Tue, Aug 11, 2026
[Archive]
Volume 12, Issue 1 (Winter 2026)
JCCNC 2026, 12(1): 71-86 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ehwarieme T A, Josiah U, Abote M, Uzezi H. Evaluation of Nurses’ Knowledge and Utilization of Nonpharmacological Pain Management Techniques in Orthopedic Wards. JCCNC 2026; 12 (1) :71-86
URL: http://jccnc.iums.ac.ir/article-1-808-en.html
URL: http://jccnc.iums.ac.ir/article-1-808-en.html



1- Department of Nursing Science, University of Benin, Benin City, Nigeria. , timothy.ehwarieme@uniben.edu
2- Department of Nursing Science, Delta State University, Cleveland, United States.
3- University of Portsmouth, Portsmouth, England.
2- Department of Nursing Science, Delta State University, Cleveland, United States.
3- University of Portsmouth, Portsmouth, England.
Full-Text [PDF 761 kb]
(724 Downloads)
| Abstract (HTML) (790 Views)
Full-Text: (88 Views)
Introduction
Pain is a leading cause of hospital visits and hospitalization (Swartzentruber, 2021), and it can significantly affect a person’s quality of life (QoL) and hinder recovery from illness or injury. When unrelieved, pain can lead to a cycle of deterioration in health and outlook. Proper pain management not only supports rehabilitation but also reduces health risks and enhances overall QoL (Mohiuddin, 2019). Pain management is a critical component of patient care in orthopedic wards, particularly given the prevalence of postoperative pain and traumatic injuries (WHO, 2019). While pharmacological interventions are essential, nonpharmacological pain management (NPPM) techniques have gained recognition as effective complementary approaches (Smith et al., 2020). These methods help improve patient outcomes, reduce reliance on opioids and other analgesics, and promote overall wellbeing. Techniques such as relaxation therapy, distraction, massage, and guided imagery have been shown to alleviate pain and improve patient satisfaction (Kidanemariam et al., 2020).
Recent studies have underscored the benefits and challenges of such methods. Niyonkuru et al. (2025) demonstrated that interventions like preoperative education, mind-body techniques, and physical therapies effectively reduce postoperative pain, minimize opioid use, and enhance recovery outcomes. However, workload pressures and insufficient training remain barriers to consistent application. Similarly, Bhoi et al. (2021) noted that musculoskeletal diseases are a common source of chronic pain and disability. While complementary and alternative medicine (CAM) modalities, such as acupuncture, yoga, and herbal remedies, improve daily functioning when combined with conventional care, their effectiveness is variable and largely supportive rather than curative. In a systematic review, Bakker et al. (2020) reported mixed evidence, with some studies showing reduced pain and opioid use following CAM interventions. Nonetheless, heterogeneity and methodological limitations meant there was insufficient evidence to firmly establish CAM as a postoperative pain management alternative.
From the nursing perspective, Tsegaye et al. (2023) found that less than half (48.1%) of nurses in Ethiopia demonstrated good practice in NPPM, with utilization influenced by access to pain assessment tools, favorable attitudes, and younger age groups. Likewise, Kia et al. (2021) observed moderate use (55.8%) of such methods among intensive care unite (ICU) nurses in Iran, with repositioning being the most common. Barriers such as nurse fatigue, multiple responsibilities, and inadequate staffing limited broader use, while demographic factors showed little influence. A qualitative inquiry by Abuijlan et al. (2023) further highlighted nurses’ lived experiences, revealing that NPPM requires constant monitoring, careful selection of techniques, and collaboration across healthcare teams. Nurses also identified barriers stemming from both patient-related and organizational factors, calling for inter-professional teamwork and clearer role definitions to improve practice.
