Sun, Jun 7, 2026
[Archive]
Volume 12, Issue 1 (Winter 2026)
JCCNC 2026, 12(1): 33-46 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Bekti Prasetyo Y, Ika Wardojo S S. From Birth Size to Birth Order: Predictors of Child Mortality. JCCNC 2026; 12 (1) :33-46
URL: http://jccnc.iums.ac.ir/article-1-782-en.html
URL: http://jccnc.iums.ac.ir/article-1-782-en.html



1- Department of Community Nursing, Faculty of Health Sciences, University Muhammadiyah of Malang, Malang, Indonesia. , yoyok@umm.ac.id
2- Department of Community Nursing, Faculty of Health Sciences, University Muhammadiyah of Malang, Malang, Indonesia.
2- Department of Community Nursing, Faculty of Health Sciences, University Muhammadiyah of Malang, Malang, Indonesia.
Keywords: Child mortality, Birth order, Birth weight, Socioeconomic factors, Receiver operating characteristic (ROC) analysis
Full-Text [PDF 687 kb]
(271 Downloads)
| Abstract (HTML) (451 Views)
Full-Text: (39 Views)
Introduction
Information on mortality among children under 5 years is vital for describing a country’s health status and the quality of its community’s life (Debere & Adjiwanou, 2024; Hossain et al., 2024). At the same time, the mortality of children under 5 years is a crucial measure of a country’s socioeconomic and demographic progress and quality of life (QoL), particularly in families (Wahl et al., 2023). Lack of competent human resources, poor infrastructure, and underinvestment in health systems have dramatically raised child mortality rates in low- and middle-income countries (Dauda et al., 2024; Mekonnen et al., 2024a)urban areas generally have better access to and use of maternal, newborn, and child health (MNCH).
Child mortality is still a crucial global issue, particularly in Indonesia. The mortality rate for children under 5 years of age declined by 49%, from 77 deaths per 1000 live births in 2000 to 39 deaths in 2017, or 1 in every 14 children dying in 2017 (WHO, 2019). Indonesia has been attempting to reduce child mortality each year, and the rate is decreasing. The 2017 Indonesia demographic and health survey (IDHS) statistics show a neonatal mortality rate (NMR) of 15 per 1000 live births, an infant mortality rate of 24 per 1000 live births, and a toddler mortality rate of 32 per 1000 live births (Ministry of Health Indonesia, 2019; Statista, 2021). Of course, this figure remains far from the sustainable development goals (SDGs), which set a target of 12 per 1000 live births for child mortality (WHO, 2015).
In 2019, low birth weight (Wulandari et al., 2022) was the leading cause of infant death in Indonesia. Other reasons for death were hypoxia, congenital disabilities, infection, and newborn tetanus (Soleman, 2020). In Indonesia, the factors influencing child mortality include maternal age at birth, birth spacing, and the child’s weight at birth. A child’s birth weight affects their nutritional health and immunological system (Soleman, 2020). Indonesia’s national policy for children’s health states that every child has the right to survive, grow, and develop, as well as the right to be protected from violence and discrimination, underscoring the need for integrated, comprehensive, and sustainable child health initiatives (Kemenkes, 2022). Child health efforts in Indonesia include prenatal care, newborn and infant health, toddler and preschooler health, school-age child and adolescent health, and child health protection (Kemenkes, 2022). However, Indonesia strives to reduce the mortality rate of children under 5 by the SDGs target by 2030.
This research introduces a novel approach, employing receiver operating characteristic (ROC) curve analysis to assess and compare the predictive accuracy of various models for identifying key factors contributing to child mortality in Indonesia. Unlike previous studies that have examined the determinants of child mortality, this research distinguishes itself by focusing on ROC curves—a method not commonly used in public health research in this context. By integrating ROC analysis, the study offers a more robust and comprehensive evaluation of predictive models, highlighting their sensitivity, specificity, and accuracy. Furthermore, the research provides context-specific insights by addressing Indonesia’s unique socioeconomic, cultural, and healthcare-related factors, ensuring that the findings are highly relevant to local policymakers and healthcare providers.
Despite extensive global research on child mortality, significant gaps remain, particularly within the Indonesian context. One such gap is the limited application of ROC analysis in public health research on child mortality in Indonesia, which this study addresses by offering a nuanced understanding of the predictive power of various factors. Additionally, while much of the existing literature relies on generalized models, this research focuses on Indonesia-specific data, providing insights more applicable to the local context. The study also bridges the gap in integrating multiple predictors by simultaneously evaluating them through ROC analysis, enabling a more comprehensive understanding of their collective impact. Finally, by systematically comparing predictive models, the research addresses the lack of comparative analysis in existing studies and ultimately identifies the most effective strategies for reducing child mortality in Indonesia.
The theoretical foundation of this study is rooted in the determinants of child mortality, which encompass demographic, socioeconomic, biological, and healthcare-related factors. The conceptual model integrates key elements from public health and epidemiological theories, including the life-course perspective and the social determinants of health framework. These frameworks emphasize the interplay of maternal, neonatal, and environmental factors in shaping child survival outcomes. Maternal education, socioeconomic status, and access to healthcare are critical predictors that influence child health and mortality (Ogunniyi et al., 2024; Zhang et al., 2024). These elements provide a structured approach to understanding the multifaceted nature of child mortality, aligning with global health theories on inequality, resource access, and health system efficiency.
The conceptual framework of this research introduces ROC analysis as a novel method to evaluate predictive models of child mortality. ROC analysis is a tool for assessing the accuracy of predictors such as birth size and birth order by quantifying their sensitivity and specificity (Obuchowski & Bullen, 2018). This approach integrates predictive analytics into public health research, offering a deeper understanding of how individual factors contribute to child mortality risk. The framework emphasizes the relative predictive power of birth characteristics by comparing the area under the curve (AUC) values of different predictors. It situates them within a broader context of healthcare disparities and maternal health factors. This methodology provides a structured means to evaluate the effectiveness of targeted interventions to reduce child mortality.
The framework also incorporates Indonesia’s unique socioeconomic and cultural context, recognizing the influence of maternal health practices, birth traditions, and healthcare accessibility on child mortality. This perspective aligns with Bronfenbrenner’s ecological systems theory, highlighting the interaction between individual and environmental factors (Ogunniyi et al., 2024). The study acknowledges that child mortality in Indonesia is not only influenced by biological determinants but also by external factors such as maternal age, birth spacing, healthcare infrastructure, and cultural norms. These elements underscore the importance of a holistic approach that integrates individual-level and systemic-level predictors into a cohesive model, ensuring the findings are contextually relevant to Indonesian healthcare policies.
This study’s framework bridges critical gaps in child mortality research by emphasizing the application of advanced predictive analytics and context-specific data. Unlike traditional models, which often focus on singular or generalized predictors, this framework evaluates multiple determinants simultaneously to capture their collective impact. The innovative use of ROC analysis offers a more nuanced understanding of the predictive power of factors such as birth size and birth order, which are often underexplored in the public health literature. Furthermore, integrating Indonesia-specific data addresses the limited applicability of global models to local contexts, enhancing the study’s relevance and utility for policymakers. By aligning theoretical insights with practical applications, the framework aims to contribute to effective, evidence-based interventions to reduce child mortality in Indonesia. In this study, we analysed predictors of child mortality using secondary data from the 2017 IDHS and evaluated the predictive ability of birth size and birth order through ROC analysis.
Materials and Methods
Study design
The cross-sectional design allows for examining data collected at a single point in time, providing a snapshot of the factors associated with child mortality in Indonesia. This approach is well-suited for identifying potential predictors and assessing their relationship with child mortality, using secondary data from the 2017 IDHS.
Sample and data collection
This study used secondary data from the 2017 IDHS. The IDHS utilized standardized questionnaires developed by the demographic and health surveys (DHS) program, including the household questionnaire, the women’s questionnaire, and the child health questionnaire. These instruments were adapted to the Indonesian context and pretested to ensure cultural relevance. The validity and reliability of the IDHS instruments are well established internationally, as they undergo rigorous methodological development and field testing. In Indonesia, the Ministry of Health conducted the survey in collaboration with the National Population and Family Planning Board and the Central Statistics Agency, ensuring high-quality, nationally representative data.
The study’s population consisted of women aged 15-49, from whom data were collected using a multistage stratified random sampling technique. In the first stage, several census blocks (enumeration areas) were randomly selected from each stratum using probability proportional to size. In the second stage, 25 households were randomly selected from each chosen census block. This method ensures that the sample is nationally representative and covers various geographic and social groups nationwide.
The total initial sample comprised 17848 respondents. Data were collected by a team of 1160 trained personnel who administered the survey and ensured data quality. The survey collected detailed information on various factors, including socioeconomic status, healthcare access, maternal and child health indicators, and more. A thorough data-cleaning process was conducted to ensure the integrity of the analysis. Incomplete responses and unanswered questions from respondents were carefully removed from the dataset. After this process, a final sample of 13946 respondents was obtained, which served as the core dataset for analysis in this study.
Study variables
The study investigated a range of independent variables to assess their impact on child mortality in Indonesia. These variables encompassed the child’s age, gender, place of residence, parental education, and issues such as vaginal bleeding during pregnancy. Factors such as the child’s birth weight, antenatal care, and the mother’s knowledge of danger signs during pregnancy were examined. The study classified children’s ages into 0-24 months (coded 0) and 25-59 months (coded 1). Gender was recorded as male (coded 1) or female (coded 2), while residence was categorized as urban (coded 1) or rural (coded 2). Maternal education was divided into four levels: No schooling (coded 0), primary (coded 1), secondary (coded 2), and higher education (coded 3). Vaginal bleeding during pregnancy was noted as either “yes” or “no,” and the child’s size at birth was categorized into 6 groups ranging from very large (coded 1) to unknown size (coded 8).
