient participation in cancer TDM often depends on the availability of adequate information and the patient’s confidence in evaluating the available treatment options. Evidence from multiple studies highlights variations in how patients engage in decision-making, reflecting individual preferences and contextual influences. Research conducted in South Korea has confirmed that patients tend to take an active role in treatment decisions (Shin et al., 2017). Similarly, early-stage papillary thyroid cancer patients were found to be more proactive in choosing surgical interventions, driven by concerns about disease progression (D’Agostino et al., 2018). Furthermore, personal preferences have been shown to significantly influence treatment choices among bladder cancer patients, affecting decisions about treatment locations and reconstruction options and reflecting high levels of patient engagement (Berry et al., 2015). However, variability in engagement patterns has also been observed, with some patients choosing active participation while others preferred to defer decisions to their HCPs (Holdsworth et al., 2020).
Conversely, passive participation is more common in specific cultural contexts, where social norms shape patients’ attitudes towards decision-making. For instance, in China and Indonesia, breast and colorectal cancer (CRC) patients often entrusted decisions to family or physicians, influenced by sociocultural norms and limited health literacy (Wang et al., 2020; Gu et al., 2023; Sitanggang & Lin, 2024). Even in Western countries, such as the United States, there are cases where ovarian cancer patients rely more on their physicians’ expertise to make urgent treatment decisions (Pozzar et al., 2018). Likewise, a study found that some patients favor a passive stance, placing full trust in their HCPs’ clinical knowledge (Dew et al., 2019).
Family involvement
Family involvement constitutes a foundational element in enhancing the quality of care and overall wellbeing of cancer patients. This scoping review identifies four primary dimensions of family engagement: Emotional support, information gathering, influence in decision-making, and practical support. Firstly, emotional support from FMs contributes significantly to the patient’s psychological resilience, as their presence, empathy, and moral support alleviate the anxiety and stress often associated with cancer treatment (Shin et al., 2017; Sattar et al., 2018; Nakayama et al., 2020) family caregiver, and their treating oncologist view the risks and benefits of family involvement in cancer TDM. Secondly, families frequently serve as advocates, proactively seeking information on diagnoses, treatment options, and care plans, thereby facilitating more informed and meaningful decision-making by the patient (Berry et al., 2015; McCaughan et al., 2022). Moreover, FMs play a critical role in influencing treatment decisions, especially when patients experience cognitive or physical limitations, thereby ensuring that chosen interventions align with the patient’s values and preferences, which ultimately enhances the appropriateness of clinical care (Dew et al., 2019; Malhotra et al., 2020; Wang et al., 2020). Finally, practical support, ranging from assistance with mobility and daily living tasks to medication management, plays a pivotal role in alleviating patients’ burdens, thereby enabling them to focus on recovery (Berry et al., 2015; Dew et al., 2019; Sitanggang & Lin, 2024). In summary, these aspects underscore the integral and multidimensional role of family involvement in supporting patients through the complexities of cancer treatment.
HCPs’ roles
HCPs play a pivotal role in supporting cancer patients and their families by serving as primary sources of information, facilitators of decision-making, providers of emotional support, and experts in clinical care. To begin with, HCPs serve as crucial information providers, ensuring that patients and families receive clear and comprehensive explanations regarding diagnoses, treatment options, and care plans (Berry et al., 2015; Laidsaar-Powell et al., 2016; Shin et al., 2017; Schuler et al., 2017; D’Agostino et al., 2018; Pozzar et al., 2018; Sattar et al., 2018; Dew et al., 2019; Wang et al., 2020; Malhotra et al., 2020; Nakayama et al., 2020; McCaughan et al., 2022; Sitanggang and Lin, 2024). As noted by several studies, effective communication from HCPs encourages patient and family engagement and promotes active participation in the care process (Schuler et al., 2017; Malhotra et al., 2020; Nakayama et al., 2020). In addition to this role, HCPs facilitate decision-making by guiding patients and families through complex choices, thereby reducing ambiguity and fostering confidence in treatment pathways (Heuser et al., 2023; Tilly et al., 2023). A further role is the provision of emotional support, in which HCPs contribute to a calm, empathetic environment that helps reduce anxiety and enhance emotional resilience among patients (Laidsaar-Powell et al., 2016; Sattar et al., 2018; Wang et al., 2020). Finally, the clinical expertise of HCPs is essential to delivering safe, evidence-based, and high-quality care. This expertise allows HCPs to accurately diagnose, assess, and implement clinical interventions aligned with current best practices, contributing to optimal care outcomes (Pozzar et al., 2018; Dew et al., 2019; McCaughan et al., 2022). Taken together, these roles underscore the integral role of HCPs in holistic patient and family wellbeing in cancer care.
