Fri, Jul 17, 2026
[Archive]
Volume 12, Issue 1 (Winter 2026)
JCCNC 2026, 12(1): 59-70 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Khalkhali M, Jabbarzadeh Tabrizi F, Seyyed Rasooli A, Sarbakhsh P, Khajehgoodari M. Nurses’ and Patients’ Perspectives on Missed Nursing Care in Hospitals Affiliated With Tabriz University of Medical Sciences, Tabriz City, Iran. JCCNC 2026; 12 (1) :59-70
URL: http://jccnc.iums.ac.ir/article-1-801-en.html
URL: http://jccnc.iums.ac.ir/article-1-801-en.html
Mahsa Khalkhali1 

 , Faranak Jabbarzadeh Tabrizi *2 , Alehe Seyyed Rasooli1 , Parvin Sarbakhsh3 , Mohammad Khajehgoodari1
, Faranak Jabbarzadeh Tabrizi *2 , Alehe Seyyed Rasooli1 , Parvin Sarbakhsh3 , Mohammad Khajehgoodari1
, Faranak Jabbarzadeh Tabrizi *2 , Alehe Seyyed Rasooli1 , Parvin Sarbakhsh3 , Mohammad Khajehgoodari1
1- Department of Medical Surgical Nursing, Faculty of Nursing and Midwifery, Tabriz University of Medical Sciences, Tabriz, Iran.
2- Department of Medical Surgical Nursing, Faculty of Nursing and Midwifery, Tabriz University of Medical Sciences, Tabriz, Iran. ,jabbarzadehf@tbzmed.ac.ir
3- Health and Environmental Research Center, Tabriz University of medical sciences, Tabriz, Iran.
2- Department of Medical Surgical Nursing, Faculty of Nursing and Midwifery, Tabriz University of Medical Sciences, Tabriz, Iran. ,
3- Health and Environmental Research Center, Tabriz University of medical sciences, Tabriz, Iran.
Keywords: Nurses’ perspective, Patients’ perspective, Delayed care, Missed nursing care, Quality of health care
Full-Text [PDF 644 kb]
(402 Downloads)
| Abstract (HTML) (685 Views)
Full-Text: (59 Views)
Introduction
Care is a fundamental need and the cornerstone of the nursing process (Toney-Butler & Thayer, 2023), aimed at assisting, supporting, and empowering patients. Nurses serve as the front line of patient care (Hämel et al., 2022), ensuring that routine tasks are consistently performed. However, certain aspects of care may be overlooked despite adherence to standard procedures (Assadian et al., 2021).
The term “missed care” was first identified by Kalisch in 2006 (Kalisch & Williams, 2009) and refers to any aspect of patient care that is omitted or delayed (Kalisch & Xie, 2014). Kalisch’s model, derived from a qualitative study on nursing process implementation, highlighted 3 predictive variables: Labor resources, material resources, and communication. These factors play a pivotal role in ensuring proper care delivery. Additionally, individual attributes of nurses, such as beliefs and values, significantly influence whether nursing care is fully executed or missed (Kalisch, 2006).
Regarding the importance of addressing missed care, it should be noted that one of the fundamental rights of hospitalized patients is the assurance that their needs are met and that they receive comprehensive and safe care from the healthcare system. However, under certain conditions, such as staff shortages, some caregiving activities may be omitted or forgotten (Khajooee et al., 2019). Many hospitalized patients are put at risk due to missed care. Consequences such as falls, medication errors, hospital-acquired infections, pressure ulcers, gastrointestinal bleeding, increased pain and discomfort, and readmissions are cited as outcomes of missed care (Kalisch et al., 2012; Stemmer et al., 2022).
Evidence shows that during each shift, nurses miss some aspects of nursing care (Karimi et al., 2021). Missed care often results in negative consequences for both nurses and organizations. At the individual level, nurses experience reduced job satisfaction, while at the organizational level, turnover, absenteeism, and resignations increase. Nurses have described their experiences with moral distress, role disruption, and frustration when unable to provide complete care to their patients (Kalisch et al., 2009; Kalisch, 2006).
Numerous studies conducted in other countries around the world have examined the extent and types of missed nursing care from the nurses’ perspective, as well as the consequences and factors leading to missed care (Papathanasiou et al., 2024; Willis et al., 2024; Mainz et al., 2024; Abere et al., 2024; Mandal & Seethalakshmi, 2023; Heng et al., 2023; Kalánková et al., 2020; Moreno-Monsiváis et al.; 2015, Gustafsson et al., 2020). Similarly, studies in Iran have investigated the extent and types of missed nursing care from the nurses’ perspective, the associated factors, and nurses’ experiences with missed care (Chegini et al., 2020; Janatolmakan & Khatony, 2022a; Babaei et al., 2024; Ghorbani et al., 2023; Rezaee et al., 2021; Amrolahi-Mishavan et al.; 2022, Rahmani et al., 2022; Rezaei-Shahsavarloo et al., 2021; Janatolmakan & Khatony, 2022b).
The results regarding the extent, types, and causes of missed care vary across different studies in the country. For example, a 2021 study in Ardabil Province reported that, from the nurses’ perspective, the most missed care involved turning patients every 2 hours and measuring vital signs (Ebadi et al., 2021). A study in Urmia Province identified patients’ emergency conditions, the insufficient number of nursing assistants, and an unexpected increase in patient numbers as contributing factors to missed nursing care (Rezaee et al., 2019). While most studies have focused on nurses’ perspectives, this raises the question of whether patients’ perspectives on missed care are equally important. A scoping review emphasized that since patients actively participate in their care, understanding their perspectives on care that is either inadequately performed or entirely omitted is crucial and constitutes a fundamental aspect of their rights (Gustafsson et al., 2020), especially because studies have shown that missed care occurs more frequently among patients with lower levels of consciousness or those who are critically ill (Kalisch et al., 2014; Cho et al., 2017; Orique et al., 2017).
However, studies evaluating the extent, types, and causes of missed care from patients’ perspectives are very limited. Given that nurses’ and patients’ perspectives on missed care may differ (Gustafsson et al., 2020), comparing these viewpoints is essential. Such comparisons can reveal discrepancies and highlight areas needing improvement.
Despite the importance of this comparison, no comprehensive study has addressed this topic in Iran. Most existing studies have focused solely on nurses’ perspectives (Karimi et al., 2021; Rezaee et al., 2021; Ebadi et al., 2021; Yaghoubi et al., 2019), potentially overlooking critical aspects of care that patients deem important. Therefore, this study aims to bridge this gap by comparing nurses’ and patients’ perspectives on missed nursing care in medical-surgical wards. The findings are expected to provide valuable insights that enhance the quality of care in medical-surgical departments.
Materials and Methods
Design, setting, and sample
This descriptive comparative cross-sectional study was conducted in the medical-surgical departments of 7 teaching hospitals affiliated with Tabriz University of Medical Sciences (Imam Reza, Sina, Shohada, Nikookari, Alzahra, Taleghani, and Alavi) in 2024.
The sample size was determined using a similar study that compared nurses’ and patients’ perspectives on missed care (Moreno-Monsiváis et al., 2015). Based on the reported means and standard deviations from that study, with a power of 80% and a confidence level of 95%, the sample size for both nurses and patients was calculated to be 154 each. Given a 10% attrition rate due to incomplete or invalid questionnaires, the sample size was increased to 172 per group. After eliminating incomplete questionnaires, data from 167 nurses and 164 patients were analyzed.