Further variables included antenatal care (no [coded 0] or yes [coded 1]) and the mother’s knowledge of danger signs during pregnancy (no [coded 0] or yes [coded 1]). Economic status was divided into 5 categories: Poorest (coded 1), poorer (coded 2), middle (coded 3), richer (coded 4), and richest (coded 5). The number of births was categorized into three groups: 1-2 births (coded 0), 3-5 births (coded 1), and 6-13 births (coded 2). The timing of the child’s initial access to the mother’s nipple was dichotomized into immediate (coded 0) or delayed (coded 1). The dependent variable was the child’s survival status, with survival coded as 1 (yes) and non-survival as 0 (no).
Data analysis
Categorical variables were summarized using frequency distributions and percentages to analyze predictors of child mortality in Indonesia, providing a clear overview of their prevalence and distribution. Relationships between predictors and child mortality were examined using cross-tabulation and chi-square tests. significant predictors were identified through multivariable logistic regression, with a P value threshold of <0.05, and non-significant variables were excluded using backward elimination. The final model’s predictive performance was evaluated using an ROC curve, which plots sensitivity versus specificity to assess accuracy and discriminative ability, providing insights into the model’s effectiveness in predicting child mortality.
Results
Respondents’ characteristics
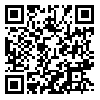
Table 1 outlines the characteristics of the respondents (n=13946) and offers valuable insights into factors related to child mortality in Indonesia. The data reveal that a majority of the children were aged 25-59 months (53.4%), with a near-equal distribution between male (51.2%) and female (48.9%) children. The respondents’ residence was almost evenly split between urban (49.8%) and rural (50.2%) areas. Educational attainment of the mothers varied, with a majority having secondary education (56.2%), while only a tiny fraction had no formal education (1.2%). Additionally, issues such as vaginal bleeding during pregnancy were reported by 45.3% of respondents, and a significant portion (54.7%) did not experience this complication.
Further data analysis shows that most children were of average size at birth (53.6%), with a notable proportion classified as larger than average (27.5%). Antenatal care was significantly underutilized, with 85.4% of respondents reporting no such care. Knowledge of danger signs during pregnancy was more prevalent, with 65.7% of mothers aware of them. Economic status was diverse, with the wealth index ranging from the poorest (25.6%) to the richest (17.3%). Birth order data indicate that most children were first- or second-born (64.2%), and the timing of initial breastfeeding shows that 57.6% were breastfed immediately after birth. The survival status of children was overwhelmingly positive, with 99.2% reported to be alive. This study only included one child per mother to clarify the analysis and avoid confusion. We chose the last-born child under 5 because the 2017 IDHS collects the most complete and detailed information on the most recent child, including health, nutrition, and survival. Using the last-born child also helps reduce errors since mothers usually remember recent events better than older ones. These findings underscore the diverse demographic, socioeconomic, and health-related factors that contribute to child mortality, providing a foundation for targeted interventions and further research (Table 1).
Predictors of child mortality
Table 2 outlines the bivariate analysis and cross-tabulation of the outcome variable against various covariates from the 2017 IDHS dataset, revealing important insights into factors influencing child mortality. The child’s age showed no significant association with mortality; both age groups (0-24 months and 25-59 months) had similar odds ratios (OR=0.94; 95% CI, 0.65%, 1.36%; P=0.755). Similarly, the sex of the child did not appear to influence survival outcomes, as the odds of mortality for male children were not significantly different from those of female children (OR=1.162; 95% CI, 0.80%, 1.68%; P=0.428). However, the place of residence presented a near-significant association, with children in urban areas showing a trend toward lower mortality odds than those in rural areas (OR=0.690; 95% CI, 0.47%, 1%; P=0.052).

Maternal education level emerged as a significant predictor of child mortality. Children born to mothers with no education had significantly higher odds of mortality compared to those whose mothers had higher education (OR=3.750; 95% CI, 1.23%, 11.34%; P<0.001). Additionally, primary education was associated with increased odds of mortality (OR =1.979; 95% CI, 1.11%, 3.51%). Vaginal bleeding during pregnancy also showed a significant association, with children whose mothers experienced this complication having higher odds of mortality compared to those without such issues (OR=1.580; 95% CI, 1.07%, 2.33%; P=0.020).
The size of the child at birth was another critical factor, with very large, larger-than-average, and average-sized children all demonstrating significantly lower odds of mortality compared to tiny children. Specifically, very large children had the lowest odds (OR=0.130; 95% CI, 0.03%, 0.44%; P<0.001). The wealth index also indicated economic disparities in child survival, with children from the poorest households showing significantly higher odds of mortality than those from the richest households (OR=1.919; 95% CI, 1.10%, 3.34%; P=0.001). Lastly, birth order was a strong predictor, with first and second-born children showing significantly higher odds of mortality than those who were sixth to thirteenth in Birth order (OR=0.168; 95% CI, 0.09%, 0.30%; P<0.001). These findings underscore the importance of socioeconomic factors, maternal health, and birth characteristics in determining child survival in Indonesia.
Model of child mortality
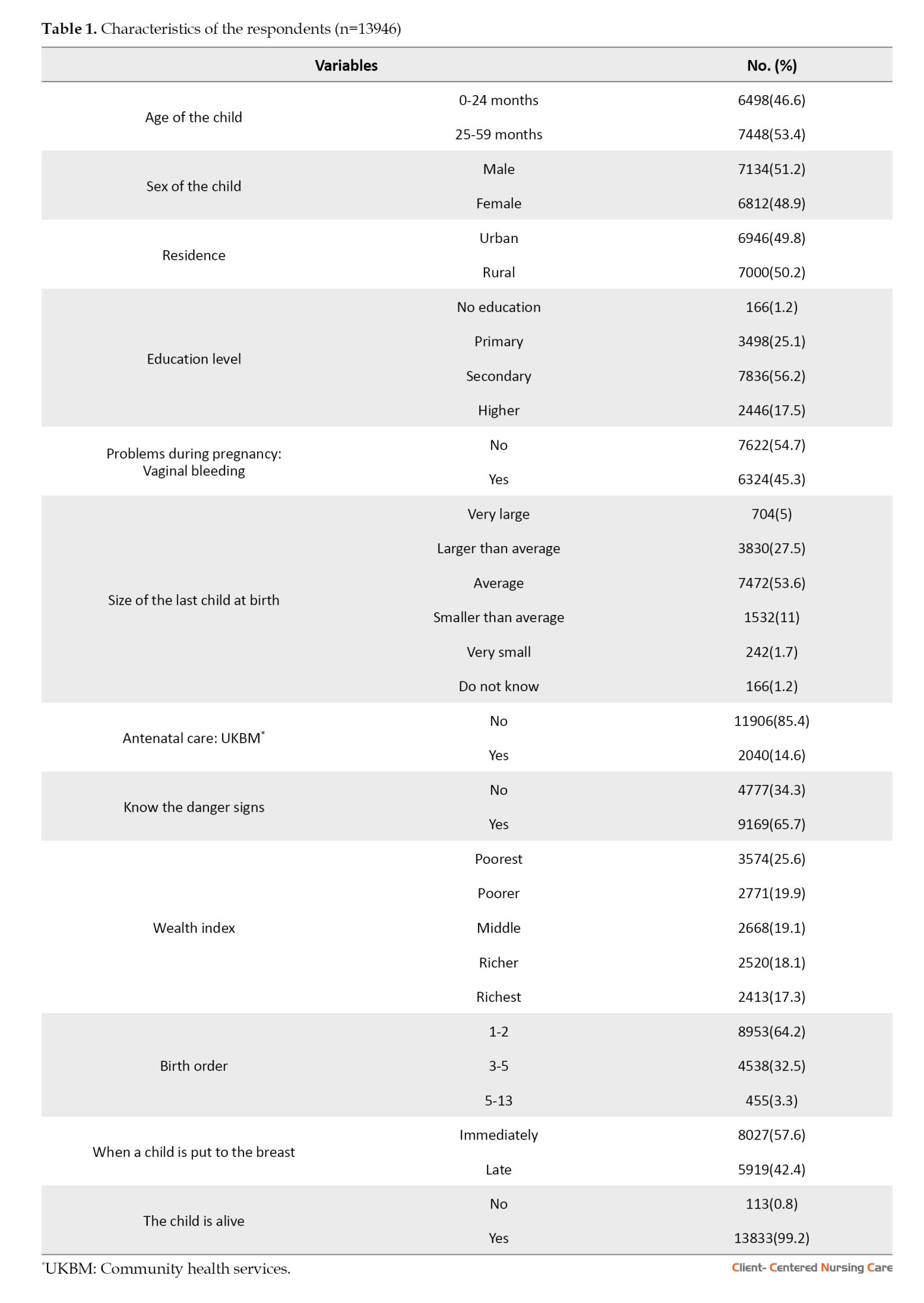
The multivariate analysis of child mortality using the 2017 IDHS data highlights the significant influence of birth size and birth order on child survival. The size of the child at birth emerged as a critical predictor, with very large, larger-than-average, and average-sized children exhibiting significantly higher odds of mortality compared to very small children. Specifically, very large children had an odds ratio of 5.964 (95% CI, 1.698%, 20.942%; P=0.005), while larger-than-average and average-sized children had ORs of 5.554 (95% CI, 2.284%, 13.506%; P<0.001) and 3.922 (95% CI, 1.719%, 8.949%; P=0.001), respectively. Even children who were smaller than average had a higher risk of mortality, with an OR of 2.887 (95% CI, 1.155%, 7.214%; P=0.023) when compared to very small children who served as the reference group. These findings suggest that extremes in birth size, particularly very large sizes, are associated with a higher risk of mortality, underscoring the importance of monitoring and managing birth outcomes (Table 3).