In Ethiopia, a 2018 study found that most nurses rely heavily on pharmacological approaches for pain management (Zeleke et al., 2018). In Nigeria, similar trends have been documented. At two hospitals in Ibadan, nurses displayed awareness of nonpharmacological methods, yet this awareness did not consistently translate into practice. The study found that limited knowledge of NPPM’s importance and effectiveness, coupled with attitude gaps, hindered its actual use (Ogunfowokan & Taiwo, 2021). In Benin City, an evaluation of nurses revealed that while relaxation techniques were the most commonly used nonpharmacological intervention, prescription medications remained the predominant method of pain management (Akpojaro et al., 2024).
Additionally, at Aminu Kano Teaching Hospital in the north, even though 94% of nurses were aware of nonpharmacological strategies, their adoption was not widespread. Many continued to rely heavily on pharmacological approaches, indicating a disconnect between knowledge and routine practice (Umar et al., 2023). Overall, these studies consistently show that nonpharmacological interventions are beneficial in reducing pain, limiting opioid reliance, and improving patient outcomes. However, their utilization remains suboptimal due to inadequate training, workload pressures, limited awareness, and organizational barriers (Zeleke et. al., 2021).
Building on this, further evidence highlights a persistent gap in nurses’ knowledge and utilization of NPPM strategies, particularly in orthopedic wards. A systematic review by Rasheed et al. (2019) found that nurses often lack awareness and understanding of these methods, which hinders their effective integration into patient care. Furthermore, a survey by Smith et al. (2020) found that nurses often reported limited training and education on nonpharmacological strategies, leading to low confidence in their use. Several studies have emphasized the importance of education and training in enhancing nurses’ practices concerning NPPM. For instance, Simsek and Gozen (2021) revealed that 60.5% of nurses had average knowledge of these methods, and 51.7% exhibited a positive attitude, suggesting room for improvement through training. Geleto et al. (2021) found that 54.2% of nurses in Ethiopia had adequate knowledge, and 49.8% had a favorable attitude. Factors such as education, years of experience, and nurse-patient ratios were significantly associated with knowledge and attitudes. Jira (2020) reported that 51.2% of nurses had adequate knowledge, and 47% had a positive attitude, with work experience, education level, and training courses being key contributors to improved practices. Studies from other regions have also highlighted challenges in utilizing nonpharmacological methods. Bayoumi (2021) found that, while cognitive-behavioral techniques such as distraction were frequently used in Egypt, barriers, including insufficient time, patient reluctance, and patient health beliefs, hindered broader adoption. Zeleke (2021) noted that in Ethiopia, many nurses reported poor adherence to NPPM, citing obstacles such as fatigue, insufficient physician collaboration, and inadequate nurse-patient ratios. Similarly, Ojo and Apata (2021) and Kimbi et al. (2016) found that nurses in Nigeria and Cameroon faced challenges, such as the lack of pain assessment tools and unfavorable attitudes, despite moderate rates of NPPM practice.
These similarities suggest that Nigeria mirrors the challenges of other African countries, such as Ethiopia, where, despite familiarity with and theoretical knowledge of nonpharmacological approaches, practical practices often skew towards pharmacological interventions. This condition underscores the need for enhanced training and education to deepen nurses’ understanding of nonpharmacological techniques, attitude-focused interventions to shift nursing perceptions and confidence toward these approaches, and practical implementation strategies that bridge the gap between knowledge and consistent utilization. Bringing in the knowledge-to-action (KTA) framework here could be particularly powerful, guiding transformation from knowledge awareness to sustained clinical change within Nigerian orthopedic wards.
The bio-psychosocial model by Engel (1977) highlights the multidimensional nature of pain and underscores the importance of addressing psychological and social aspects through non-drug approaches. In addition, Kolcaba’s Comfort Theory (1994) aligns with nursing practice by emphasizing holistic care and comfort promotion, thereby justifying nurses’ central role in applying these strategies in orthopedic wards. Building on these perspectives, this study was anchored in the KTA framework developed by Graham et al. (2006), which provides a practical lens for understanding and addressing persistent gaps in nurses’ knowledge, and the framework emphasizes a cyclical process that begins with knowledge creation. In this context, knowledge of evidence-based NPPM techniques progresses through the action cycle, which involves adapting this knowledge to the clinical setting, implementing it in practice, monitoring its use, and sustaining its application over time. Applying the KTA framework to this study allows for the examination not only of nurses’ knowledge levels but also of the extent to which this knowledge is translated into actual use in orthopedic wards. It also highlights the importance of identifying barriers and facilitators within the healthcare environment that influence the movement from knowledge to sustained practice.