Nurses were selected using proportionate stratified random sampling based on population size. The sample size was allocated to each hospital department based on the number of nurses, and the desired sample was randomly selected from each department’s list of nurses. For patients, a stratified convenience sampling method was also employed. By estimating the number of hospitalized patients in each department, a sample size proportional to this number was allocated to each department. During sampling, the desired sample was selected from among the hospitalized patients who met the inclusion criteria.
Inclusion and exclusion criteria
The inclusion criteria for nurses were as follows: holding a bachelor’s degree or higher, having at least 6 months of work experience in medical-surgical departments, being employed in these departments at the time of data collection, and lacking concurrent responsibilities in other units (to maintain stability in the study population).
The inclusion criteria for patients were as follows: Age over 18 years, at least 48 hours had passed since hospitalization in the medical-surgical department, no known cognitive or psychiatric disorders (Gharaeipour & Andrew, 2013), and awareness of time and place, which is determined by obtaining a minimum score of 24 on the mini-mental state examination (MMSE). This questionnaire has open questions to assess a person’s mental state and memory in dimensions such as orientation to time and place, attention, and recall (Gharaeipour & Andrew, 2013). Incomplete questionnaires were discarded in both groups.
Data collection
Data were collected by the Mahsa Khalkhali from February to June 2024. To collect data from nurses who met the inclusion criteria, the researcher visited the relevant departments during different shifts and explained the study’s objectives and procedures. The time for completing the questionnaire was determined by the nurses (e.g. during a break at breakfast). Regarding data collection from eligible patients, after explaining the study objectives, the questions and options were read aloud to illiterate patients, and their responses were recorded in the questionnaire. Patients were asked to complete the questionnaires when they were comfortable and relatively calm. To ensure the accuracy of the data collected, the researchers emphasized their commitment to confidentiality and data protection.
Study instruments
Data were collected from nurses and patients using demographic questionnaires and the missed nursing care survey (MISSCARE survey).
The nurses’ demographic questionnaire included items on age, gender, marital status, education level, employment status, hospital and department of employment, years of hospital experience, years of experience in medical- surgical departments, interest in the nursing profession, and work schedule details such as the number and type of shifts. The patients’ demographic questionnaire collected information on age, gender, marital status, number of children, education level, residence status (local/non-local), hospitalization history, length of hospital stay, and admission department. While the basic structure of these questionnaires was derived from Kalisch’s scale, modifications were made, particularly for patients, to better align with the study objectives.
The MISSCARE survey was developed by Kalisch & Williams (2009) and was psychometrically evaluated in 2009 (Kalisch & Williams, 2009). This questionnaire assesses the frequency of missed nursing care activities and their contributing factors. Each section can be used independently (Khajooee et al., 2019). In this study, we employed only the section evaluating missed nursing care.
The original version demonstrated high reliability with a Cronbach α of 0.94 (Kalisch & Williams, 2009). The Persian version of the questionnaire, validated by Khajooee et al. (2019), demonstrated strong psychometric properties, with a Cronbach α of 0.91.
The section of measuring missed nursing care consists of 24 items. Responses are rated on a Likert scale from 1 to 5, with higher scores indicating greater frequency of missed nursing care (Khajooee et al., 2019). The modifications in this study, similar to the study conducted in Mexico (Moreno-Monsiváis et al., 2015), were limited to the inclusion of parenthetical examples to facilitate patients’ understanding. For example, vital signs were added as “e.g., blood pressure, fever, etc.” After adding examples, the questionnaire’s validity was confirmed by 10 faculty members at Tabriz University of Medical Sciences, and its Cronbach α was estimated at 0.91.
Data analysis
The collected data were analyzed using SPSS software, version 21. The Kolmogorov-Smirnov normality test was performed, and the results were not statistically significant (P>0.05), indicating that the distributions of the variables were normal. To describe the quantitative data, the mean and standard deviation were used. The mean scores for patients’ and nurses’ perspectives were estimated both pointwise and with 95% confidence intervals. Additionally, the mean scores were converted to a 1 to 5 scale and analyzed using the independent t-test, the Pearson correlation coefficient, and one-way analysis of variance (ANOVA). Significance level was set at P≤0.05 for all tests.
Results
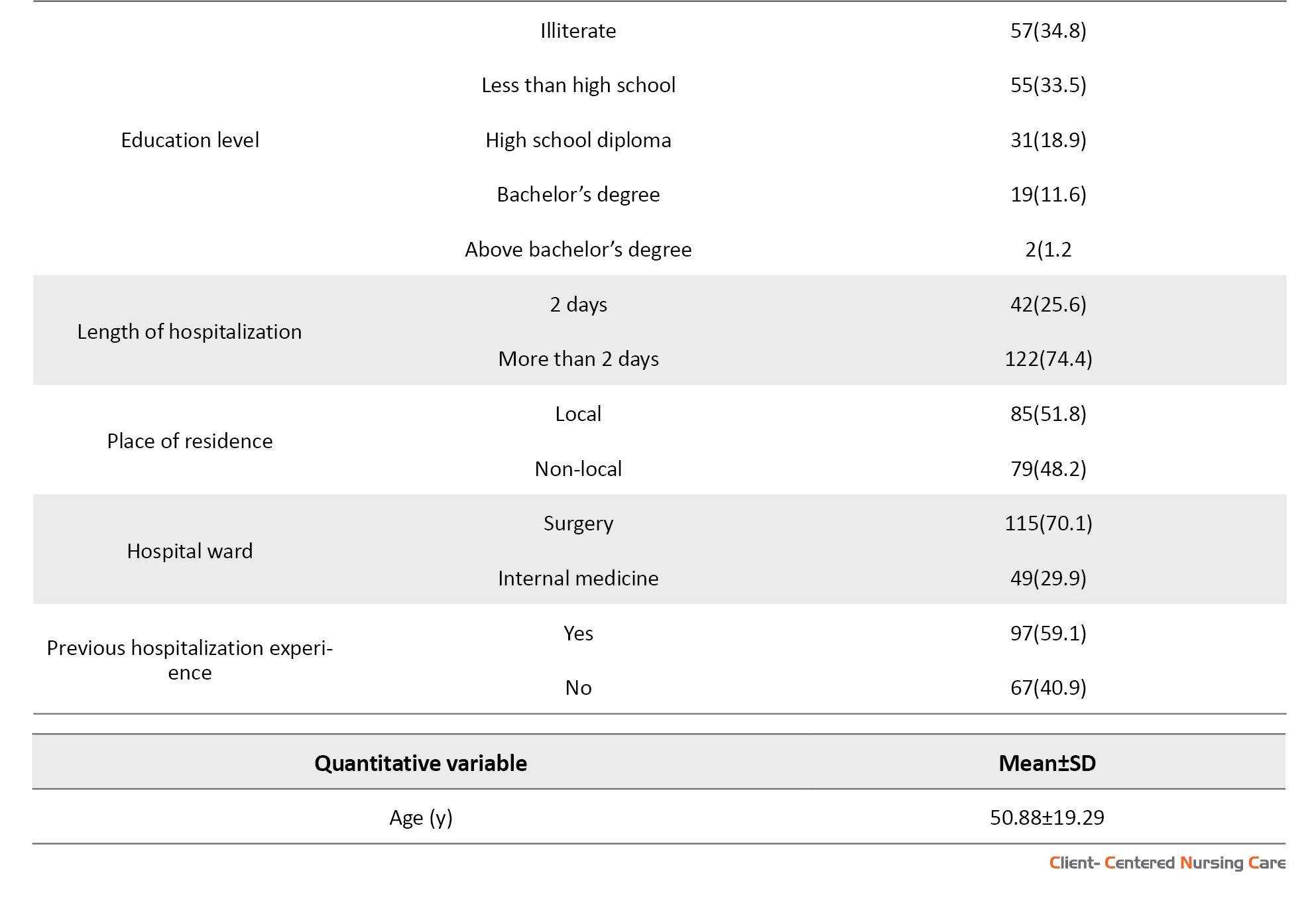
The study results showed that the majority of participating nurses were female (56.9%), married (53.3%), and held a bachelor’s degree (85.6%). The mean age of the nurses was 30.03±4.90 years. The mean age of the patients was 50.89±19.27 years, including 65 men (38.5%) and 99 women (58.6%) (Table 1).