Birth order also played a significant role in determining child survival. Children who were first or second-born had significantly higher odds of mortality (OR=5.209; 95% CI, 2.861%, 9.483%; P<0.001) compared to those who were sixth to thirteenth in birth order. Similarly, third to fifth-born children also faced increased mortality risk, with an OR of 2.836 (95% CI, 1.552%, 5.184%; P=0.001). This pattern indicates that lower birth order is associated with higher mortality, potentially due to resource allocation, maternal health, or caregiving capacity. Notably, education level, pregnancy-related issues such as vaginal bleeding, and wealth index were excluded from the final model because their P values exceeded 0.05, suggesting that these factors were not significant predictors of child mortality after controlling for other variables. This result emphasizes the critical impact of birth characteristics over socioeconomic and maternal health factors in this context (Table 3).
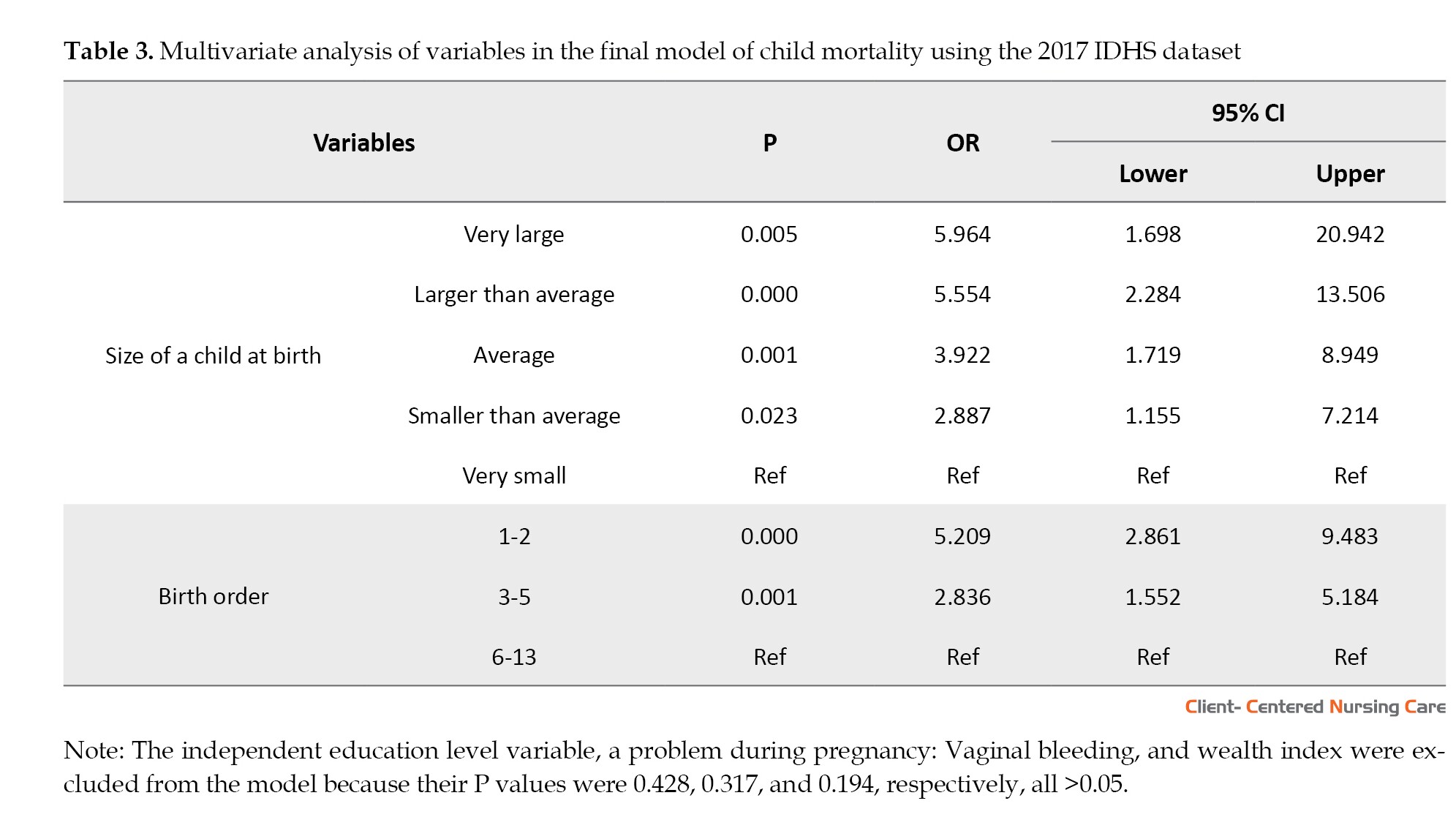
The ROC curve was used to evaluate the predictive ability of the final model for child mortality in Indonesia, focusing on two key predictors: birth weight and birth order. The AUC measures the model’s accuracy, with higher values indicating better discriminative power. In this study, the AUC for birth order was 0.611, suggesting that this variable has modest predictive ability, correctly classifying child mortality outcomes approximately 61% of the time. On the other hand, the child’s birth weight had an AUC of 0.582, indicating slightly lower predictive ability, with the model correctly classifying outcomes about 58% of the time (Figure 1).
These AUC values reflect the model’s overall performance in predicting child mortality based on these two variables. Although both predictors demonstrate some ability to distinguish between children who survive and those who do not, the relatively moderate AUC values suggest room for improvement in the model’s predictive power. Birth order appears to be a slightly stronger predictor than the child’s birth size, but neither alone is highly accurate. These findings highlight the need to consider additional factors or refine the model further to enhance its ability to predict child mortality more precisely in the Indonesian context.
Discussion
Characteristics of the respondents
The findings from the respondents’ characteristics in Table 1 provide a detailed view of the factors influencing child mortality in Indonesia. The near-equal distribution of male and female children and the balanced urban and rural residency suggest that gender and location might not be significant determinants of child mortality on their own. However, these variables should still be considered in a broader analysis that includes other socioeconomic and health-related factors (Amegbor & Addae, 2023; Ahmed & Atiqul Haq, 2024; Hossain et al., 2024).
Mothers’ educational attainment emerged as a critical factor, with the majority having secondary education. This finding suggests that education is vital to child health outcomes, potentially affecting mothers’ ability to access healthcare, understand health risks, and make informed decisions about their children’s wellbeing (Khani Jeihooni et al., 2022; Nishad & Sinha, 2023; Zhang et al., 2024). The presence of pregnancy complications, such as vaginal bleeding, reported by 45.3% of respondents, is another significant concern, highlighting the need for improved maternal healthcare services, especially during pregnancy (Seid et al., 2023; Girchenko et al., 2024).
The data on antenatal care utilization reveal a glaring gap: 85.4% of respondents reported no antenatal care. This underutilization is alarming and points to potential barriers to accessing healthcare services, which could contribute to higher risks of child mortality. Additionally, knowledge of danger signs during pregnancy, although relatively high at 65.7%, indicates that a significant portion of the population still lacks critical awareness, which could delay seeking care and lead to adverse outcomes (Pai et al., 2023; Tiruye & Shiferaw, 2023).
The economic disparities reflected in the wealth index suggest that child mortality risk may vary across socioeconomic groups, with the poorest potentially more vulnerable (Hossain et al., 2024). The timing of initial breastfeeding and the survival status of children further reinforce the importance of immediate postnatal care and interventions (Rosenberg et al., 2024). Overall, these results emphasize the need for targeted public health interventions that address education, access to maternal and child healthcare, and socioeconomic inequalities to reduce child mortality in Indonesia.
Predictors of child mortality
The bivariate analysis and cross-tabulation of factors influencing child mortality in Indonesia provide significant insights into the complex interplay of demographic, socioeconomic, and health-related variables. One of the most striking findings is the non-significant association between child mortality and variables like the age and sex of the child. This finding suggests that, in this context, survival outcomes are not predominantly determined by these demographic factors but rather by other underlying conditions. However, the near-significant association between urban residence and lower mortality odds highlights the potential influence of environmental factors, such as access to healthcare, sanitation, and other public health resources, which are often more readily available in urban settings (Girma et al., 2023; Khan et al., 2023).
Maternal education level stands out as a critical predictor of child survival, with the data clearly showing that children born to mothers with no formal education face significantly higher mortality risks. This finding underscores the pivotal role of maternal education in enhancing child health outcomes, likely due to better health literacy, improved utilization of healthcare services, and greater awareness of child-rearing practices (Oyekale & Maselwa, 2018; Yaya et al., 2019; Ifada et al., 2020; Balaj et al., 2021). The strong association between maternal education and child survival suggests that public health interventions to improve women's educational opportunities could substantially reduce child mortality in Indonesia (Yaya et al., 2018; Zhang et al., 2024).
The analysis also highlights the importance of maternal health during pregnancy, as evidenced by the significant association between vaginal bleeding and increased child mortality. This finding emphasizes the need for enhanced prenatal care and monitoring, especially for high-risk pregnancies, to mitigate complications that could lead to adverse outcomes (Combellick et al., 2024; Mekonnen et al., 2024b). Additionally, the size of the child at birth and the birth order emerged as strong predictors of survival, with large children and those born early in birth order facing higher mortality risks. These findings highlight the importance of targeted interventions, such as improved maternal nutrition and family planning, to address these risk factors (Bango & Ghosh, 2023; Masquelier et al., 2023; Debere & Adjiwanou, 2024).
Economic disparities, as reflected in the wealth index, further complicate the picture of child mortality in Indonesia (Amini Rarani et al., 2018; Yaya et al., 2020). The higher odds of mortality among children from the poorest households compared to those from wealthier backgrounds suggest that socioeconomic inequalities play a crucial role in child survival (Amini Rarani et al., 2018; Balaj et al., 2021). This finding highlights the need for policies and programs that address these disparities by improving access to healthcare, nutrition, and other essential services for the most vulnerable populations. The research underscores the multifaceted nature of child mortality in Indonesia, driven by socioeconomic, health, and demographic factors. Addressing these issues through comprehensive public health strategies will be essential in reducing child mortality and improving overall child health outcomes in the country (Garcia et al., 2023; Ghazy et al., 2024).