Within this content, despite growing recognition of the benefits of NPPM, there remains a significant knowledge and implementation gap among nurses in orthopedic wards. Addressing this gap is crucial for improving patient outcomes and promoting holistic pain management; therefore, guided by the KTA framework, this research aims to assess the current state of knowledge and utilization of NPPM strategies, along with associated factors, among nurses in orthopedic wards at selected hospitals in Benin City.
Materials and Methods
Design, setting, and sample
This study used a cross-sectional descriptive design to gather and analyze data, allowing respondents to express their feelings freely. The study was conducted among registered nurses working in orthopedic wards at the University of Benin Teaching Hospital (UBTH)and Edo Specialist Hospital, both located in Benin City, Edo State, Nigeria. UBTH is a tertiary healthcare facility that provides both secondary and tertiary care, and also serves as a training center for health professionals and researchers. It has three orthopedic wards (male, female, and pediatric) with a total of 96 nurses assigned to these units. Edo Specialist Hospital, a central hospital with over 200 beds, is managed by a private healthcare consultant. It offers a broad range of services, including intensive care, cardiology, dermatology, and orthopedic care. The hospital also has three orthopedic wards: Male, female, and pediatric, with a total of 104 nurses. In total, 200 nurses work in the orthopedic wards at both facilities.
The sample size was determined using Yamane’s Equation (1967) (Equation 1) at a confidence level of 95% and margin of error of 0.05 as cited by Althubaiti (2022):
1. n=N/1+N(e)2
, with a 10% attrition rate, the total sample size was estimated at 146 nurses.
Proportional to size sampling was used. This sampling method is used in survey research where the probability of selecting a unit (e.g. a hospital, ward, or community) is proportional to its size in the population. Accordingly, 70 and 76 nurses were recruited from UBTH and Edo Specialist Hospital, respectively.
Inclusion criteria
The study included registered nurses with valid licenses who had at least 6 months of experience working in orthopedic wards, were currently employed in the orthopedic units of the UBTH or Edo Specialist Hospital, and willingly consented to participate.
Instrument for data collection
The research tools were developed through a combination of literature review, adaptation of validated instruments, and expert input to ensure contextual relevance to the study setting.
Literature review and source instruments
A comprehensive literature review was conducted using databases such as PubMed, CINAHL, and Google Scholar to identify previously validated tools related to nurses’ knowledge, practices, and perceived barriers in pain management. The knowledge assessment questionnaire (section B) drew on items from the nurses’ knowledge and attitudes survey regarding pain developed by Ferrell and McCaffery (2014), with modifications to reflect orthopedic-specific pain management scenarios. The pain management practice checklist (section c) was informed by clinical audit tools and observational checklists used in studies on pain management in surgical and orthopaedic settings (Bernardi et al., 2007; Chatchumni et al., 2016a; Chatchumni et al., 2016b). The barriers to pain management questionnaire (section D) was adapted from barrier-assessment frameworks used in previous studies on institutional, patient-related, and nurse-related obstacles to optimal pain control (Al Qadire & Al Khalaileh, 2014).
Contextual adaptation
Items from source instruments were reviewed and adapted to match the Nigerian healthcare setting, with particular attention to the realities of the University of Benin Teaching Hospital and Edo Specialist Hospital. Terminology was localized, examples were drawn from experiences in the orthopedic ward, and questions were adjusted to account for available medications, resources, and common cultural attitudes toward pain. This condition gives rise to the following, as described below.