Discussion
Based on the findings of this review (Table 4), there are three main themes regarding SDM levels in cancer treatment in clinical settings: Patient participation, family involvement, and the role of HCPs.
Patient participation in decision-making
Patient involvement in decision-making is a fundamental component of effective SDM, reflecting a broader shift toward patient-centered care. Evidence from the literature indicates a strong trend toward adopting collaborative, or SDM approaches in various clinical settings (Laidsaar-Powell et al., 2016; Schuler et al., 2017; Mokhles et al., 2018; Sattar et al., 2018; Malhotra et al., 2020; Nakayama et al., 2020; McCaughan et al., 2022; Heuser et al., 2023; Tilly et al., 2023). SDM has emerged as a well-established strategy in healthcare settings, designed to involve patients actively in decision-making. This approach is instrumental in enhancing patient autonomy and promoting a more patient-centered model of care (Barry & Edgman-Levitan, 2012; Stiggelbout et al., 2012). In oncology, SDM is particularly crucial, fostering collaborative communication between patients and healthcare providers, which is essential for optimizing treatment outcomes and patient satisfaction in complex therapeutic decisions (Shickh et al., 2023).
Despite its recognized benefits, SDM implementation is not uniform across settings, with variations influenced by patient demographics, such as age, education level, and cultural background. Research indicates that younger, more educated patients are more likely to actively engage in treatment decisions, while older patients often prefer a more passive role, relying predominantly on medical guidance (Gieseler et al., 2019; Pyke-Grimm et al., 2020). Factors such as health literacy, decision-making dynamics, and the intricacies of cancer treatment modalities play a significant role in shaping these engagement patterns (Chang et al., 2019; Gieseler et al., 2019). In many cultural contexts, particularly in Asian countries, prevailing social norms often lead patients to defer decision-making responsibilities to FMs or HCPs (Wang et al., 2020; Sitanggang & Lin, 2024). These considerations highlight the need for a more nuanced approach that respects diverse cultural norms while upholding patient autonomy in the SDM process.
The movement towards SDM in clinical practice represents a significant advancement in modern healthcare, particularly in oncology, where treatment adherence and clinical outcomes are closely linked to patient engagement. Engaging patients in therapeutic decision-making enhances the personalization of care, enabling healthcare providers to more effectively respond to individual patient needs and preferences. However, many patients remain reliant on professional expertise, and a growing inclination toward active participation underscores the need for a balanced approach that integrates patient autonomy with professional guidance in cancer care.
Given the complexity of implementing SDM, there are considerable implications for practice, policy, and research. Clinically, HCPs must adopt communication frameworks that support SDM, incorporating decision aids and culturally tailored resources to meet local and individual needs. Health education programs would benefit from incorporating SDM-focused training, with emphasis on cross-cultural sensitivity and ethical decision-making. At the policy level, healthcare systems should advocate for patient-centered policies that incentivize SDM practices, alongside supporting the development of digital and informational infrastructures that facilitate informed decision-making. Future research should aim to validate SDM models that address cultural variability and assess their impact on long-term outcomes and patient satisfaction. This multifaceted approach holds significant promise for improving the quality of patient care, satisfaction, and health outcomes, particularly in diverse patient populations and complex care settings.
Family involvement
The findings of this review highlight the crucial role of family involvement in SDM in cancer treatment, where families often provide emotional, informational, decisional, and practical support to patients. Studies consistently show that FMs act as key advocates, helping patients navigate complex medical information and making more informed treatment decisions (Shin et al., 2017; Malhotra et al., 2020; McCaughan et al., 2022). This active involvement of families can significantly influence the patient's treatment pathway by offering a support system that reduces anxiety and enhances the patient's confidence in their choices (Shin et al., 2017; Sattar et al., 2018).