Model of child mortality
The multivariate analysis of child mortality from the 2017 IDHS offers critical insights into the factors significantly influencing child survival in Indonesia. The analysis reveals that birth size is a crucial determinant of mortality risk, with both very large and larger-than-average sizes associated with significantly higher odds of mortality compared to very small children (Kim et al., 2022). Interestingly, while small size is often considered a risk factor, this analysis indicates that the extremes in birth size, particularly large or larger than average, pose an even greater risk. These findings may reflect complications associated with delivery or underlying health conditions in larger infants, necessitating careful monitoring and medical intervention (Memiah et al., 2020) infant, and child deaths occur in low- and middle-income countries (LMICs. The strong association between birth size and mortality underscores the importance of prenatal care focused on monitoring fetal growth and ensuring appropriate measures are taken during delivery to manage potential complications (Yaya et al., 2020; Chang et al., 2021) the NMR.
Birth order also emerged as a significant predictor of child mortality, with first and second-born children facing notably higher risks compared to those born later in the birth sequence. This pattern might be explained by parental inexperience, less developed maternal health during first births, or higher stress and resource strain in larger families that could disadvantage early-born children. However, the finding that first- and second-born children are at higher risk suggests that targeted interventions for new mothers, particularly to ensure adequate health care and support, could be crucial for reducing early child mortality (Akinyemi et al., 2018; Yaya et al., 2018; Amir-ud-Din et al., 2021). The exclusion of variables such as maternal education, vaginal bleeding during pregnancy, and wealth index from the final model is particularly notable. While these factors are often considered significant in other contexts, their lack of significance here suggests that, within this dataset, birth-related factors are more directly impactful on child survival outcomes than socioeconomic or maternal health variables, even after controlling for other factors. This finding challenges familiar assumptions and highlights the need for a more nuanced approach to understanding and addressing child mortality, emphasizing the role of birth characteristics as critical determinants (Yaya et al., 2018).
The ROC curve analysis provides valuable insights into the predictive ability of the final model used to assess child mortality in Indonesia, specifically focusing on birth order and birth size. The AUC values indicate the model’s capability to correctly classify child mortality outcomes, offering a metric of accuracy and discriminative power. In this study, the AUC for birth order was 0.611, indicating modest predictive ability. This finding suggests that while the birth order can distinguish between survival and mortality outcomes to some extent, its effectiveness is limited, correctly classifying outcomes approximately 61% of the time. Similarly, the child’s birth weight yielded an AUC of 0.582, indicating even lower predictive ability, with the model correctly classifying outcomes only 58% of the time.
These findings underscore a critical aspect of the model’s performance: While birth order and birth size contribute to predicting child mortality, their predictive power is relatively modest. The AUC values, which are only slightly above 0.5, suggest that these variables alone are insufficient to build a highly accurate model for predicting child mortality. The relatively moderate performance of these predictors points to the complexity of factors influencing child survival, indicating that other variables not included in the final model may play a significant role. This finding highlights the potential for enhancing the model’s accuracy by integrating additional predictors, such as maternal health indicators, socioeconomic status, access to healthcare, and environmental factors, which may provide a more comprehensive understanding of the determinants of child mortality (Lartey et al., 2016; Akinyemi et al., 2018; Warrohmah et al., 2018; Millogo et al., 2019; Balaj et al., 2021) including Indonesia. This study aims to assess the key factors associated with mortality of Indonesian infants using survival analysis. Data taken from 14,727 live-born infants (2007-2012).
The analysis also raises important considerations for public health interventions in Indonesia. The modest predictive ability of birth order and birth size suggests that risk assessments should consider these factors. While the findings suggest that birth order and size at birth are significant predictors of child mortality, relying solely on these variables may not be sufficient to accurately identify children at the highest risk of mortality. Incorporating additional factors into the predictive model could enhance its precision and improve the identification of vulnerable children needing targeted interventions. Therefore, a multifaceted approach that includes a broader range of risk factors is necessary to improve the accuracy of predictions and, consequently, the effectiveness of interventions to reduce child mortality. This approach could involve a more detailed examination of maternal and child health data and better integration of community-level factors to capture the diverse influences on child survival in Indonesia.
Overall, the study’s results suggest that health interventions in Indonesia should prioritize improving prenatal and perinatal care, explicitly managing birth outcomes, and providing targeted support to new mothers, particularly those with first or second births. While addressing socioeconomic disparities remains essential, the findings indicate that immediate improvements in child survival could be achieved by focusing on birth-related risks and ensuring that maternal and infant health are closely monitored during the critical periods before, during, and after birth. This approach could help reduce child mortality rates more effectively and contribute to broader public health goals in Indonesia.
This study has some limitations that should be considered. First, because it uses cross-sectional data, it cannot establish transparent cause-and-effect relationships, highlighting the need for future longitudinal studies. Some variables, like birth size, rely on self-reported data, which may lead to recall or reporting bias. The study focuses on selected factors, such as birth order and size, but does not include others, such as environmental conditions or maternal health, which could also influence child mortality. The findings may not apply to all regions, as they are based on data from specific populations.
Additionally, measureless factors, such as community health resources, may have influenced the results. Changes in healthcare access or socioeconomic conditions were not considered, and issues such as missing or incomplete data may have affected the study’s accuracy. Future research should address these limitations to better guide effective interventions.
Conclusion
In conclusion, this study highlights the modest predictive power of birth order and birth size in forecasting child mortality in Indonesia, as indicated by their AUC values. While these factors are essential, their limited ability to accurately predict outcomes underscores the complexity of child survival and the need for a more comprehensive model. It is crucial to integrate additional variables such as maternal health, socioeconomic status, access to healthcare, and environmental influences to improve predictions and interventions.
Public health strategies in Indonesia should prioritize enhancing prenatal and perinatal care, with a focus on managing birth outcomes and providing targeted support to mothers, particularly those with first or second births. Addressing these birth-related risks, alongside efforts to reduce socioeconomic disparities, could lead to significant improvements in child survival rates. By adopting a multifaceted approach that closely monitors maternal and infant health, Indonesia can make meaningful progress toward reducing child mortality and achieving broader public health objectives.
Ethical Considerations
Compliance with ethical guidelines
This study adhered to ethical standards by utilizing datasets from the 2017 IDHS obtained through the DHS Program before the commencement of the research. The Institutional Review Board approved the study, as documented in Authorization Letter 142047, confirming compliance with all ethical guidelines and protocols. The 2017 IDHS had already received ethical clearance from Indonesia’s National Ethics Committee. Respondents were presented with an informed consent statement in accordance with these ethical standards before participating in any interviews or biomarker tests. This statement, read aloud to each respondent, allowed them the choice to participate or decline. For minors, parental or guardian consent was required before participation. The informed consent statement provided comprehensive details about the interview/test, including its purpose, the expected duration, procedures involved, potential risks and benefits, and contact information for further inquiries. Essentially, the statement emphasized the voluntary nature of participation, allowing respondents to refuse any questions, decline any tests, or withdraw from the study at any point. It also ensured that the respondent’s identity and information would remain strictly confidential. Access to the 2017 IDHS data was granted via the DHS Program’s website.
Data availability
The datasets generated by the survey research during and or analyzed during the current study are available in the Dataverse repository.
Funding
The Directorate of Research and the Community Services University of Muhammadiyah Malang provided grant support for all phases of this study (Grant No.: E.2.a./334/BAA-UMM/IV/2022).
Authors' contributions
Conceptualization and data collection: Yoyok Bekti Prasetyo; Review and editing: Yoyok Bekti Prasetyo and Sri Sunarigsih Ika Wardojo; Writing the original draft and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors want to thank the Principal of University of Muhammadiyah Malang for their invaluable support and encouragement throughout this study.
References
Information on mortality among children under 5 years is vital for describing a country’s health status and the quality of its community’s life (Debere & Adjiwanou, 2024; Hossain et al., 2024). At the same time, the mortality of children under 5 years is a crucial measure of a country’s socioeconomic and demographic progress and quality of life (QoL), particularly in families (Wahl et al., 2023). Lack of competent human resources, poor infrastructure, and underinvestment in health systems have dramatically raised child mortality rates in low- and middle-income countries (Dauda et al., 2024; Mekonnen et al., 2024a)urban areas generally have better access to and use of maternal, newborn, and child health (MNCH).
Child mortality is still a crucial global issue, particularly in Indonesia. The mortality rate for children under 5 years of age declined by 49%, from 77 deaths per 1000 live births in 2000 to 39 deaths in 2017, or 1 in every 14 children dying in 2017 (WHO, 2019). Indonesia has been attempting to reduce child mortality each year, and the rate is decreasing. The 2017 Indonesia demographic and health survey (IDHS) statistics show a neonatal mortality rate (NMR) of 15 per 1000 live births, an infant mortality rate of 24 per 1000 live births, and a toddler mortality rate of 32 per 1000 live births (Ministry of Health Indonesia, 2019; Statista, 2021). Of course, this figure remains far from the sustainable development goals (SDGs), which set a target of 12 per 1000 live births for child mortality (WHO, 2015).