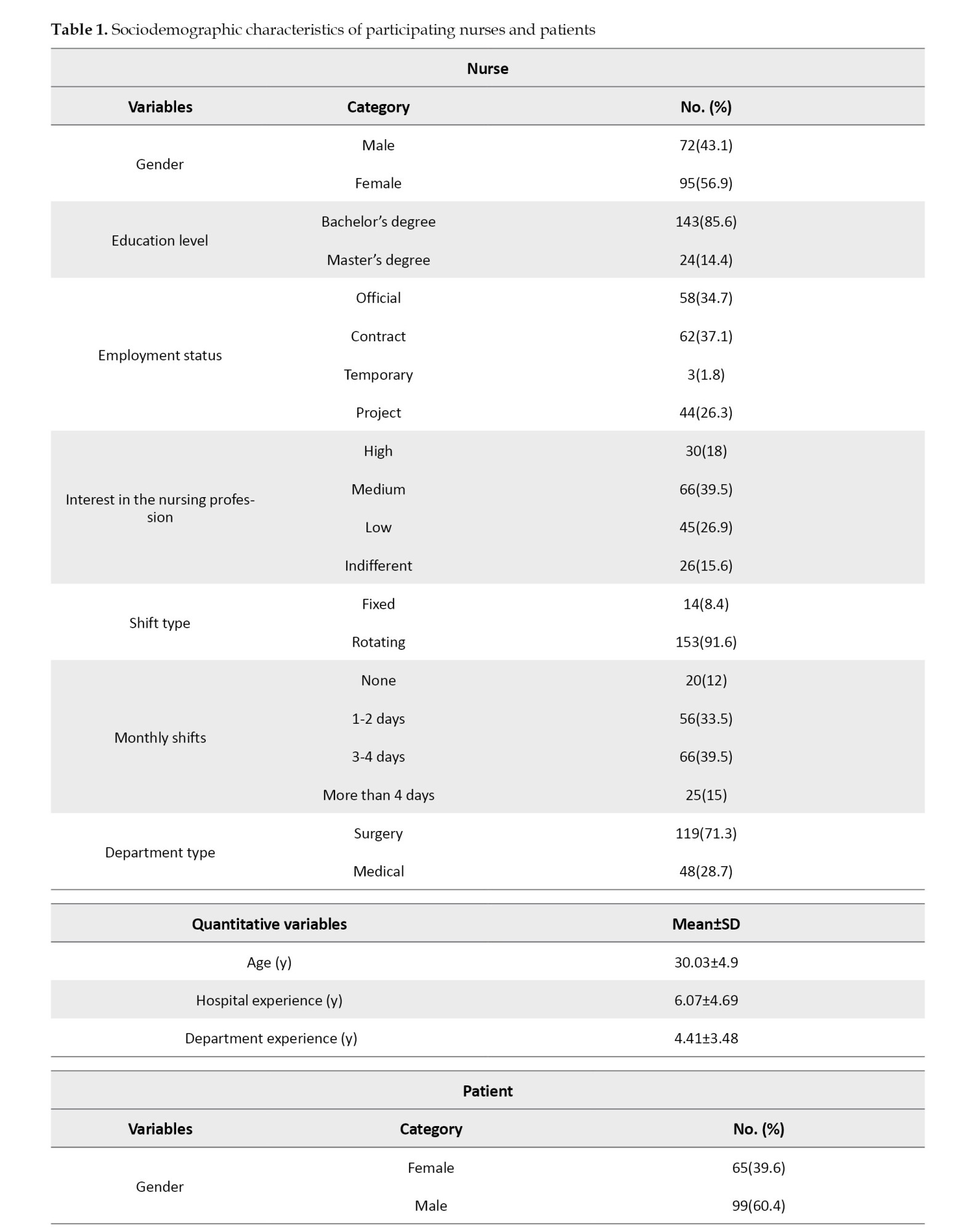
In the present study, a borderline statistically significant association was observed between interest in the nursing profession and the extent of missed care (P=0.05). However, no statistically significant relationships were found between missed care and other demographic variables, either among nurses or patients (P>0.05).
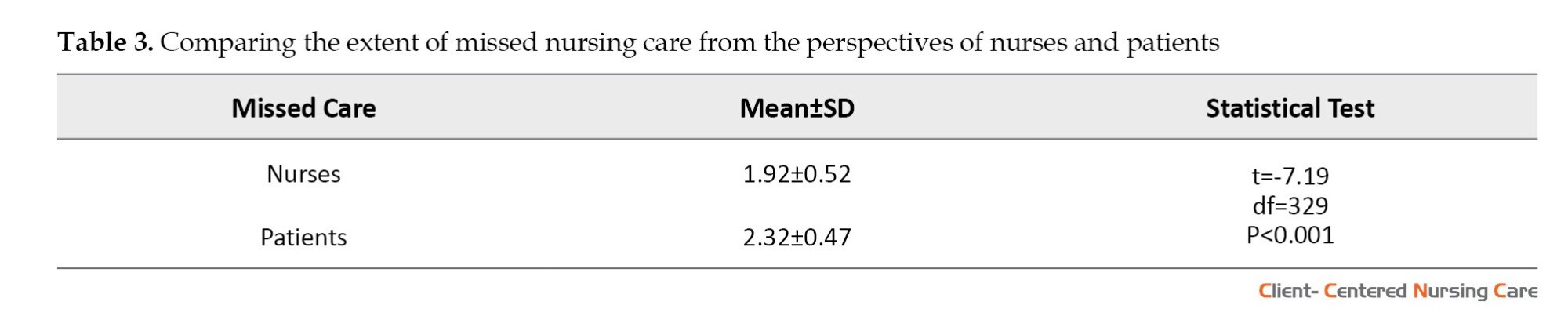
The overall mean score for missed nursing care was 1.92±0.52 from nurses’ perspective and 2.32±0.47 from patients’ perspective. From the nurses’ perspective, the two most frequently missed care items, as indicated by the highest mean scores, were “supervision or assistance with oral hygiene” (3.06±1.07) and “nurse supervision of the eating habits of all patients” (3.06±1.07). From the patients’ perspective, the two highest mean scores were “supervision of bathing or daily skin care (e.g. hand and face washing)” (3.59±1.35) and “supervision or assistance with oral hygiene” (3.34±1.33) (Table 2).

The lowest mean score from the nurses’ perspective was related to the item “inquiring about fluid intake (e.g. tea, water) and urinary function" (1.3±0.54), and from the patients’ perspective, it was related to the item «administration of medications regularly and daily» (1.48±0.73) (Table 2). There was a statistically significant difference between the extent of missed care perceived by patients and nurses (Table 3, P<0.001), indicating that patients perceived a greater extent of missed nursing care (Table 3).