Section A collects demographic data, including age, sex, tribe, highest level of education, years of service, and professional ranking and ward. It consists of 8 closed-ended questions. Section B evaluates participants’ knowledge of NPPM strategies through 15 closed-ended multiple-choice questions. Each correct answer earns 2 marks. Results are categorized as poor (0-9), moderate (10-20), or good (21-30). Section C assesses the use of NPPM strategies, consisting of 15 closed-ended questions. A 4-point Likert scale (always, sometimes, rarely, never) is used, with scores ranging from 1 (never) to 4 (always). Higher scores indicate greater use of NPPM strategies. Section D identifies barriers to the use of NPPM strategies in the wards, comprising 12 closed-ended questions. A 5-point Likert scale (1-5) is used to assess the importance of various barriers, with 5 indicating the highest importance.
Validity and reliability
The research instruments underwent a thorough validation process. Face validity was assessed by experts in Orthopedics/Trauma and Orthopedics Nursing, who reviewed the instruments for clarity and relevance and suggested corrections, which the researcher subsequently implemented. The content validity of the tools was reviewed by a panel of 5 experts, including 2 orthopedic nursing specialists, 1 pain management consultant, and 2 nursing educators. The panel evaluated the tools for relevance, clarity, comprehensiveness, and alignment with the study objectives. The content validity index (CVI) was used, and items with a score ≥0.8 were retained. A split-half reliability test was conducted with 15 nurses (10% of the sample) at another hospital using the research instrument. Internal consistency was assessed using the Cronbach α to compute the reliability coefficient. The reliability scores obtained for sections B, C, and D were 0.85, 0.88, and 0.75, respectively, indicating satisfactory consistency