In 2019, low birth weight (Wulandari et al., 2022) was the leading cause of infant death in Indonesia. Other reasons for death were hypoxia, congenital disabilities, infection, and newborn tetanus (Soleman, 2020). In Indonesia, the factors influencing child mortality include maternal age at birth, birth spacing, and the child’s weight at birth. A child’s birth weight affects their nutritional health and immunological system (Soleman, 2020). Indonesia’s national policy for children’s health states that every child has the right to survive, grow, and develop, as well as the right to be protected from violence and discrimination, underscoring the need for integrated, comprehensive, and sustainable child health initiatives (Kemenkes, 2022). Child health efforts in Indonesia include prenatal care, newborn and infant health, toddler and preschooler health, school-age child and adolescent health, and child health protection (Kemenkes, 2022). However, Indonesia strives to reduce the mortality rate of children under 5 by the SDGs target by 2030.
This research introduces a novel approach, employing receiver operating characteristic (ROC) curve analysis to assess and compare the predictive accuracy of various models for identifying key factors contributing to child mortality in Indonesia. Unlike previous studies that have examined the determinants of child mortality, this research distinguishes itself by focusing on ROC curves—a method not commonly used in public health research in this context. By integrating ROC analysis, the study offers a more robust and comprehensive evaluation of predictive models, highlighting their sensitivity, specificity, and accuracy. Furthermore, the research provides context-specific insights by addressing Indonesia’s unique socioeconomic, cultural, and healthcare-related factors, ensuring that the findings are highly relevant to local policymakers and healthcare providers.
Despite extensive global research on child mortality, significant gaps remain, particularly within the Indonesian context. One such gap is the limited application of ROC analysis in public health research on child mortality in Indonesia, which this study addresses by offering a nuanced understanding of the predictive power of various factors. Additionally, while much of the existing literature relies on generalized models, this research focuses on Indonesia-specific data, providing insights more applicable to the local context. The study also bridges the gap in integrating multiple predictors by simultaneously evaluating them through ROC analysis, enabling a more comprehensive understanding of their collective impact. Finally, by systematically comparing predictive models, the research addresses the lack of comparative analysis in existing studies and ultimately identifies the most effective strategies for reducing child mortality in Indonesia.
The theoretical foundation of this study is rooted in the determinants of child mortality, which encompass demographic, socioeconomic, biological, and healthcare-related factors. The conceptual model integrates key elements from public health and epidemiological theories, including the life-course perspective and the social determinants of health framework. These frameworks emphasize the interplay of maternal, neonatal, and environmental factors in shaping child survival outcomes. Maternal education, socioeconomic status, and access to healthcare are critical predictors that influence child health and mortality (Ogunniyi et al., 2024; Zhang et al., 2024). These elements provide a structured approach to understanding the multifaceted nature of child mortality, aligning with global health theories on inequality, resource access, and health system efficiency.
The conceptual framework of this research introduces ROC analysis as a novel method to evaluate predictive models of child mortality. ROC analysis is a tool for assessing the accuracy of predictors such as birth size and birth order by quantifying their sensitivity and specificity (Obuchowski & Bullen, 2018). This approach integrates predictive analytics into public health research, offering a deeper understanding of how individual factors contribute to child mortality risk. The framework emphasizes the relative predictive power of birth characteristics by comparing the area under the curve (AUC) values of different predictors. It situates them within a broader context of healthcare disparities and maternal health factors. This methodology provides a structured means to evaluate the effectiveness of targeted interventions to reduce child mortality.
The framework also incorporates Indonesia’s unique socioeconomic and cultural context, recognizing the influence of maternal health practices, birth traditions, and healthcare accessibility on child mortality. This perspective aligns with Bronfenbrenner’s ecological systems theory, highlighting the interaction between individual and environmental factors (Ogunniyi et al., 2024). The study acknowledges that child mortality in Indonesia is not only influenced by biological determinants but also by external factors such as maternal age, birth spacing, healthcare infrastructure, and cultural norms. These elements underscore the importance of a holistic approach that integrates individual-level and systemic-level predictors into a cohesive model, ensuring the findings are contextually relevant to Indonesian healthcare policies.
This study’s framework bridges critical gaps in child mortality research by emphasizing the application of advanced predictive analytics and context-specific data. Unlike traditional models, which often focus on singular or generalized predictors, this framework evaluates multiple determinants simultaneously to capture their collective impact. The innovative use of ROC analysis offers a more nuanced understanding of the predictive power of factors such as birth size and birth order, which are often underexplored in the public health literature. Furthermore, integrating Indonesia-specific data addresses the limited applicability of global models to local contexts, enhancing the study’s relevance and utility for policymakers. By aligning theoretical insights with practical applications, the framework aims to contribute to effective, evidence-based interventions to reduce child mortality in Indonesia. In this study, we analysed predictors of child mortality using secondary data from the 2017 IDHS and evaluated the predictive ability of birth size and birth order through ROC analysis.
Materials and Methods
Study design
The cross-sectional design allows for examining data collected at a single point in time, providing a snapshot of the factors associated with child mortality in Indonesia. This approach is well-suited for identifying potential predictors and assessing their relationship with child mortality, using secondary data from the 2017 IDHS.
Sample and data collection
This study used secondary data from the 2017 IDHS. The IDHS utilized standardized questionnaires developed by the demographic and health surveys (DHS) program, including the household questionnaire, the women’s questionnaire, and the child health questionnaire. These instruments were adapted to the Indonesian context and pretested to ensure cultural relevance. The validity and reliability of the IDHS instruments are well established internationally, as they undergo rigorous methodological development and field testing. In Indonesia, the Ministry of Health conducted the survey in collaboration with the National Population and Family Planning Board and the Central Statistics Agency, ensuring high-quality, nationally representative data.
The study’s population consisted of women aged 15-49, from whom data were collected using a multistage stratified random sampling technique. In the first stage, several census blocks (enumeration areas) were randomly selected from each stratum using probability proportional to size. In the second stage, 25 households were randomly selected from each chosen census block. This method ensures that the sample is nationally representative and covers various geographic and social groups nationwide.
The total initial sample comprised 17848 respondents. Data were collected by a team of 1160 trained personnel who administered the survey and ensured data quality. The survey collected detailed information on various factors, including socioeconomic status, healthcare access, maternal and child health indicators, and more. A thorough data-cleaning process was conducted to ensure the integrity of the analysis. Incomplete responses and unanswered questions from respondents were carefully removed from the dataset. After this process, a final sample of 13946 respondents was obtained, which served as the core dataset for analysis in this study.
Study variables
The study investigated a range of independent variables to assess their impact on child mortality in Indonesia. These variables encompassed the child’s age, gender, place of residence, parental education, and issues such as vaginal bleeding during pregnancy. Factors such as the child’s birth weight, antenatal care, and the mother’s knowledge of danger signs during pregnancy were examined. The study classified children’s ages into 0-24 months (coded 0) and 25-59 months (coded 1). Gender was recorded as male (coded 1) or female (coded 2), while residence was categorized as urban (coded 1) or rural (coded 2). Maternal education was divided into four levels: No schooling (coded 0), primary (coded 1), secondary (coded 2), and higher education (coded 3). Vaginal bleeding during pregnancy was noted as either “yes” or “no,” and the child’s size at birth was categorized into 6 groups ranging from very large (coded 1) to unknown size (coded 8).
Further variables included antenatal care (no [coded 0] or yes [coded 1]) and the mother’s knowledge of danger signs during pregnancy (no [coded 0] or yes [coded 1]). Economic status was divided into 5 categories: Poorest (coded 1), poorer (coded 2), middle (coded 3), richer (coded 4), and richest (coded 5). The number of births was categorized into three groups: 1-2 births (coded 0), 3-5 births (coded 1), and 6-13 births (coded 2). The timing of the child’s initial access to the mother’s nipple was dichotomized into immediate (coded 0) or delayed (coded 1). The dependent variable was the child’s survival status, with survival coded as 1 (yes) and non-survival as 0 (no).
Data analysis
Categorical variables were summarized using frequency distributions and percentages to analyze predictors of child mortality in Indonesia, providing a clear overview of their prevalence and distribution. Relationships between predictors and child mortality were examined using cross-tabulation and chi-square tests. significant predictors were identified through multivariable logistic regression, with a P value threshold of <0.05, and non-significant variables were excluded using backward elimination. The final model’s predictive performance was evaluated using an ROC curve, which plots sensitivity versus specificity to assess accuracy and discriminative ability, providing insights into the model’s effectiveness in predicting child mortality.
Results
Respondents’ characteristics
Table 1 outlines the characteristics of the respondents (n=13946) and offers valuable insights into factors related to child mortality in Indonesia. The data reveal that a majority of the children were aged 25-59 months (53.4%), with a near-equal distribution between male (51.2%) and female (48.9%) children. The respondents’ residence was almost evenly split between urban (49.8%) and rural (50.2%) areas. Educational attainment of the mothers varied, with a majority having secondary education (56.2%), while only a tiny fraction had no formal education (1.2%). Additionally, issues such as vaginal bleeding during pregnancy were reported by 45.3% of respondents, and a significant portion (54.7%) did not experience this complication.
Further data analysis shows that most children were of average size at birth (53.6%), with a notable proportion classified as larger than average (27.5%). Antenatal care was significantly underutilized, with 85.4% of respondents reporting no such care. Knowledge of danger signs during pregnancy was more prevalent, with 65.7% of mothers aware of them. Economic status was diverse, with the wealth index ranging from the poorest (25.6%) to the richest (17.3%). Birth order data indicate that most children were first- or second-born (64.2%), and the timing of initial breastfeeding shows that 57.6% were breastfed immediately after birth. The survival status of children was overwhelmingly positive, with 99.2% reported to be alive. This study only included one child per mother to clarify the analysis and avoid confusion. We chose the last-born child under 5 because the 2017 IDHS collects the most complete and detailed information on the most recent child, including health, nutrition, and survival. Using the last-born child also helps reduce errors since mothers usually remember recent events better than older ones. These findings underscore the diverse demographic, socioeconomic, and health-related factors that contribute to child mortality, providing a foundation for targeted interventions and further research (Table 1).