Discussion
This study highlights a significant difference between patients’ and nurses’ perceptions of missed nursing care. From the nurses’ perspective, the most frequently missed care items were monitoring or assisting with patients’ oral hygiene and supervising their dietary habits. From the patients’ perspective, supervision of bathing or daily skin care was reported as the most frequently missed care, followed closely by supervision or assistance with oral hygiene—the latter aligning with nurses’ perceptions. Nurses, given resource constraints and their clinical responsibilities, tend to focus on physiologically essential tasks, such as assessing fluid intake and urinary function, daily measurement of vital signs and pain, and providing care for intravenous catheters. In contrast, patients who experience care up close prioritize comfort and basic hygiene needs, with bathing and skin cleanliness being cited as their most important concerns (Endalamaw et al., 2024). These discrepancies underscore the need for a patient-centered framework that aligns clinical standards with patients’ values to ensure comprehensive, holistic nursing care.
In the study by Kalisch et al. (2011), oral care also receives the highest average score for missed care from the nurses’ perspective. Jenson and colleagues argue that nurses in internal-surgical units are in a position to influence oral care outcomes and reduce related diseases, and this can be achieved through proper staff training (Jenson et al., 2018). Initially, it might seem that overlooking this care is not critical, but it is important to remember that oral infections can spread to other parts of the body. Additionally, poor oral hygiene affects patients’ appetite and willingness to eat (Rajasekaran et al., 2024). Neglecting this care during hospitalization can lead to dental decay or gum infections, resulting in additional dental costs post-discharge. Therefore, educating nurses on the importance of routine oral care could reduce instances of this type of missed care at the bedside.
Modern studies indicate that daily bathing significantly reduces infection rates (Reynolds et al., 2021). Bathing not only helps maintain patient hygiene but also reduces body odor, stimulates blood circulation, and enhances patient comfort and relaxation. Additionally, bathing provides nurses with the opportunity to inspect patients’ skin and identify potential problems early. However, patient bathing in hospital settings might be overlooked or inadequately performed (Abbas & Sastry, 2016; Tai et al., 2021). Factors such as staff shortages, high workload, and poor coordination among healthcare teams can contribute to the neglect of this crucial care (Moreno-Monsiváis et al., 2015).
Our study found that patients perceived the extent of missed care as moderate, with a higher percentage of missed care than nurses reported. In other words, nurses in this study perceived the overall extent of missed care as notably lower than patients did. Some other studies also indicate that missed nursing care has been perceived as moderate from the nurses’ perspective (Karadaş et al., 2024; Mainz et al., 2024; Abere et al., 2024; Mandal & Seethalakshmi, 2023; Heng et al., 2023; Kalánková et al., 2020; Gustafsson et al., 2020; Moreno-Monsiváis et al., 2015).
The difference between nurses’ and patients’ perceptions of missed care, and patients’ higher perception of it, warrants careful analysis. We propose 3 interrelated explanations rooted in systemic challenges. First, chronic nursing shortages compel task triage, relegating «non-urgent» hygiene care despite its profound impact on patient dignity and infection risk (Papathanasiou et al., 2024). Second, supervisory practices disproportionately emphasize visible, technical tasks (e.g. medication administration, wound care) while overlooking holistic processes like bathing or emotional support (Southard, 2024). This “surveillance bias” implicitly signals that non-technical care is expendable (Moreno-Monsiváis et al., 2015). Third, concurrent employment across hospitals induces fatigue, further narrowing focus to checklist-driven tasks at the expense of holistic care (Abbaszadeh et al., 2025). Consequently, nurses’ lower missed-care ratings reflect adaptation to institutional constraints that normalize omissions of “low-priority” hygiene interventions. The specific missed care items also reflect these systemic pressures. Nurses’ emphasis on omitting oral care aligns with global patterns (Kalisch & Xie, 2014); its neglect—though often perceived as non-urgent—predisposes patients to systemic infections, malnutrition, and post-discharge dental morbidity (Rajasekaran et al., 2024). Conversely, patients’ emphasis on omissions in bathing/skin care highlights a critical dignity deficit. Bathing transcends hygiene; it embodies comfort, promotes circulation, enables skin assessment, and reduces hospital-acquired infections (Reynolds et al., 2021). That patients rated overall missed care as moderate—significantly higher than nurses—reflects their heightened sensitivity to omissions impacting well-being and autonomy. In contrast, nurses may normalize compromises due to resource constraints (Maghsoud et al., 2022).
Regarding demographic variables, there was a borderline statistical relationship between nurses’ professional interest and the extent of missed care, with greater engagement correlating with lower missed care. This finding suggests that intrinsic motivation may help mitigate missed nursing care (Srulovici & Yanovich, 2022), reinforcing the importance of nurturing professional engagement through autonomy, recognition, and supportive supervision to enhance care quality (Delima et al., 2024). To improve the quality of nursing care, it is essential to consider both patients’ and nurses’ perspectives simultaneously, as previous studies have emphasized this point (Karadaş et al., 2024; Mainz et al., 2024; Abere et al., 2024; Mandal & Seethalakshmi, 2023; Heng et al., 2023; Kalánková et al., 2020; Gustafsson et al., 2020; Moreno-Monsiváis et al., 2015). Such an approach may enhance patient satisfaction and alleviate nurses’ workload-related challenges.
This study is subject to the inherent limitations of cross-sectional studies that prevent the establishment of causal relationships. Furthermore, self-reported data may not always accurately reflect reality, as responses can be influenced by various factors such as recall bias, subjective interpretation, or response tendencies.
Conclusion
This study showed significant differences between the perspectives of patients and nurses regarding missed nursing care. The findings indicated that, from the nurses’ perspective, the most frequently missed care was monitoring patients’ eating habits and oral care. In contrast, patients highlighted supervision of bathing and daily skin care. These differences suggest that improving nursing care quality requires considering the views of both groups. Further studies in this field can help to identify missed care more accurately and provide appropriate solutions to improve the quality of care. It is also recommended to use the second part of the questionnaire to identify factors affecting missed care.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of Tabriz University of Medical Sciences, Tabriz, Iran (Code: IR.TBZMED.REC.1402.612). The study adhered to the ethical standards outlined in the Helsinki Declaration. Participants were informed of the study’s purpose, and written informed consent was obtained.
Funding
This study was extracted from the master’s thesis of Mahsa Khalkhali, approved by the Department of Medical Surgical Nursing, Faculty of Nursing and Midwifery, Tabriz University of Medical Sciences, Tabriz, Iran. This study was financially supported by Tabriz University of Medical Sciences, Tabriz, Iran.
Authors' contributions
Conceptualization: Faranak Jabbarzadeh Tabrizi. and Mohammad Khajehgoodari; Methodology and analysis: Mohammad Khajehgoodari and Parvin Sarbakhsh; Supervision and project administration: Faranak Jabbarzadeh Tabrizi and Alehe Seyyed Rasooli; Data collection and writing the initial draft: Mahsa Khalkhali and Mohammad Khajehgoodari; Review and editing: Faranak Jabbarzadeh Tabrizi and Mohammad Khajehgoodari; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The researchers extend their sincere gratitude to the nurses and patients who participated in the study, as well as the administration of the selected hospitals, Imam Reza, Sina, Shohada, Al-Zahra, Alavi, Nikookari, and Taleghani, for their cooperation and support in the sampling process. Additionally, appreciation is expressed to the Deputy of Research and Technology at Tabriz University of Medical Sciences for their valuable support in facilitating this research.
References
Care is a fundamental need and the cornerstone of the nursing process (Toney-Butler & Thayer, 2023), aimed at assisting, supporting, and empowering patients. Nurses serve as the front line of patient care (Hämel et al., 2022), ensuring that routine tasks are consistently performed. However, certain aspects of care may be overlooked despite adherence to standard procedures (Assadian et al., 2021).