Family involvement in medical decision-making aligns with the principles of patient-centered care, which emphasize collaborative relationships between patients, families, and healthcare providers. According to the theory of relational autonomy, patients’ decisions are not made in isolation but are influenced by their relationships and the social context in which they live. This concept supports the idea that FMs' roles in decision-making contribute to a shared understanding of the patient's values and treatment goals, thus enhancing the decision-making process (Elwyn et al., 2012).
In cancer treatment decisions, families serve both as supporters and influential participants. Prior research indicates that families often assume primary or SDM roles, which substantially affects treatment choices and outcomes. For instance, a national survey by Dionne-Odom et al. found that 87.6% of family caregivers engaged in treatment decisions, with 53.9% sharing decision-making responsibilities (Dionne-Odom et al., 2023). This significant role is especially prominent among adult children of older patients, who frequently facilitate SDM, leading to more informed treatment choices (Dijkman et al., 2022). However, it is essential to maintain a balance between family involvement and patient autonomy (Hobbs et al., 2015). This family role highlights the need for clear and open communication among all parties involved, ensuring that patient autonomy is upheld while valuing family contributions
Although family involvement generally enhances the SDM process by providing emotional, informational, and practical support, it is essential to maintain a patient-centered approach in which the individual's preferences and values remain central. While families often serve as advocates and sources of strength, their influence should not override the patient's autonomy, especially in decisions with significant personal implications. HCPs play a crucial mediating role in balancing these dynamics by facilitating open dialogue that respects both the patient’s choices and the family’s perspectives, aiming to reach a consensus aligned with the patient’s best interests.
The insights from this review highlight the need for healthcare systems to adopt a more structured and culturally responsive framework for incorporating family involvement into SDM. It includes equipping HCPs with communication competencies that are sensitive to diverse familial roles and expectations, particularly in collectivist cultures where family input is traditionally more dominant. Additionally, integrating guidelines and decision-support tools that explicitly address family dynamics could improve the quality and transparency of the decision-making process. Prioritizing family engagement in SDM not only promotes holistic, person-centered care but also strengthens the therapeutic alliance between patients, families, and clinicians—ultimately contributing to better treatment experiences and outcomes.
Role of HCPs
The findings of this review suggest that HCPs play multifaceted roles in SDM. Across the included studies, HCPs were consistently involved as providers of clinical information, facilitators of decision-making, sources of emotional support, and contributors of clinical expertise throughout the treatment process. These roles are essential in helping patients navigate the complexities of cancer care, ultimately enhancing their confidence and satisfaction with the chosen treatment pathway.
These roles align closely with the principles of SDM, which advocate for collaborative communication between patients and healthcare providers. Effective communication emerged as a fundamental element, enabling patients to fully comprehend their diagnoses and treatment options, thereby supporting informed, value-based decision-making (Kehl et al., 2015; Dew et al., 2019; Heuser et al., 2023). High levels of trust in HCPs also shape how patients engage, especially in complex or urgent care (Hariati et al., 2021). HCP engagement significantly influences the implementation of patient- and family-centered care (Hariati et al., 2023). This approach also reflects the core of patient-centered care, where patients’ preferences, goals, and values are integrated into clinical decision-making (Elwyn et al., 2012).
Previous studies support these findings, emphasizing the importance of HCP communication skills in improving clinical outcomes. For instance, studies have shown that patients who perceive their healthcare providers as effective communicators report lower anxiety levels and greater satisfaction with their care (Faller et al., 2016). Additionally, studies have identified barriers to implementing SDM, including time constraints and limited formal training in communication and decision-making techniques (Légaré et al., 2008). These challenges have been further explored in recent research, particularly within the context of the UK’s National Health Service, highlighting the need for ongoing initiatives to equip HCPs with the skills necessary to engage patients effectively in treatment decisions (Joseph-Williams et al., 2017), which examined the implementation of SDM in the UK's National Health Service. Similarly, a qualitative study in Indonesia found that nurses face challenges in education due to the absence of standardized policies, limited training, and a lack of educational resources (Hariati et al., 2022). Also, a qualitative study in Indonesia highlights the challenges nurses face in providing effective discharge education due to the absence of standardized guidelines and limited training (Hariati et al., 2021). These studies collectively indicate the need for ongoing efforts to equip HCPs with the skills to engage patients in their treatment decisions effectively.