Predictors of child mortality
Table 2 outlines the bivariate analysis and cross-tabulation of the outcome variable against various covariates from the 2017 IDHS dataset, revealing important insights into factors influencing child mortality. The child’s age showed no significant association with mortality; both age groups (0-24 months and 25-59 months) had similar odds ratios (OR=0.94; 95% CI, 0.65%, 1.36%; P=0.755). Similarly, the sex of the child did not appear to influence survival outcomes, as the odds of mortality for male children were not significantly different from those of female children (OR=1.162; 95% CI, 0.80%, 1.68%; P=0.428). However, the place of residence presented a near-significant association, with children in urban areas showing a trend toward lower mortality odds than those in rural areas (OR=0.690; 95% CI, 0.47%, 1%; P=0.052).
Maternal education level emerged as a significant predictor of child mortality. Children born to mothers with no education had significantly higher odds of mortality compared to those whose mothers had higher education (OR=3.750; 95% CI, 1.23%, 11.34%; P<0.001). Additionally, primary education was associated with increased odds of mortality (OR =1.979; 95% CI, 1.11%, 3.51%). Vaginal bleeding during pregnancy also showed a significant association, with children whose mothers experienced this complication having higher odds of mortality compared to those without such issues (OR=1.580; 95% CI, 1.07%, 2.33%; P=0.020).
The size of the child at birth was another critical factor, with very large, larger-than-average, and average-sized children all demonstrating significantly lower odds of mortality compared to tiny children. Specifically, very large children had the lowest odds (OR=0.130; 95% CI, 0.03%, 0.44%; P<0.001). The wealth index also indicated economic disparities in child survival, with children from the poorest households showing significantly higher odds of mortality than those from the richest households (OR=1.919; 95% CI, 1.10%, 3.34%; P=0.001). Lastly, birth order was a strong predictor, with first and second-born children showing significantly higher odds of mortality than those who were sixth to thirteenth in Birth order (OR=0.168; 95% CI, 0.09%, 0.30%; P<0.001). These findings underscore the importance of socioeconomic factors, maternal health, and birth characteristics in determining child survival in Indonesia.
Model of child mortality
The multivariate analysis of child mortality using the 2017 IDHS data highlights the significant influence of birth size and birth order on child survival. The size of the child at birth emerged as a critical predictor, with very large, larger-than-average, and average-sized children exhibiting significantly higher odds of mortality compared to very small children. Specifically, very large children had an odds ratio of 5.964 (95% CI, 1.698%, 20.942%; P=0.005), while larger-than-average and average-sized children had ORs of 5.554 (95% CI, 2.284%, 13.506%; P<0.001) and 3.922 (95% CI, 1.719%, 8.949%; P=0.001), respectively. Even children who were smaller than average had a higher risk of mortality, with an OR of 2.887 (95% CI, 1.155%, 7.214%; P=0.023) when compared to very small children who served as the reference group. These findings suggest that extremes in birth size, particularly very large sizes, are associated with a higher risk of mortality, underscoring the importance of monitoring and managing birth outcomes (Table 3).
Birth order also played a significant role in determining child survival. Children who were first or second-born had significantly higher odds of mortality (OR=5.209; 95% CI, 2.861%, 9.483%; P<0.001) compared to those who were sixth to thirteenth in birth order. Similarly, third to fifth-born children also faced increased mortality risk, with an OR of 2.836 (95% CI, 1.552%, 5.184%; P=0.001). This pattern indicates that lower birth order is associated with higher mortality, potentially due to resource allocation, maternal health, or caregiving capacity. Notably, education level, pregnancy-related issues such as vaginal bleeding, and wealth index were excluded from the final model because their P values exceeded 0.05, suggesting that these factors were not significant predictors of child mortality after controlling for other variables. This result emphasizes the critical impact of birth characteristics over socioeconomic and maternal health factors in this context (Table 3).
The ROC curve was used to evaluate the predictive ability of the final model for child mortality in Indonesia, focusing on two key predictors: birth weight and birth order. The AUC measures the model’s accuracy, with higher values indicating better discriminative power. In this study, the AUC for birth order was 0.611, suggesting that this variable has modest predictive ability, correctly classifying child mortality outcomes approximately 61% of the time. On the other hand, the child’s birth weight had an AUC of 0.582, indicating slightly lower predictive ability, with the model correctly classifying outcomes about 58% of the time (Figure 1).
These AUC values reflect the model’s overall performance in predicting child mortality based on these two variables. Although both predictors demonstrate some ability to distinguish between children who survive and those who do not, the relatively moderate AUC values suggest room for improvement in the model’s predictive power. Birth order appears to be a slightly stronger predictor than the child’s birth size, but neither alone is highly accurate. These findings highlight the need to consider additional factors or refine the model further to enhance its ability to predict child mortality more precisely in the Indonesian context.
Discussion
Characteristics of the respondents
The findings from the respondents’ characteristics in Table 1 provide a detailed view of the factors influencing child mortality in Indonesia. The near-equal distribution of male and female children and the balanced urban and rural residency suggest that gender and location might not be significant determinants of child mortality on their own. However, these variables should still be considered in a broader analysis that includes other socioeconomic and health-related factors (Amegbor & Addae, 2023; Ahmed & Atiqul Haq, 2024; Hossain et al., 2024).
Mothers’ educational attainment emerged as a critical factor, with the majority having secondary education. This finding suggests that education is vital to child health outcomes, potentially affecting mothers’ ability to access healthcare, understand health risks, and make informed decisions about their children’s wellbeing (Khani Jeihooni et al., 2022; Nishad & Sinha, 2023; Zhang et al., 2024). The presence of pregnancy complications, such as vaginal bleeding, reported by 45.3% of respondents, is another significant concern, highlighting the need for improved maternal healthcare services, especially during pregnancy (Seid et al., 2023; Girchenko et al., 2024).
The data on antenatal care utilization reveal a glaring gap: 85.4% of respondents reported no antenatal care. This underutilization is alarming and points to potential barriers to accessing healthcare services, which could contribute to higher risks of child mortality. Additionally, knowledge of danger signs during pregnancy, although relatively high at 65.7%, indicates that a significant portion of the population still lacks critical awareness, which could delay seeking care and lead to adverse outcomes (Pai et al., 2023; Tiruye & Shiferaw, 2023).
The economic disparities reflected in the wealth index suggest that child mortality risk may vary across socioeconomic groups, with the poorest potentially more vulnerable (Hossain et al., 2024). The timing of initial breastfeeding and the survival status of children further reinforce the importance of immediate postnatal care and interventions (Rosenberg et al., 2024). Overall, these results emphasize the need for targeted public health interventions that address education, access to maternal and child healthcare, and socioeconomic inequalities to reduce child mortality in Indonesia.
Predictors of child mortality
The bivariate analysis and cross-tabulation of factors influencing child mortality in Indonesia provide significant insights into the complex interplay of demographic, socioeconomic, and health-related variables. One of the most striking findings is the non-significant association between child mortality and variables like the age and sex of the child. This finding suggests that, in this context, survival outcomes are not predominantly determined by these demographic factors but rather by other underlying conditions. However, the near-significant association between urban residence and lower mortality odds highlights the potential influence of environmental factors, such as access to healthcare, sanitation, and other public health resources, which are often more readily available in urban settings (Girma et al., 2023; Khan et al., 2023).
Maternal education level stands out as a critical predictor of child survival, with the data clearly showing that children born to mothers with no formal education face significantly higher mortality risks. This finding underscores the pivotal role of maternal education in enhancing child health outcomes, likely due to better health literacy, improved utilization of healthcare services, and greater awareness of child-rearing practices (Oyekale & Maselwa, 2018; Yaya et al., 2019; Ifada et al., 2020; Balaj et al., 2021). The strong association between maternal education and child survival suggests that public health interventions to improve women's educational opportunities could substantially reduce child mortality in Indonesia (Yaya et al., 2018; Zhang et al., 2024).
The analysis also highlights the importance of maternal health during pregnancy, as evidenced by the significant association between vaginal bleeding and increased child mortality. This finding emphasizes the need for enhanced prenatal care and monitoring, especially for high-risk pregnancies, to mitigate complications that could lead to adverse outcomes (Combellick et al., 2024; Mekonnen et al., 2024b). Additionally, the size of the child at birth and the birth order emerged as strong predictors of survival, with large children and those born early in birth order facing higher mortality risks. These findings highlight the importance of targeted interventions, such as improved maternal nutrition and family planning, to address these risk factors (Bango & Ghosh, 2023; Masquelier et al., 2023; Debere & Adjiwanou, 2024).
Economic disparities, as reflected in the wealth index, further complicate the picture of child mortality in Indonesia (Amini Rarani et al., 2018; Yaya et al., 2020). The higher odds of mortality among children from the poorest households compared to those from wealthier backgrounds suggest that socioeconomic inequalities play a crucial role in child survival (Amini Rarani et al., 2018; Balaj et al., 2021). This finding highlights the need for policies and programs that address these disparities by improving access to healthcare, nutrition, and other essential services for the most vulnerable populations. The research underscores the multifaceted nature of child mortality in Indonesia, driven by socioeconomic, health, and demographic factors. Addressing these issues through comprehensive public health strategies will be essential in reducing child mortality and improving overall child health outcomes in the country (Garcia et al., 2023; Ghazy et al., 2024).
Model of child mortality
The multivariate analysis of child mortality from the 2017 IDHS offers critical insights into the factors significantly influencing child survival in Indonesia. The analysis reveals that birth size is a crucial determinant of mortality risk, with both very large and larger-than-average sizes associated with significantly higher odds of mortality compared to very small children (Kim et al., 2022). Interestingly, while small size is often considered a risk factor, this analysis indicates that the extremes in birth size, particularly large or larger than average, pose an even greater risk. These findings may reflect complications associated with delivery or underlying health conditions in larger infants, necessitating careful monitoring and medical intervention (Memiah et al., 2020) infant, and child deaths occur in low- and middle-income countries (LMICs. The strong association between birth size and mortality underscores the importance of prenatal care focused on monitoring fetal growth and ensuring appropriate measures are taken during delivery to manage potential complications (Yaya et al., 2020; Chang et al., 2021) the NMR.