The term “missed care” was first identified by Kalisch in 2006 (Kalisch & Williams, 2009) and refers to any aspect of patient care that is omitted or delayed (Kalisch & Xie, 2014). Kalisch’s model, derived from a qualitative study on nursing process implementation, highlighted 3 predictive variables: Labor resources, material resources, and communication. These factors play a pivotal role in ensuring proper care delivery. Additionally, individual attributes of nurses, such as beliefs and values, significantly influence whether nursing care is fully executed or missed (Kalisch, 2006).
Regarding the importance of addressing missed care, it should be noted that one of the fundamental rights of hospitalized patients is the assurance that their needs are met and that they receive comprehensive and safe care from the healthcare system. However, under certain conditions, such as staff shortages, some caregiving activities may be omitted or forgotten (Khajooee et al., 2019). Many hospitalized patients are put at risk due to missed care. Consequences such as falls, medication errors, hospital-acquired infections, pressure ulcers, gastrointestinal bleeding, increased pain and discomfort, and readmissions are cited as outcomes of missed care (Kalisch et al., 2012; Stemmer et al., 2022).
Evidence shows that during each shift, nurses miss some aspects of nursing care (Karimi et al., 2021). Missed care often results in negative consequences for both nurses and organizations. At the individual level, nurses experience reduced job satisfaction, while at the organizational level, turnover, absenteeism, and resignations increase. Nurses have described their experiences with moral distress, role disruption, and frustration when unable to provide complete care to their patients (Kalisch et al., 2009; Kalisch, 2006).
Numerous studies conducted in other countries around the world have examined the extent and types of missed nursing care from the nurses’ perspective, as well as the consequences and factors leading to missed care (Papathanasiou et al., 2024; Willis et al., 2024; Mainz et al., 2024; Abere et al., 2024; Mandal & Seethalakshmi, 2023; Heng et al., 2023; Kalánková et al., 2020; Moreno-Monsiváis et al.; 2015, Gustafsson et al., 2020). Similarly, studies in Iran have investigated the extent and types of missed nursing care from the nurses’ perspective, the associated factors, and nurses’ experiences with missed care (Chegini et al., 2020; Janatolmakan & Khatony, 2022a; Babaei et al., 2024; Ghorbani et al., 2023; Rezaee et al., 2021; Amrolahi-Mishavan et al.; 2022, Rahmani et al., 2022; Rezaei-Shahsavarloo et al., 2021; Janatolmakan & Khatony, 2022b).
The results regarding the extent, types, and causes of missed care vary across different studies in the country. For example, a 2021 study in Ardabil Province reported that, from the nurses’ perspective, the most missed care involved turning patients every 2 hours and measuring vital signs (Ebadi et al., 2021). A study in Urmia Province identified patients’ emergency conditions, the insufficient number of nursing assistants, and an unexpected increase in patient numbers as contributing factors to missed nursing care (Rezaee et al., 2019). While most studies have focused on nurses’ perspectives, this raises the question of whether patients’ perspectives on missed care are equally important. A scoping review emphasized that since patients actively participate in their care, understanding their perspectives on care that is either inadequately performed or entirely omitted is crucial and constitutes a fundamental aspect of their rights (Gustafsson et al., 2020), especially because studies have shown that missed care occurs more frequently among patients with lower levels of consciousness or those who are critically ill (Kalisch et al., 2014; Cho et al., 2017; Orique et al., 2017).
However, studies evaluating the extent, types, and causes of missed care from patients’ perspectives are very limited. Given that nurses’ and patients’ perspectives on missed care may differ (Gustafsson et al., 2020), comparing these viewpoints is essential. Such comparisons can reveal discrepancies and highlight areas needing improvement.
Despite the importance of this comparison, no comprehensive study has addressed this topic in Iran. Most existing studies have focused solely on nurses’ perspectives (Karimi et al., 2021; Rezaee et al., 2021; Ebadi et al., 2021; Yaghoubi et al., 2019), potentially overlooking critical aspects of care that patients deem important. Therefore, this study aims to bridge this gap by comparing nurses’ and patients’ perspectives on missed nursing care in medical-surgical wards. The findings are expected to provide valuable insights that enhance the quality of care in medical-surgical departments.
Materials and Methods
Design, setting, and sample
This descriptive comparative cross-sectional study was conducted in the medical-surgical departments of 7 teaching hospitals affiliated with Tabriz University of Medical Sciences (Imam Reza, Sina, Shohada, Nikookari, Alzahra, Taleghani, and Alavi) in 2024.
The sample size was determined using a similar study that compared nurses’ and patients’ perspectives on missed care (Moreno-Monsiváis et al., 2015). Based on the reported means and standard deviations from that study, with a power of 80% and a confidence level of 95%, the sample size for both nurses and patients was calculated to be 154 each. Given a 10% attrition rate due to incomplete or invalid questionnaires, the sample size was increased to 172 per group. After eliminating incomplete questionnaires, data from 167 nurses and 164 patients were analyzed.
Nurses were selected using proportionate stratified random sampling based on population size. The sample size was allocated to each hospital department based on the number of nurses, and the desired sample was randomly selected from each department’s list of nurses. For patients, a stratified convenience sampling method was also employed. By estimating the number of hospitalized patients in each department, a sample size proportional to this number was allocated to each department. During sampling, the desired sample was selected from among the hospitalized patients who met the inclusion criteria.
Inclusion and exclusion criteria
The inclusion criteria for nurses were as follows: holding a bachelor’s degree or higher, having at least 6 months of work experience in medical-surgical departments, being employed in these departments at the time of data collection, and lacking concurrent responsibilities in other units (to maintain stability in the study population).
The inclusion criteria for patients were as follows: Age over 18 years, at least 48 hours had passed since hospitalization in the medical-surgical department, no known cognitive or psychiatric disorders (Gharaeipour & Andrew, 2013), and awareness of time and place, which is determined by obtaining a minimum score of 24 on the mini-mental state examination (MMSE). This questionnaire has open questions to assess a person’s mental state and memory in dimensions such as orientation to time and place, attention, and recall (Gharaeipour & Andrew, 2013). Incomplete questionnaires were discarded in both groups.
Data collection
Data were collected by the Mahsa Khalkhali from February to June 2024. To collect data from nurses who met the inclusion criteria, the researcher visited the relevant departments during different shifts and explained the study’s objectives and procedures. The time for completing the questionnaire was determined by the nurses (e.g. during a break at breakfast). Regarding data collection from eligible patients, after explaining the study objectives, the questions and options were read aloud to illiterate patients, and their responses were recorded in the questionnaire. Patients were asked to complete the questionnaires when they were comfortable and relatively calm. To ensure the accuracy of the data collected, the researchers emphasized their commitment to confidentiality and data protection.
Study instruments
Data were collected from nurses and patients using demographic questionnaires and the missed nursing care survey (MISSCARE survey).
The nurses’ demographic questionnaire included items on age, gender, marital status, education level, employment status, hospital and department of employment, years of hospital experience, years of experience in medical- surgical departments, interest in the nursing profession, and work schedule details such as the number and type of shifts. The patients’ demographic questionnaire collected information on age, gender, marital status, number of children, education level, residence status (local/non-local), hospitalization history, length of hospital stay, and admission department. While the basic structure of these questionnaires was derived from Kalisch’s scale, modifications were made, particularly for patients, to better align with the study objectives.
The MISSCARE survey was developed by Kalisch & Williams (2009) and was psychometrically evaluated in 2009 (Kalisch & Williams, 2009). This questionnaire assesses the frequency of missed nursing care activities and their contributing factors. Each section can be used independently (Khajooee et al., 2019). In this study, we employed only the section evaluating missed nursing care.