In this context, structured orientation and training programs have proven effective in improving HCPs' clinical readiness and interpersonal skills. A recent scoping review emphasizes that well-designed onboarding initiatives for nurses significantly strengthen their confidence, communication skills, and role adaptation within hospital settings (Ernawaty et al., 2024). These findings support the implementation of structured training programs to prepare nurses for such interventions. As shown by Erfina et al. (2024), nurse-delivered multimodal interventions not only address physical and psychological symptoms but also enhance the therapeutic alliance between patients and providers, an essential component of effective SDM. This finding highlights the importance of equipping nurses with both clinical and communication competencies to deliver meaningful, patient-centered cancer care.
Therefore, a more structured approach is needed to strengthen HCPs' role as facilitators in patient treatment decision-making. Although HCPs are strategically positioned to guide patients in choosing treatment options, their effectiveness is often hindered by systemic barriers such as a lack of training in SDM practices and time constraints within clinical settings. Addressing these obstacles can significantly enhance patient engagement, resulting in more personalized and satisfying healthcare experiences.
The findings of this review underscore the importance of healthcare systems prioritizing the development of training programs to improve HCPs' communication and decision-making skills. By integrating SDM principles into medical education and clinical practice, healthcare providers can bridge the gap between professional recommendations and patient preferences. Additionally, the use of digital decision aids and culturally sensitive communication strategies can promote a more inclusive and patient-centered approach across diverse healthcare settings.
These findings present several implications for clinical practice. First, adopting a more holistic approach to patient care that integrates the perspectives of patients, families, and HCPs can enhance the SDM process. Implementing SDM tools that accommodate cultural nuances can improve patient engagement, particularly among diverse patient populations. Additionally, equipping HCPs with training in cultural sensitivity and communication skills will foster more effective and empathetic interactions with patients and their families.
While this scoping review provides a comprehensive overview, certain limitations should be acknowledged. The review was limited to articles published in English and Indonesian, potentially excluding relevant studies in other languages. Moreover, most of the included studies were conducted in high-income countries, which may not fully represent the experiences of patients in low- and middle-income settings.
Future research should examine the SDM process across diverse cultural contexts and healthcare systems to provide a broader perspective. Additionally, longitudinal studies examining how interactions among patients, families, and HCPs evolve could offer deeper insights into optimizing SDM in cancer care.
Conclusion
This scoping review examined the roles of patients, families, and HCPs in the SDM process for cancer patients in clinical settings. Three primary factors emerged: Patient participation, family involvement, and support from HCPs. Active patient engagement and family involvement were shown to enhance patient confidence and satisfaction, while HCPs played critical roles as information providers and decision facilitators. Balancing patient autonomy with family input was highlighted as essential, facilitated through effective communication by HCPs. Structured frameworks and culturally sensitive training for HCPs are recommended to improve SDM, ensuring decisions are both patient-centered and value-aligned across diverse healthcare settings. These findings present several implications for clinical practice. First, adopting a more holistic approach to patient care that integrates the perspectives of patients, families, and HCPs can enhance the SDM process. Implementing SDM tools that accommodate cultural nuances can improve patient engagement, particularly among diverse patient populations. Additionally, equipping HCPs with training in cultural sensitivity and communication skills will foster more effective and empathetic interactions with patients and their families.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization: Fadiah Izzati Salim and Suni Hariati;Methodology: Fadiah Izzati Salim and Andi Masyitha Irwan; Investigation and data curation: Fadiah Izzati Salim and Andi Masyitha Irwan; Data analysis, validation and visualization: Suni Hariati and Erfina Erfina; Writing the original draft: Fadiah Izzati Salim, Suni Hariati, and Andi Masyitha Irwan; Review, editing and final approval: All authors; Supervision: Suni Hariati.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank Kusrini Kadar, for her proofreading of this article.