Data collection procedure
Nurses who met the inclusion criteria were identified and approached personally at their respective hospital wards. The purpose of the study was explained to each participant, and they were shown the consent form before being invited to participate. Nurses who agreed to take part were provided with a questionnaire to complete privately. Data were collected at times that did not interfere with the nurses’ routine duties, such as during shift changes, break periods, or immediately after duty hours. The researcher personally retrieved the completed questionnaires and stored them in sealed envelopes to ensure confidentiality. Data collection lasted for one month.
Data analysis
Data were collated, entered into a Microsoft Excel spreadsheet, and analyzed using SPSS software, version 24.0. The normality of the variables was assessed using the Shapiro-Wilk test, as it is suitable for small to medium sample sizes. A P value greater than 0.05 indicated that the data were normally distributed (in this study, the P value was 0.067). Descriptive and inferential statistical analyses were employed. Multivariate logistic regression was used to assess the significance of the variables at the 5% level.
Results
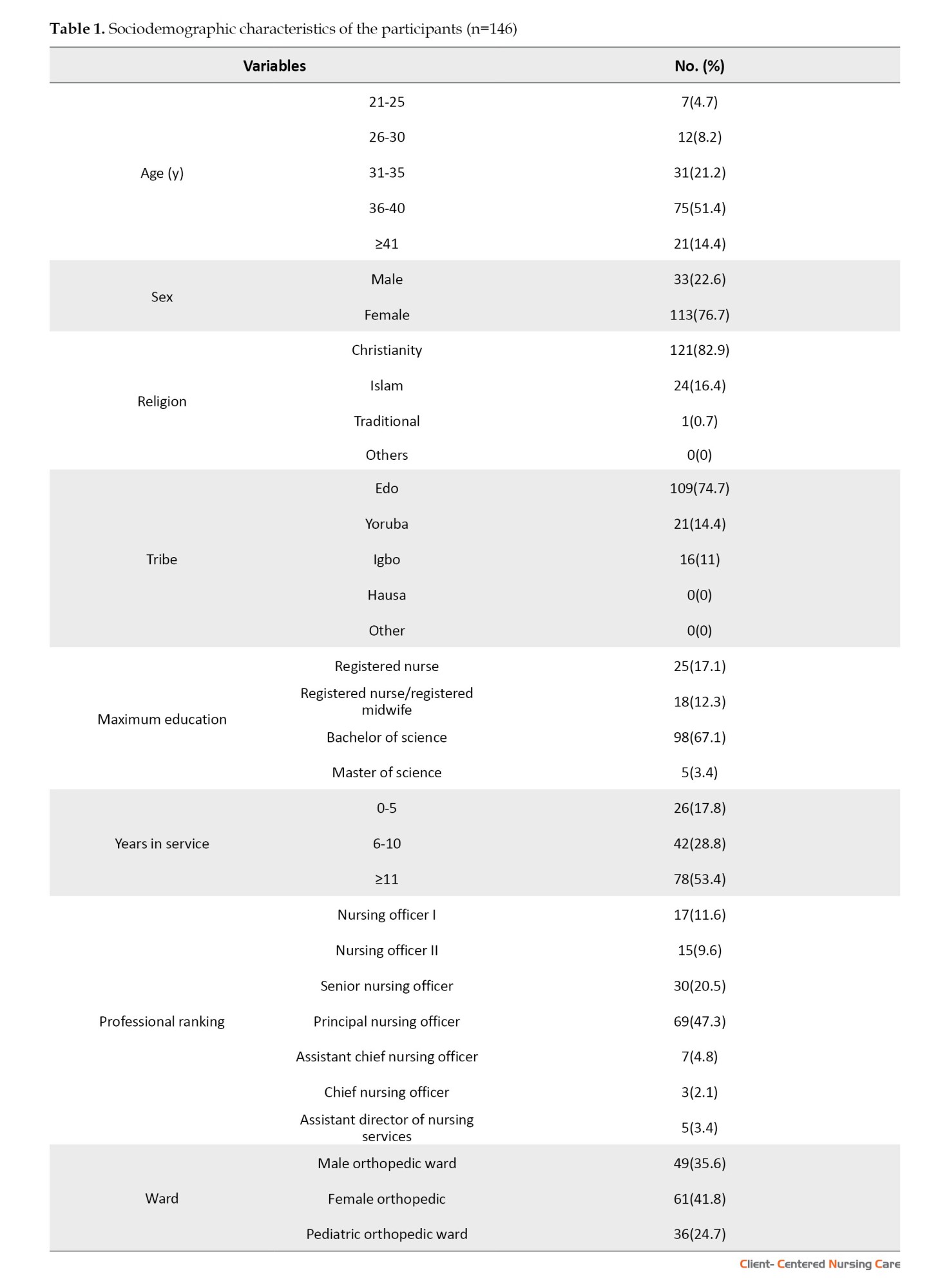
The demographic characteristics of the study participants revealed that the majority were aged 36 to 40 years (51.4%), with a larger proportion being female (76.7%). Most participants identified as Christians (82.9%) and were from the Edo tribe (74.7%). Regarding education, 67.1% had a Bachelor’s degree, while 53.4% had 11 or more years of experience. In terms of professional ranking, 47.3% were principal nursing officers, and 41.8% worked in the Female Orthopedic Department (Table 1).