The original version demonstrated high reliability with a Cronbach α of 0.94 (Kalisch & Williams, 2009). The Persian version of the questionnaire, validated by Khajooee et al. (2019), demonstrated strong psychometric properties, with a Cronbach α of 0.91.
The section of measuring missed nursing care consists of 24 items. Responses are rated on a Likert scale from 1 to 5, with higher scores indicating greater frequency of missed nursing care (Khajooee et al., 2019). The modifications in this study, similar to the study conducted in Mexico (Moreno-Monsiváis et al., 2015), were limited to the inclusion of parenthetical examples to facilitate patients’ understanding. For example, vital signs were added as “e.g., blood pressure, fever, etc.” After adding examples, the questionnaire’s validity was confirmed by 10 faculty members at Tabriz University of Medical Sciences, and its Cronbach α was estimated at 0.91.
Data analysis
The collected data were analyzed using SPSS software, version 21. The Kolmogorov-Smirnov normality test was performed, and the results were not statistically significant (P>0.05), indicating that the distributions of the variables were normal. To describe the quantitative data, the mean and standard deviation were used. The mean scores for patients’ and nurses’ perspectives were estimated both pointwise and with 95% confidence intervals. Additionally, the mean scores were converted to a 1 to 5 scale and analyzed using the independent t-test, the Pearson correlation coefficient, and one-way analysis of variance (ANOVA). Significance level was set at P≤0.05 for all tests.
Results
The study results showed that the majority of participating nurses were female (56.9%), married (53.3%), and held a bachelor’s degree (85.6%). The mean age of the nurses was 30.03±4.90 years. The mean age of the patients was 50.89±19.27 years, including 65 men (38.5%) and 99 women (58.6%) (Table 1).
In the present study, a borderline statistically significant association was observed between interest in the nursing profession and the extent of missed care (P=0.05). However, no statistically significant relationships were found between missed care and other demographic variables, either among nurses or patients (P>0.05).
The overall mean score for missed nursing care was 1.92±0.52 from nurses’ perspective and 2.32±0.47 from patients’ perspective. From the nurses’ perspective, the two most frequently missed care items, as indicated by the highest mean scores, were “supervision or assistance with oral hygiene” (3.06±1.07) and “nurse supervision of the eating habits of all patients” (3.06±1.07). From the patients’ perspective, the two highest mean scores were “supervision of bathing or daily skin care (e.g. hand and face washing)” (3.59±1.35) and “supervision or assistance with oral hygiene” (3.34±1.33) (Table 2).
The lowest mean score from the nurses’ perspective was related to the item “inquiring about fluid intake (e.g. tea, water) and urinary function" (1.3±0.54), and from the patients’ perspective, it was related to the item «administration of medications regularly and daily» (1.48±0.73) (Table 2). There was a statistically significant difference between the extent of missed care perceived by patients and nurses (Table 3, P<0.001), indicating that patients perceived a greater extent of missed nursing care (Table 3).
Discussion
This study highlights a significant difference between patients’ and nurses’ perceptions of missed nursing care. From the nurses’ perspective, the most frequently missed care items were monitoring or assisting with patients’ oral hygiene and supervising their dietary habits. From the patients’ perspective, supervision of bathing or daily skin care was reported as the most frequently missed care, followed closely by supervision or assistance with oral hygiene—the latter aligning with nurses’ perceptions. Nurses, given resource constraints and their clinical responsibilities, tend to focus on physiologically essential tasks, such as assessing fluid intake and urinary function, daily measurement of vital signs and pain, and providing care for intravenous catheters. In contrast, patients who experience care up close prioritize comfort and basic hygiene needs, with bathing and skin cleanliness being cited as their most important concerns (Endalamaw et al., 2024). These discrepancies underscore the need for a patient-centered framework that aligns clinical standards with patients’ values to ensure comprehensive, holistic nursing care.
In the study by Kalisch et al. (2011), oral care also receives the highest average score for missed care from the nurses’ perspective. Jenson and colleagues argue that nurses in internal-surgical units are in a position to influence oral care outcomes and reduce related diseases, and this can be achieved through proper staff training (Jenson et al., 2018). Initially, it might seem that overlooking this care is not critical, but it is important to remember that oral infections can spread to other parts of the body. Additionally, poor oral hygiene affects patients’ appetite and willingness to eat (Rajasekaran et al., 2024). Neglecting this care during hospitalization can lead to dental decay or gum infections, resulting in additional dental costs post-discharge. Therefore, educating nurses on the importance of routine oral care could reduce instances of this type of missed care at the bedside.
Modern studies indicate that daily bathing significantly reduces infection rates (Reynolds et al., 2021). Bathing not only helps maintain patient hygiene but also reduces body odor, stimulates blood circulation, and enhances patient comfort and relaxation. Additionally, bathing provides nurses with the opportunity to inspect patients’ skin and identify potential problems early. However, patient bathing in hospital settings might be overlooked or inadequately performed (Abbas & Sastry, 2016; Tai et al., 2021). Factors such as staff shortages, high workload, and poor coordination among healthcare teams can contribute to the neglect of this crucial care (Moreno-Monsiváis et al., 2015).
Our study found that patients perceived the extent of missed care as moderate, with a higher percentage of missed care than nurses reported. In other words, nurses in this study perceived the overall extent of missed care as notably lower than patients did. Some other studies also indicate that missed nursing care has been perceived as moderate from the nurses’ perspective (Karadaş et al., 2024; Mainz et al., 2024; Abere et al., 2024; Mandal & Seethalakshmi, 2023; Heng et al., 2023; Kalánková et al., 2020; Gustafsson et al., 2020; Moreno-Monsiváis et al., 2015).
The difference between nurses’ and patients’ perceptions of missed care, and patients’ higher perception of it, warrants careful analysis. We propose 3 interrelated explanations rooted in systemic challenges. First, chronic nursing shortages compel task triage, relegating «non-urgent» hygiene care despite its profound impact on patient dignity and infection risk (Papathanasiou et al., 2024). Second, supervisory practices disproportionately emphasize visible, technical tasks (e.g. medication administration, wound care) while overlooking holistic processes like bathing or emotional support (Southard, 2024). This “surveillance bias” implicitly signals that non-technical care is expendable (Moreno-Monsiváis et al., 2015). Third, concurrent employment across hospitals induces fatigue, further narrowing focus to checklist-driven tasks at the expense of holistic care (Abbaszadeh et al., 2025). Consequently, nurses’ lower missed-care ratings reflect adaptation to institutional constraints that normalize omissions of “low-priority” hygiene interventions. The specific missed care items also reflect these systemic pressures. Nurses’ emphasis on omitting oral care aligns with global patterns (Kalisch & Xie, 2014); its neglect—though often perceived as non-urgent—predisposes patients to systemic infections, malnutrition, and post-discharge dental morbidity (Rajasekaran et al., 2024). Conversely, patients’ emphasis on omissions in bathing/skin care highlights a critical dignity deficit. Bathing transcends hygiene; it embodies comfort, promotes circulation, enables skin assessment, and reduces hospital-acquired infections (Reynolds et al., 2021). That patients rated overall missed care as moderate—significantly higher than nurses—reflects their heightened sensitivity to omissions impacting well-being and autonomy. In contrast, nurses may normalize compromises due to resource constraints (Maghsoud et al., 2022).