Birth order also emerged as a significant predictor of child mortality, with first and second-born children facing notably higher risks compared to those born later in the birth sequence. This pattern might be explained by parental inexperience, less developed maternal health during first births, or higher stress and resource strain in larger families that could disadvantage early-born children. However, the finding that first- and second-born children are at higher risk suggests that targeted interventions for new mothers, particularly to ensure adequate health care and support, could be crucial for reducing early child mortality (Akinyemi et al., 2018; Yaya et al., 2018; Amir-ud-Din et al., 2021). The exclusion of variables such as maternal education, vaginal bleeding during pregnancy, and wealth index from the final model is particularly notable. While these factors are often considered significant in other contexts, their lack of significance here suggests that, within this dataset, birth-related factors are more directly impactful on child survival outcomes than socioeconomic or maternal health variables, even after controlling for other factors. This finding challenges familiar assumptions and highlights the need for a more nuanced approach to understanding and addressing child mortality, emphasizing the role of birth characteristics as critical determinants (Yaya et al., 2018).
The ROC curve analysis provides valuable insights into the predictive ability of the final model used to assess child mortality in Indonesia, specifically focusing on birth order and birth size. The AUC values indicate the model’s capability to correctly classify child mortality outcomes, offering a metric of accuracy and discriminative power. In this study, the AUC for birth order was 0.611, indicating modest predictive ability. This finding suggests that while the birth order can distinguish between survival and mortality outcomes to some extent, its effectiveness is limited, correctly classifying outcomes approximately 61% of the time. Similarly, the child’s birth weight yielded an AUC of 0.582, indicating even lower predictive ability, with the model correctly classifying outcomes only 58% of the time.
These findings underscore a critical aspect of the model’s performance: While birth order and birth size contribute to predicting child mortality, their predictive power is relatively modest. The AUC values, which are only slightly above 0.5, suggest that these variables alone are insufficient to build a highly accurate model for predicting child mortality. The relatively moderate performance of these predictors points to the complexity of factors influencing child survival, indicating that other variables not included in the final model may play a significant role. This finding highlights the potential for enhancing the model’s accuracy by integrating additional predictors, such as maternal health indicators, socioeconomic status, access to healthcare, and environmental factors, which may provide a more comprehensive understanding of the determinants of child mortality (Lartey et al., 2016; Akinyemi et al., 2018; Warrohmah et al., 2018; Millogo et al., 2019; Balaj et al., 2021) including Indonesia. This study aims to assess the key factors associated with mortality of Indonesian infants using survival analysis. Data taken from 14,727 live-born infants (2007-2012).
The analysis also raises important considerations for public health interventions in Indonesia. The modest predictive ability of birth order and birth size suggests that risk assessments should consider these factors. While the findings suggest that birth order and size at birth are significant predictors of child mortality, relying solely on these variables may not be sufficient to accurately identify children at the highest risk of mortality. Incorporating additional factors into the predictive model could enhance its precision and improve the identification of vulnerable children needing targeted interventions. Therefore, a multifaceted approach that includes a broader range of risk factors is necessary to improve the accuracy of predictions and, consequently, the effectiveness of interventions to reduce child mortality. This approach could involve a more detailed examination of maternal and child health data and better integration of community-level factors to capture the diverse influences on child survival in Indonesia.
Overall, the study’s results suggest that health interventions in Indonesia should prioritize improving prenatal and perinatal care, explicitly managing birth outcomes, and providing targeted support to new mothers, particularly those with first or second births. While addressing socioeconomic disparities remains essential, the findings indicate that immediate improvements in child survival could be achieved by focusing on birth-related risks and ensuring that maternal and infant health are closely monitored during the critical periods before, during, and after birth. This approach could help reduce child mortality rates more effectively and contribute to broader public health goals in Indonesia.
This study has some limitations that should be considered. First, because it uses cross-sectional data, it cannot establish transparent cause-and-effect relationships, highlighting the need for future longitudinal studies. Some variables, like birth size, rely on self-reported data, which may lead to recall or reporting bias. The study focuses on selected factors, such as birth order and size, but does not include others, such as environmental conditions or maternal health, which could also influence child mortality. The findings may not apply to all regions, as they are based on data from specific populations.
Additionally, measureless factors, such as community health resources, may have influenced the results. Changes in healthcare access or socioeconomic conditions were not considered, and issues such as missing or incomplete data may have affected the study’s accuracy. Future research should address these limitations to better guide effective interventions.
Conclusion
In conclusion, this study highlights the modest predictive power of birth order and birth size in forecasting child mortality in Indonesia, as indicated by their AUC values. While these factors are essential, their limited ability to accurately predict outcomes underscores the complexity of child survival and the need for a more comprehensive model. It is crucial to integrate additional variables such as maternal health, socioeconomic status, access to healthcare, and environmental influences to improve predictions and interventions.
Public health strategies in Indonesia should prioritize enhancing prenatal and perinatal care, with a focus on managing birth outcomes and providing targeted support to mothers, particularly those with first or second births. Addressing these birth-related risks, alongside efforts to reduce socioeconomic disparities, could lead to significant improvements in child survival rates. By adopting a multifaceted approach that closely monitors maternal and infant health, Indonesia can make meaningful progress toward reducing child mortality and achieving broader public health objectives.
Ethical Considerations
Compliance with ethical guidelines
This study adhered to ethical standards by utilizing datasets from the 2017 IDHS obtained through the DHS Program before the commencement of the research. The Institutional Review Board approved the study, as documented in Authorization Letter 142047, confirming compliance with all ethical guidelines and protocols. The 2017 IDHS had already received ethical clearance from Indonesia’s National Ethics Committee. Respondents were presented with an informed consent statement in accordance with these ethical standards before participating in any interviews or biomarker tests. This statement, read aloud to each respondent, allowed them the choice to participate or decline. For minors, parental or guardian consent was required before participation. The informed consent statement provided comprehensive details about the interview/test, including its purpose, the expected duration, procedures involved, potential risks and benefits, and contact information for further inquiries. Essentially, the statement emphasized the voluntary nature of participation, allowing respondents to refuse any questions, decline any tests, or withdraw from the study at any point. It also ensured that the respondent’s identity and information would remain strictly confidential. Access to the 2017 IDHS data was granted via the DHS Program’s website.
Data availability
The datasets generated by the survey research during and or analyzed during the current study are available in the Dataverse repository.
Funding
The Directorate of Research and the Community Services University of Muhammadiyah Malang provided grant support for all phases of this study (Grant No.: E.2.a./334/BAA-UMM/IV/2022).
Authors' contributions
Conceptualization and data collection: Yoyok Bekti Prasetyo; Review and editing: Yoyok Bekti Prasetyo and Sri Sunarigsih Ika Wardojo; Writing the original draft and final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors want to thank the Principal of University of Muhammadiyah Malang for their invaluable support and encouragement throughout this study.