References
American Cancer Society., 2024. What is cancer? Retrieved from: [Link]
Aromataris, E. & Munn, Z., 2020. JBI manual for evidence synthesis. Adelaide: JBI. [Link]
Barry, M. J. & Edgman-Levitan, S., 2012.‘Shared decision making - the pinnacle of patient-centered care. New England Journal of Medicine, 366(9), pp. 780-1. [DOI:10.1056/nejmp1109283]
Berry, D. L., et al., 2015. ‘Treatment decision making in patients with bladder cancer. Bladder Cancer, 1(2), pp. 151-8. [DOI:10.3233/BLC-150029] [PMID]
Chang, H. L., Li, F. S. & Lin, C. F., 2019. Factors influencing implementation of shared medical decision making in patients with cancer. Patient Preference and Adherence, 13, pp. 1995-2005. [DOI:10.2147/PPA.S217561] [PMID]
Covvey, J. R. et al., 2019. ‘Barriers and facilitators to shared decision-making in oncology: A systematic review of the literature. Supportive Care in Cancer, 27(5), pp. 1613-7. [DOI:10.1007/s00520-019-04675-7] [PMID]
D’Agostino, T. A. et al., 2018. ‘Treatment decision making in early-stage papillary thyroid cancer. Psycho-Oncology, 27(1), pp. 61-8. [DOI:10.1002/pon.4383]
Dew, K. et al., 2019. Cancer care decision-making and treatment consent: An observational study of patients’ and clinicians’ rights. Journal of Sociology, 55(1), pp. 161-78. [DOI:10.1177/1440783318773880]
Dijkman, B. L., et al., 2022. ‘Involvement of adult children in treatment decision-making for older patients with cancer - a qualitative study of perceptions and experiences of oncology surgeons and nurses. Supportive Care in Cancer, 30(11), pp. 9203-10. [DOI:10.1007/s00520-022-07349-z] [PMID]
Dionne-Odom, J. N., et al., 2023. Family caregiver roles and challenges in assisting patients with cancer treatment decision-making: Analysis of data from a national survey. Health Expectations, 26(5), pp. 1965-76. [DOI:10.1111/hex.13805] [PMID]
Elwyn, G., et al., 2012. Shared decision making: A model for clinical practice. Journal of General Internal Medicine, 27(10), pp. 1361-7. [DOI:10.1007/s11606-012-2077-6] [PMID]
Erfina, E., et al., 2024. Effectiveness of a multimodal nursing intervention on quality of sleep, fatigue, and level of depression among Indonesian patients with gynecological cancer: A pilot study. Cancer Nursing, 47(1), pp. 72-80. [DOI:10.1097/NCC.0000000000001158] [PMID]
Ernawaty, E., Hariati, S. & Saleh, A., 2024. Program components, impact, and duration of implementing a new nurse orientation program in hospital contexts: A scoping review. International Journal of Nursing Studies Advances, 7, pp. 100214. [DOI:10.1016/j.ijnsa.2024.100214] [PMID]
Faller, H., et al., 2016. ‘Satisfaction with information and unmet information needs in men and women with cancer. Journal of Cancer Survivorship, 10(1), pp. 62-70. [DOI:10.1007/s11764-015-0451-1] [PMID]
Gieseler, F., et al., 2019. ‘Adherence of Older Breast Cancer Patients to Cancer Therapy Recommendations. Diversity & Equality in Health and Care, 16(1), pp. 11-17. [DOI:10.21767/2049-5471.1000187]
Gu, X. F. et al., 2023. Involvement in treatment decision-making and self-reported efficacy among patients with advanced colorectal cancer: A nationwide multicenter cross-sectional study. Frontiers in Oncology, 13, pp. 1-16. [DOI:10.3389/fonc.2023.1168078] [PMID]
Hariati, S., et al., 2021. ‘Indonesian mothers’ beliefs on caring practices at home for preterm babies after hospital discharge: A qualitative study. Journal for Specialists in Pediatric Nursing, 26(3), pp. 1-12. [DOI:10.1111/jspn.12330] [PMID]
Hariati, S., et al., 2022. Exploring Indonesian nurses’ perspectives on preparing parents of preterm infants for hospital discharge: A qualitative study. Journal of Neonatal Nursing, 28(1), pp. 59-66. [DOI:10.1016/j.jnn.2021.07.002]