Regarding demographic variables, there was a borderline statistical relationship between nurses’ professional interest and the extent of missed care, with greater engagement correlating with lower missed care. This finding suggests that intrinsic motivation may help mitigate missed nursing care (Srulovici & Yanovich, 2022), reinforcing the importance of nurturing professional engagement through autonomy, recognition, and supportive supervision to enhance care quality (Delima et al., 2024). To improve the quality of nursing care, it is essential to consider both patients’ and nurses’ perspectives simultaneously, as previous studies have emphasized this point (Karadaş et al., 2024; Mainz et al., 2024; Abere et al., 2024; Mandal & Seethalakshmi, 2023; Heng et al., 2023; Kalánková et al., 2020; Gustafsson et al., 2020; Moreno-Monsiváis et al., 2015). Such an approach may enhance patient satisfaction and alleviate nurses’ workload-related challenges.
This study is subject to the inherent limitations of cross-sectional studies that prevent the establishment of causal relationships. Furthermore, self-reported data may not always accurately reflect reality, as responses can be influenced by various factors such as recall bias, subjective interpretation, or response tendencies.
Conclusion
This study showed significant differences between the perspectives of patients and nurses regarding missed nursing care. The findings indicated that, from the nurses’ perspective, the most frequently missed care was monitoring patients’ eating habits and oral care. In contrast, patients highlighted supervision of bathing and daily skin care. These differences suggest that improving nursing care quality requires considering the views of both groups. Further studies in this field can help to identify missed care more accurately and provide appropriate solutions to improve the quality of care. It is also recommended to use the second part of the questionnaire to identify factors affecting missed care.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of Tabriz University of Medical Sciences, Tabriz, Iran (Code: IR.TBZMED.REC.1402.612). The study adhered to the ethical standards outlined in the Helsinki Declaration. Participants were informed of the study’s purpose, and written informed consent was obtained.
Funding
This study was extracted from the master’s thesis of Mahsa Khalkhali, approved by the Department of Medical Surgical Nursing, Faculty of Nursing and Midwifery, Tabriz University of Medical Sciences, Tabriz, Iran. This study was financially supported by Tabriz University of Medical Sciences, Tabriz, Iran.
Authors' contributions
Conceptualization: Faranak Jabbarzadeh Tabrizi. and Mohammad Khajehgoodari; Methodology and analysis: Mohammad Khajehgoodari and Parvin Sarbakhsh; Supervision and project administration: Faranak Jabbarzadeh Tabrizi and Alehe Seyyed Rasooli; Data collection and writing the initial draft: Mahsa Khalkhali and Mohammad Khajehgoodari; Review and editing: Faranak Jabbarzadeh Tabrizi and Mohammad Khajehgoodari; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The researchers extend their sincere gratitude to the nurses and patients who participated in the study, as well as the administration of the selected hospitals, Imam Reza, Sina, Shohada, Al-Zahra, Alavi, Nikookari, and Taleghani, for their cooperation and support in the sampling process. Additionally, appreciation is expressed to the Deputy of Research and Technology at Tabriz University of Medical Sciences for their valuable support in facilitating this research.
References
Abbas, S. & Sastry, S., 2016. Chlorhexidine: Patient bathing and infection prevention. Current Infectious Disease Reports, 18, pp. 1-5. [DOI:10.1007/s11908-016-0532-y] [PMID]
Abbaszadeh, R., et al., 2025. Contributors to fatigue among nurses working in critical care units: A qualitative study. Nursing in Critical Care, 30, pp. e13091. [DOI:10.1111/nicc.70088] [PMID]
Abere, Y., et al., 2024. Magnitude and reasons for missed nursing care among nurses working in South Gondar Zone public hospitals, Amhara regional state, Northcentral Ethiopia: Institution-based cross-sectional study. BMC Nursing, 23, pp. 765. [DOI:10.1186/s12912-024-02438-2] [PMID]
Amrolahi-Mishavan, F., et al., 2022. Factors affecting missed nursing care in hospitals: A scoping review. Health Sciences Review, 4, pp. 100053. [DOI:10.1016/j.hsr.2022.100053]
Assadian, O., et al., 2021. Practical recommendations for routine cleaning and disinfection procedures in healthcare institutions: A narrative review. Journal of Hospital Infection, 113, pp. 104-14. [DOI:10.1016/j.jhin.2021.03.010] [PMID]
Babaei, F., et al., 2024. Investigating the relationship between missed/rationed nursing care and organizational commitment in Iranian nurses. BMC Nursing, 23, pp. 540. [DOI:10.1186/s12912-024-02199-y] [PMID]
Chegini, Z., et al., 2020. Missed nursing care and related factors in Iranian hospitals: A cross‐sectional survey. Journal of Nursing Management, 28, pp. 2205-15. [DOI:10.1111/jonm.13055] [PMID]
Cho, S. H., et al., 2017. Relationships between nurse staffing and patients’ experiences, and the mediating effects of missed nursing care. Journal of Nursing Scholarship, 49, pp. 347-55. [DOI:10.1111/jnu.12292] [PMID]
Delima, M., et al., 2024. Relationship of Motivation and Supervision with Nurse Performance in Implementing Nursing Care. International Journal of Nursing Information, 3, pp. 22-30. [DOI:10.58418/ijni.v3i2.103]
Ebadi, J., et al., 2021. Missed nursing care and its related factors in Ardabil and Khalkhal educational and medical centers in 2020. Journal of Health and Care, 23, pp. 78-87. [DOI:10.52547/jhc.23.1.78]
Endalamaw, A., et al., 2024. A scoping review of continuous quality improvement in healthcare system: Conceptualization, models and tools, barriers and facilitators, and impact. BMC Health Services Research, 24(1), pp. 487. [DOI:10.1186/s12913-024-10828-0]
Gharaeipour, M. & Andrew, M. K., 2013. Examining cognitive status of elderly Iranians: Farsi version of the modified mini-mental state examination. Applied Neuropsychology: Adult, 20, pp. 215-20. [DOI:10.1080/09084282.2012.688228] [PMID]
Ghorbani, S. H., et al., 2023. Missed nursing care, the related organizational factors, and strategies for decreasing it from the viewpoints of nurses in university-affiliated hospitals of Birjand in 2019-2020. Iranian Journal of Nursing and Midwifery Research, 28, pp. 604-9. [DOI:10.4103/ijnmr.ijnmr_255_20] [PMID]
Gustafsson, N., et al., 2020. Missed care from the patient’s perspective-a scoping review. Patient Preference and Adherence, pp. 383-400. [DOI:10.2147/PPA.S238024] [PMID]
Hämel, K., et al., 2022. How do nurses support chronically ill clients’ participation and self-management in primary care? A cross-country qualitative study. BMC Primary Care, 23, pp. 85. [DOI:10.1186/s12875-022-01687-x] [PMID]
Heng, L. M. T., et al., 2023. Nurse-Reported Missed Care and Its Association with Staff Demographics and the Work Environment. AJN The American Journal of Nursing, 123, pp. 28-36. [DOI:10.1097/01.NAJ.0000978144.33445.5b] [PMID]