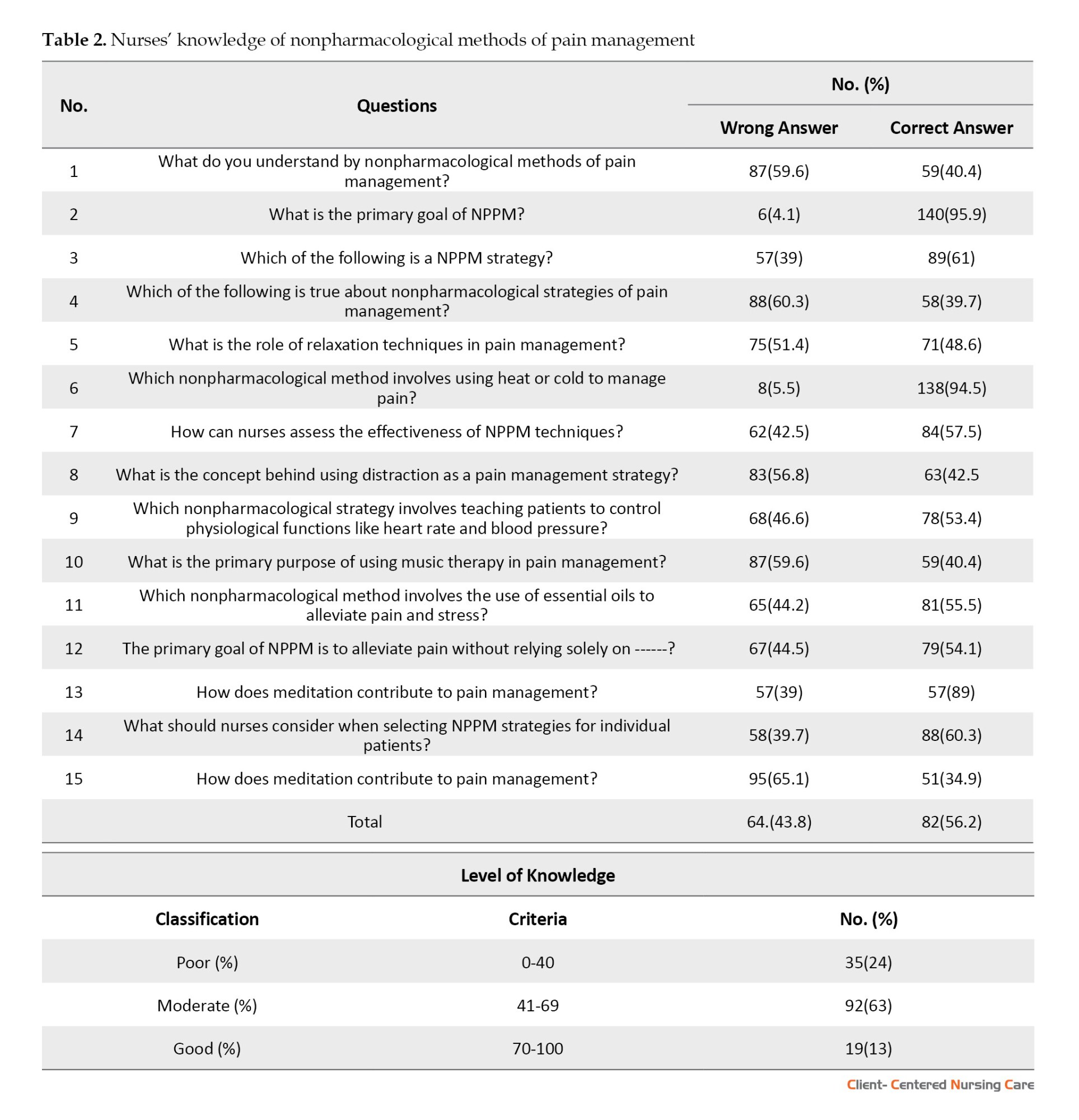
The findings revealed varying levels of knowledge among nurses regarding NPPM. While most nurses recognized the primary goal of these methods, only about half understood key techniques like relaxation and distraction. Knowledge was higher for methods such as heat/cold therapy and meditation, but moderate for biofeedback, music therapy, and essential oils. Although many nurses acknowledged the importance of patient preferences, fewer understood how meditation aids pain relief. Overall, 24% had poor knowledge, 63% had moderate knowledge, and only 13% had good knowledge of NPPM (Table 2).