Hariati, S. et al., 2023. Indonesian mothers of premature infants’ experiences in achieving initial motherhood independence in the neonatal unit: A qualitative study. Journal of Neonatal Nursing, 29(2), pp. 283-9. [DOI:10.1016/j.jnn.2022.07.001]
Heuser, C., et al., 2023. Shared-decision-making experiences in breast cancer care with and without patient participation in multidisciplinary tumor conferences: A mixed-methods-study. Journal of Multidisciplinary Healthcare, 16, pp. 397-409. [DOI:10.2147/JMDH.S397300] [PMID]
Hobbs, G. S., et al., 2015. The role of families in decisions regarding cancer treatments. Cancer, 121(7), pp. 1079-87. [DOI:10.1002/cncr.29064] [PMID]
Holdsworth, L. M., et al., 2020. Along for the Ride: A qualitative study exploring patient and caregiver perceptions of decision making in cancer care. MDM Policy and Practice, 5(1), pp. 1-9. [DOI:10.1177/2381468320933576]
Joseph-Williams, N., et al., 2017. Implementing shared decision making in the NHS: lessons from the MAGIC programme. BMJ, 357, pp. j1744. [DOI:10.1136/bmj.j1744] [PMID]
Kehl, K. L., et al., 2015. Association of actual and preferred decision roles with patient-reported quality of care: Shared decision making in cancer care. JAMA Oncology, 1(1), pp. 50-8. [DOI:10.1001/jamaoncol.2014.112] [PMID]
Khullar, N., et al., 2018. Impact of cancer diagnosis on different aspects of life of patients of cancer breast and cancer cervix uteri: A cross sectional study at Government Medical College, Amritsar, Punjab. International Journal of Community Medicine And Public Health, 5(5), pp. 2053. [DOI:10.18203/2394-6040.ijcmph20181722]
Laidsaar-Powell, R., et al., 2016. Family involvement in cancer treatment decision-making: A qualitative study of patient, family, and clinician attitudes and experiences. Patient Education and Counseling, 99(7), pp. 1146-55. [DOI:10.1016/j.pec.2016.01.014] [PMID]
Légaré, F., et al., 2008. Barriers and facilitators to implementing shared decision-making in clinical practice: Update of a systematic review of health professionals’ perceptions. Patient Education and Counseling, 73(3), pp. 526-35. [DOI:10.1016/j.pec.2008.07.018] [PMID]
Légaré, F. & Witteman, H. O., 2013. Shared decision making: Examining key elements and barriers to adoption into routine clinical practice. Health Affairs, 32(2), pp. 276-84. [DOI:10.1377/hlthaff.2012.1078] [PMID]
Magnusson, R., 2020. Non-Communicable Diseases and Global Health Politics. In C. McInnes, K. Lee & J. Youde (Eds.), The Oxford Handbook of Global Health Politics. Oxford: Oxford University Press. [DOI:10.1093/oxfordhb/9780190456818.013.35]
Malhotra, C., et al., 2020. Oncologist-patient-caregiver decision-making discussions in the context of advanced cancer in an Asian setting. Health Expectations, 23(1), pp. 220-8. [DOI:10.1111/hex.12994] [PMID]
McCaughan, D., et al., 2022. Treatment decision making (TDM): A qualitative study exploring the perspectives of patients with chronic haematological cancers. BMJ Open, 12(3), pp. e050816. [DOI:10.1136/bmjopen-2021-050816] [PMID]
Mokhles, S., et al., 2018. Treatment selection of early stage non-small cell lung cancer: The role of the patient in clinical decision making. BMC Cancer, 18(1), pp. 1-10. [DOI:10.1186/s12885-018-3986-5] [PMID]
Nakayama, K., et al., 2020. Shared decision making, physicians’ explanations, and treatment satisfaction: A cross-sectional survey of prostate cancer patients. BMC Medical Informatics and Decision Making, 20, pp. 1-10. [PMID]
No author. Open science framework. [Internet] 2024. Retrieved from: [Link]
Ouzzani, M. et al., 2016. Rayyan-a web and mobile app for systematic reviews. Systematic Reviews, 5(1), pp. 1-10. [DOI:10.1186/s13643-016-0384-4] [PMID]
Pinker, I. & Pilleron, S., 2023. Attitudes of healthcare professionals in treatment decision-making for older adults with cancer: A scoping review protocol. BMJ Open, 13(10), pp. 1-5. [DOI:10.1136/bmjopen-2023-077628]