Janatolmakan, M. & Khatony, A., 2022a. Explaining the consequences of missed nursing care from the perspective of nurses: A qualitative descriptive study in Iran. BMC Nursing, 21, pp. 59. [DOI:10.1186/s12912-022-00839-9] [PMID]
Janatolmakan, M. & Khatony, A., 2022b. Explaining the experiences of nurses regarding strategies to prevent missed nursing care: A qualitative study. Journal of Nursing Management, 30, pp. 2054-61. [DOI:10.1111/jonm.13662] [PMID]
Jenson, H., Maddux, S. & Waldo, M., 2018. Improving oral care in hospitalized non-ventilated patients: Standardizing products and protocol. Medsurg Nursing, 27, pp. 38-45. [Link]
Kalánková, D., et al., 2020. Missed, rationed or unfinished nursing care: A scoping review of patient outcomes. Journal of Nursing Management, 28, pp. 1783-97. [DOI:10.1111/jonm.12978] [PMID]
Kalisch, B., Tschannen, D. & Lee, H., 2011. Does missed nursing care predict job satisfaction? Journal of Healthcare Management, 56, pp. 117-34. [DOI:10.1097/00115514-201103000-00007] [PMID]
Kalisch, B. J. 2006. Missed nursing care: A qualitative study. Journal of Nursing Care Quality, 21, pp. 306-13. [DOI:10.1097/00001786-200610000-00006] [PMID]
Kalisch, B. J., Landstrom, G. & Williams, R. A., 2009. Missed nursing care: Errors of omission. Nursing Outlook, 57, pp. 3-9. [DOI:10.1016/j.outlook.2008.05.007] [PMID]
Kalisch, B. J., Tschannen, D. & Lee, K. H., 2012. Missed nursing care, staffing, and patient falls. Journal of Nursing Care Quality, 27, pp. 6-12. [DOI:10.1097/NCQ.0b013e318225aa23] [PMID]
Kalisch, B. J. & Williams, R. A., 2009. Development and psychometric testing of a tool to measure missed nursing care. JONA: The Journal of Nursing Administration, 39, pp. 211-9. [DOI:10.1097/NNA.0b013e3181a23cf5] [PMID]
Kalisch, B. J. & XIE, B., 2014. Errors of omission: Missed nursing care. Western Journal of Nursing Research, 36, pp. 875-890. [DOI:10.1177/0193945914531859] [PMID]
Kalisch, B. J., XIE, B. & DABNEY, B. W., 2014. Patient-reported missed nursing care correlated with adverse events. American Journal of Medical Quality, 29, pp. 415-22. [DOI:10.1177/1062860613501715] [PMID]
Karadaş, A., Ergün, S. & Kaynak, S., 2024. Relationship between missed nursing care and patients’ trust in nurses and satisfaction with care: A cross‐sectional study. Nursing & Health Sciences, 26, pp. e13149. [DOI:10.1111/nhs.13149] [PMID]
Karimi, H., et al., 2021. [Causes of missed nursing care in emergency departments in selected hospitals of Tehran University of Medical Sciences: A descriptive study in Iran (Persian)]. Iranian Journal of Nursing Research, 16(4), pp. 50-60. [Link]
Khajooee, R., et al., 2019. [Missed nursing care and its related factors from the points of view of nurses affiliated to Kerman University of Medical Sciences in 2017 (Persian)]. Hayat, 25(1), pp. 11-24. [Link]
Maghsoud, F., et al., 2022. Workload and quality of nursing care: the mediating role of implicit rationing of nursing care, job satisfaction and emotional exhaustion by using structural equations modeling approach. BMC Nursing, 21, pp. 273. [DOI:10.1186/s12912-022-01055-1] [PMID]
Mainz, H., et al., 2024. Prevalence of missed nursing care and its association with work experience: A cross-sectional survey. International Journal of Nursing Studies Advances, 6, pp. 100196. [DOI:10.1016/j.ijnsa.2024.100196] [PMID]
Mandal, L. & Seethalakshmi, A., 2023. Experience of missed nursing care: A mixed method study. Worldviews on Evidence‐Based Nursing, 20, pp. 212-9. [DOI:10.1111/wvn.12653] [PMID]
Moreno-Monsiváis, M. G., Moreno-Rodríguez, C. & Interial-Guzmán, M. G., 2015. Missed nursing care in hospitalized patients. Aquichan, 15, pp. 318-28. [DOI:10.5294/aqui.2015.15.3.2]
Orique, S. B., et al., 2017. Quantifying missed nursing care using the hospital consumer assessment of healthcare providers and systems (HCAHPS) survey. JONA: The Journal of Nursing Administration, 47, pp. 616-22. [DOI:10.1097/NNA.0000000000000556] [PMID]
Papathanasiou, I., et al., 2024. Missed nursing care; prioritizing the patient’s needs: An umbrella review. Healthcare, 224. [DOI:10.3390/healthcare12020224] [PMID]
Rahmani, P., et al., 2022. The relationship between attitude of nurses toward the patient safety and missed nursing care: A predictive study. Journal of Healthcare Quality Research, 37, pp. 138-46. [DOI:10.1016/j.jhqr.2021.10.007] [PMID]
Rajasekaran, J. J., et al., 2024. Oral microbiome: A review of its impact on oral and systemic health. Microorganisms, 12, pp. 1797. [DOI:10.3390/microorganisms12091797] [PMID]
Reynolds, S. S., et al., 2021. Results of the CHlorhexidine Gluconate Bathing implementation intervention to improve evidence-based nursing practices for prevention of central line associated bloodstream infections Study (CHanGing BathS): A stepped wedge cluster randomized trial. Implementation Science, 16, pp. 45. [DOI:10.1186/s13012-021-01112-4] [PMID]
Rezaee, S., Baljani, E. & Feizi, A., 2019. [Missed nursing care in educational, private and social welfare hospitals (Persian)]. Nursing and Midwifery Journal, 17(4), pp. 300-8. [Link]
Rezaee, S., et al., 2021. Reasons of missed nursing care from the viewpoints of nurses in educational, private, and social security hospitals in urmia-Iran in 2018. Preventive Care in Nursing & Midwifery Journal, 11, pp. 26-34. [DOI:10.52547/pcnm.11.4.26]
Rezaei-Shahsavarloo, Z., et al., 2021. Factors affecting missed nursing care in hospitalized frail older adults in the medical wards: A qualitative study. BMC Geriatrics, 21, pp. 1-12. [DOI:10.1186/s12877-021-02524-z] [PMID]
Stemmer, R., et al., 2022. A systematic review: Unfinished nursing care and the impact on the nurse outcomes of job satisfaction, burnout, intention-to-leave and turnover. Journal of Advanced Nursing, 78(8), pp. 2290–303. [DOI:10.1111/jan.15286] [PMID]
Southard, M. E., 2024. Professional nurse coach supervision: Relationships, responsibilities, and requirements. Journal of Holistic Nursing, 42, pp. 300-9. [DOI:10.1177/08980101231163675] [PMID]
Srulovici, E. & Yanovich, O. 2022. Missed nursing care: Testing the moderation‐mediation energetic and motivational pathways via a nested design. Journal of Advanced Nursing, 78, pp. 2339-48. [DOI:10.1111/jan.15144] [PMID]
Tai, C. H., Hsieh, T. C. & LEE, R. P., 2021. The effect of two bed bath practices in cost and vital signs of critically ill patients. International Journal of Environmental Research and Public Health, 18, pp. 816. [DOI:10.3390/ijerph18020816] [PMID]
Toney-Butler, T. J. & Thayer, J. M., 2023. Nursing process. In Statpearls [internet]. StatPearls Publishing. [Link]
Willis, E., et al., 2024. An integrative review of missed nursing care and the general practice nurse. Australian Journal of Primary Health, 30. [DOI:10.1071/PY23127] [PMID]
Yaghoubi, M., et al., 2019. [The relationship between teamwork and missed nursing care: Case study in a military hospital in Tehran (Persian)]. Journal of Military Medicine, 21(1), pp. 63-72. [Link]
Type of Study: Research |
Subject:
Special
Received: 2025/01/26 | Accepted: 2025/07/29 | Published: 2026/02/1
Received: 2025/01/26 | Accepted: 2025/07/29 | Published: 2026/02/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