References
Ahmed, K. J. & Atiqul Haq, S. M., 2024. Perceived risk of child mortality and fertility choices in climate-vulnerable regions of Bangladesh. Humanities and Social Sciences Communications, 11(1), pp. 147. [DOI:10.1057/s41599-024-02640-2]
Akinyemi, J. O., Bolajoko, I. & Gbadebo, B. M., 2018. ‘Death of preceding child and maternal healthcare services utilisation in Nigeria: Investigation using lagged logit models’, Journal of Health, Population and Nutrition. Journal of Health, Population and Nutrition, 37(1), pp. 1-12. [DOI:10.1186/s41043-018-0154-0]
Amegbor, P. M. & Addae, A., 2023. Spatiotemporal analysis of the effect of global development indicators on child mortality. International Journal of Health Geographics, 22(1), pp. 9. [DOI:10.1186/s12942-023-00330-x] [PMID]
Amini Rarani, M., et al., 2018. Measuring Socioeconomic Inequality Changes in Child Mortality in Iran: Two National Surveys Inequality Analysis. Iranian Journal of Public Health, 47(9), pp. 1379–87. [PMID]
Amir-ud-Din, R., et al., 2021. Impact of high-risk fertility behaviours on underfive mortality in Asia and Africa: Evidence from Demographic and Health Surveys. BMC Pregnancy and Childbirth, 21(1), pp. 344. [DOI:10.1186/s12884-021-03780-y]
Balaj, M., et al., 2021. Parental education and inequalities in child mortality: A global systematic review and meta-analysis. Lancet, 398(10300), pp. 608-20. [DOI:10.1016/S0140-6736(21)00534-1] [PMID]
Bango, M. & Ghosh, S., 2023. Reducing infant and child mortality: assessing the social inclusiveness of child health care policies and programmes in three states of India. BMC Public Health, 23(1), pp. 1149. [DOI:10.1186/s12889-023-15812-7] [PMID]
Chang, Y. S., et al., 2021. ‘Neonatal and infant mortality of very-low-birth-weight infants in Taiwan: Does the level of delivery hospital matter? Pediatrics and Neonatology. Elsevier Taiwan LLC, 62(4), pp. 419-27. [DOI:10.1016/j.pedneo.2021.04.003] [PMID]
Combellick, J. L., et al., 2024. Perinatal mental health and pregnancy-associated mortality: Opportunities for change.Archives of Women’s Mental Health, 27(3), pp. 417-24. [DOI:10.1007/s00737-023-01404-2]
Dauda, R. S., Adeniji, P. O. & Onatunji, O. G., 2024. Exploring the Determinants of Child Mortality in Nigeria: Insights from Multiple Econometric Techniques. Child Indicators Research, 17(5), pp. 2243-60. [DOI:10.1007/s12187-024-10159-w]
Debere, H. R. & Adjiwanou, V., 2024. The effects of reproductive variables on child mortality in Ethiopia: Evidence from demographic and health surveys from 2000 to 2016. Reproductive Health, 21(1), p. 4. [DOI:10.1186/s12978-023-01734-5] [PMID]
Garcia, L. P. et al., 2023. What is the impact of national public expenditure and its allocation on neonatal and child mortality? A machine learning analysis. BMC Public Health, 23(1), pp. 793. [DOI:10.1186/s12889-023-15683-y] [PMID]
Ghazy, R. M., Saidouni, A. & Taha, S. H. N., 2024. Promoting child health through a comprehensive One Health perspective: A narrative review. Egyptian Pediatric Association Gazette, 72(1), pp. 3. [DOI:10.1186/s43054-023-00243-1]
Girchenko, P., et al., 2024. Associations of polymetabolic risk of high maternal pre-pregnancy body mass index with pregnancy complications, birth outcomes, and early childhood neurodevelopment: findings from two pregnancy cohorts. BMC Pregnancy and Childbirth, 24(1), pp. 78. [DOI:10.1186/s12884-024-06274-9] [PMID]
Girma, M., et al., 2023. ‘Socio-demographic and environmental determinants of under-five child mortality in Ethiopia: using Ethiopian demographic and Health 2019 survey. BMC Pediatrics, 23(1), pp. 294. [DOI:10.1186/s12887-023-04026-w] [PMID]
Statista., 2021. Under-five child mortality rate in Indonesia 2009-2019. Retrieved from: [Link]
Hossain, S. et al., 2024. Socioeconomic factors affecting child mortality in hill tracts of chattogram division, Bangladesh. GeoJournal, 89(2), pp. 73. [DOI:10.1007/s10708-024-11082-x]
Ifada, L., Nurmalasari, M. & Pramana, S., 2020. Multilevel survival analysis for under-fives in Indonesia 2015. Paediatrica Indonesiana, 60(2), pp. 101-8. [DOI:10.14238/pi60.2.2020.101-8]
Kemenkes, R. I., 2022. Indonesia Health Profile 2021, Pusdatin. Jakarta: Kementerian Kesehatan Republik Indonesia. [Link]
Khan, G. R., Baten, A. & Azad, M. A. K., 2023. ‘Influence of contraceptive use and other socio-demographic factors on under-five child mortality in Bangladesh: Semi-parametric and parametric approaches. Contraception and Reproductive Medicine, 8(1), pp. 22. [DOI:10.1186/s40834-023-00217-z] [PMID]
Khani Jeihooni, A. et al., 2022. Effect of educational intervention based on health belief model on mothers monitoring growth of 6-12 months child with growth disorders. BMC Pediatrics, 22(1), pp. 561. [DOI:10.1186/s12887-022-03593-8] [PMID]
Kim, Y. S. et al., 2022. Child mortality of twins and singletons among late preterm and term birth: a study of national linked birth and under-five mortality data of Korea. European Journal of Pediatrics, 181(5), pp. 2109-16. [DOI:10.1007/s00431-022-04410-1] [PMID]
Lartey, S. T., Khanam, R. & Takahashi, S., 2016. ‘The impact of household wealth on child survival in Ghana. Journal of Health, Population and Nutrition, 35(1), pp. 38. [DOI:10.1186/s41043-016-0074-9] [PMID]
Masquelier, B., Menashe-Oren, A. & Reniers, G., 2023. An evaluation of truncated birth histories for the rapid measurement of fertility and child survival. Population Health Metrics, 21(1), pp. 8. [DOI:10.1186/s12963-023-00307-9]
Mekonnen, W., et al., 2024a. Inter-district and Wealth-related Inequalities in Maternal and Child Health Service Coverage and Child Mortality within Addis Ababa City. Journal of Urban Health, 101(S1), pp. 68-80. [DOI:10.1007/s11524-024-00836-0]
Mekonnen, W. et al., 2024b. Inter-district and Wealth-related Inequalities in Maternal and Child Health Service Coverage and Child Mortality within Addis Ababa City. Journal of Urban Health. [DOI:10.1007/s11524-024-00836-0] [PMID]
Memiah, P. et al., 2020. Neonatal, infant, and child mortality among women exposed to intimate partner violence in East Africa: A multi-country analysis. BMC Women’s Health. BMC Women’s Health, 20(1), pp. 1-16. [DOI:10.1186/s12905-019-0867-2] [PMID]
Millogo, O. et al., 2019. Geographical variation in the association of child, maternal and household health interventions with under-five mortality in Burkina Faso. Plos One, 14(7), pp. 1-17. [DOI:10.1371/journal.pone.0218163] [PMID]
Ministry of Health Indonesia., 2019. Indonesia Health Profile 2018. Jakarta: Ministry of Health Indonesia. [Link]
Nishad, P. & Sinha, B. R. K., 2023. Role of educational attainment of mothers in child delivery, post natal check-up, and child immunization in urban India: A study in the context of child health. In Urban dynamics, environment and health (pp. 531-546). Singapore: Springer Nature Singapore. [DOI:10.1007/978-981-99-5744-6_24]
Obuchowski, N. A. & Bullen, J. A., 2018. Receiver operating characteristic (ROC) curves: review of methods with applications in diagnostic medicine. Physics in Medicine and Biology, 29, 63(7), pp. 07TR01. [DOI:10.1088/1361-6560/aab4b1] [PMID]
Ogunniyi, A. I., et al., 2024. Evaluating the Role of Households’ Food Security Status and Socioeconomic Determinants on Child Mortality in Nigeria. Child Indicators Research, 17(4), pp. 1687-714. [DOI:10.1007/s12187-024-10134-5]
Oyekale, A. S. & Maselwa, T. C., 2018. Maternal education, fertility, and child survival in comoros. International Journal of Environmental Research and Public Health, 15(12). [DOI:10.3390/ijerph15122814] [PMID]
Pai, H., et al., 2023. Pre-Conceptional and Antenatal Care for Improved Newborn and Child Survival in India: A Review. Indian Journal of Pediatrics, 90(S1), pp. 10-19. [DOI:10.1007/s12098-023-04841-0]
Rosenberg, J., Nardella, D. & Shabanova, V., 2024. State paid family leave policies and breastfeeding duration: cross-sectional analysis of 2021 national immunization survey-child. International Breastfeeding Journal, 19(1), pp. 37. [DOI:10.1186/s13006-024-00646-9] [PMID]
Seid, A. K. et al., 2023. Pregnancy complications in last pregnancy and mothers’ long-term cardiovascular mortality: Does the relation differ from that of complications in first pregnancy? A population-based study. BMC Women’s Health, 23(1), pp. 355. [DOI:10.1186/s12905-023-02503-z] [PMID]
Soleman, S. R., 2020. The Trend of Children Mortality Rates in Indonesia. Jurnal Ilmu Kesehatan Masyarakat, 11(01), pp. 52-62. [DOI:10.26553/jikm.2020.11.1.52-62]
Tiruye, G. & Shiferaw, K., 2023. Antenatal Care Reduces Neonatal Mortality in Ethiopia: A systematic review and meta-analysis of observational studies. Maternal and Child Health Journal, 27(12), pp. 2064-76. [DOI:10.1007/s10995-023-03765-7]
Wahl, B., et al., 2023. Neonatal, Infant, and Child Mortality in India: Progress and Future Directions. Indian Journal of Pediatrics, 90(S1), pp. 1-9. [DOI:10.1007/s12098-023-04834-z] [PMID]
Warrohmah, A. N. I., et al., 2018. Analysis of the Survival of Children Under Five in Indonesia and Associated Factors. IOP Conference Series: Earth and Environmental Science, 116(1), pp. 012014. [DOI:10.1088/1755-1315/116/1/012014]
World Health Organization., 2015. Health in 2015 from MDGs to SDGs. Geneva: World Health Organization. [Link]
World Health Organization., 2019. World health statistics 2019 monitoring health for the SDGs. Geneva: World Health Organization. [Link]
Wulandari, F. et al., 2022. Maternal Characteristics and Socioeconomic Factors as Determinants of Low Birth Weight in Indonesia: Analysis of 2017 Indonesian Demographic and Health Survey (IDHS). International Journal of Environmental Research and Public Health, 19(21), pp. 13892. [DOI:10.3390/ijerph192113892] [PMID]
Yaya, S. et al., 2018. Under five mortality patterns and associated maternal risk factors in sub-Saharan Africa: A multi-country analysis. Plos One, 13(10), pp. e0205977. [DOI:10.1371/journal.pone.0205977] [PMID]
Yaya, S., et al., 2019. Decomposing the rural-urban gap in the factors of under-five mortality in sub-Saharan Africa? Evidence from 35 countries. BMC Public Health, 19(1), pp. 1-10. [DOI:10.1186/s12889-019-6940-9] [PMID]
Yaya, S. et al., 2020. Time trends, geographical, socioeconomic, and gender disparities in neonatal mortality in Burundi: evidence from the demographic and health surveys, 2010-2016. Archives of Public Health. Archives of Public Health, 78(1), pp. 115. [DOI:10.1186/s13690-020-00501-3] [PMID]
Zhang, X. et al., 2024. Adult Childrens’ College Completion Timing and Their Aging Mothers’ Self-Rated Health: The Role of Mothers’ Educational Attainment. Journal of Adult Development, 32, pp. 159–71. [DOI:10.1007/s10804-024-09484-9]
Type of Study: Research |
Subject:
General
Received: 2025/01/16 | Accepted: 2025/09/6 | Published: 2026/02/1
Received: 2025/01/16 | Accepted: 2025/09/6 | Published: 2026/02/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