Pitman, A., et al., 2018. Depression and anxiety in patients with cancer. BMJ, 361, pp. 1-6. [DOI:10.1136/bmj.k1415] [PMID]
Pozzar, R., et al., 2018. Patient, physician, and caregiver perspectives on ovarian cancer treatment decision making: Lessons from a qualitative pilot study. Pilot and Feasibility Studies, 4(1), pp. 91. [DOI:10.1186/s40814-018-0283-7] [PMID]
Pyke-Grimm, K. A., et al., 2020. ‘3 Dimensions of Treatment Decision Making in Adolescents and Young Adults with Cancer. Cancer Nursing, 43(6), pp. 436-45. [DOI:10.1097/NCC.0000000000000820] [PMID]
No author. Rayyan [Internet] 2024. Retrieved from: [Link]
Sattar, S., et al., 2018. Chemotherapy and radiation treatment decision-making experiences of older adults with cancer: A qualitative study. Journal of Geriatric Oncology, 9(1), pp. 47-52. [DOI:10.1016/j.jgo.2017.07.013] [PMID]
Schuler, M., et al., 2017. Cancer patients’ control preferences in decision making and associations with patient-reported outcomes: A prospective study in an outpatient cancer center. Supportive Care in Cancer, 25(9), pp. 2753-60. [DOI:10.1007/s00520-017-3686-8] [PMID]
Shickh, S., et al., 2023. Shared Decision Making in the Care of Patients With Cancer. American Society of Clinical Oncology Educational Book, (43), pp. 1-13. [DOI:10.1200/edbk_389516] [PMID]
Shin, D. W., et al., 2017. Attitudes toward family involvement in cancer treatment decision making: The perspectives of patients, family caregivers, and their oncologists. Psycho-Oncology, 26(6), pp. 770-8. [DOI:10.1002/pon.4226] [PMID]
Sitanggang, Y. F. & Lin, H. R., 2024. Experiences of Indonesian women with breast cancer underwent treatment decision-making: A qualitative study. Belitung Nursing Journal, 10(4), pp. 456-63. [DOI:10.33546/bnj.3395] [PMID]
Spronk, I., et al., 2018. The availability and effectiveness of tools supporting shared decision making in metastatic breast cancer care: A review. BMC Palliative Care, 17(1), pp. 1-8. [DOI:10.1186/s12904-018-0330-4] [PMID]
Stiggelbout, A. M., et al., 2012. Shared decision making: Really putting patients at the centre of healthcare. BMJ, 344(7842), pp. 1-6. [DOI:10.1136/bmj.e256] [PMID]
Stone, L. & Olsen, A., 2022. ‘Illness uncertainty and risk management for people with cancer. Australian Journal of General Practice, 51(5), pp. 321-6. [DOI:10.31128/AJGP-05-21-5992] [PMID]
Tariman, J. D., et al., 2012. Physician, patient, and contextual factors affecting treatment decisions in older adults with cancer and models of decision making: A literature review. Oncology Nursing Society, 39(1). [DOI:10.1188/12.ONF.E70-E83] [PMID]
Tilly, A. E., et al., 2023. Kusankha Pamodzi: Health care decision-making preferences among patients with cancer in Malawi. Palliative Medicine Reports, 4(1), pp. 127-32. [DOI:10.1089/pmr.2023.0002] [PMID]
Tricco, A. C., et al., 2018. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Annals of Internal Medicine, 169(7), pp. 467–73. [DOI:10.7326/M18-0850] [PMID]
Wang, L., et al., 2020. Treatment decision-making, family influences, and cultural influences of Chinese breast cancer survivors: A qualitative study using an expressive writing method. Supportive Care in Cancer, 28(7), pp. 3259-66. [DOI:10.1007/s00520-019-05161-w]
WHO., 2022. Cancer. Geneva: WHO. [Link]
Zucca, A., et al., 2014.‘Patient-centred care: Making cancer treatment centres accountable. Supportive Care in Cancer, 22(7), pp. 1989-97. [DOI:10.1007/s00520-014-2221-4] [PMID]
Type of Study: Review Article |
Subject:
General
Received: 2024/12/5 | Accepted: 2025/07/1 | Published: 2026/02/1
Received: 2024/12/5 | Accepted: 2025/07/1 | Published: 2026/02/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