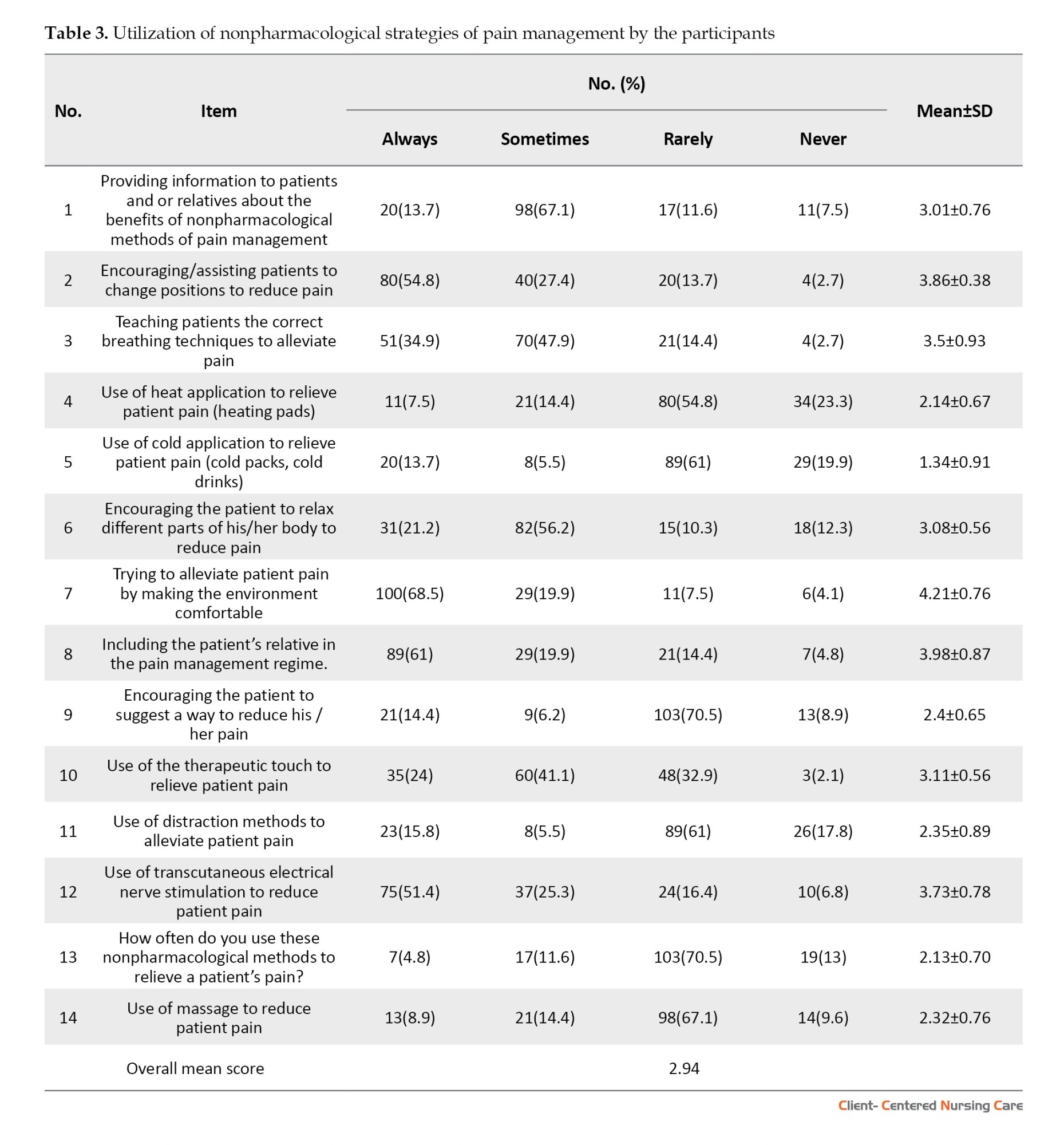
The findings showed varying levels of utilization of NPPM methods among nurses. Frequently used strategies included patient education, position changes, breathing techniques to ensure comfort, and involving relatives. Moderately used methods included relaxation, therapeutic touch, and electrical nerve stimulation. Less commonly practiced techniques included heat and cold application, distraction, and massage. While most nurses (76.7%) used these methods occasionally, only 15.1% applied them consistently. Considering that the instrument items range from 1 to 4 and the average total response is 2.94, the use of non-NPPM methods was generally moderate (Table 3).
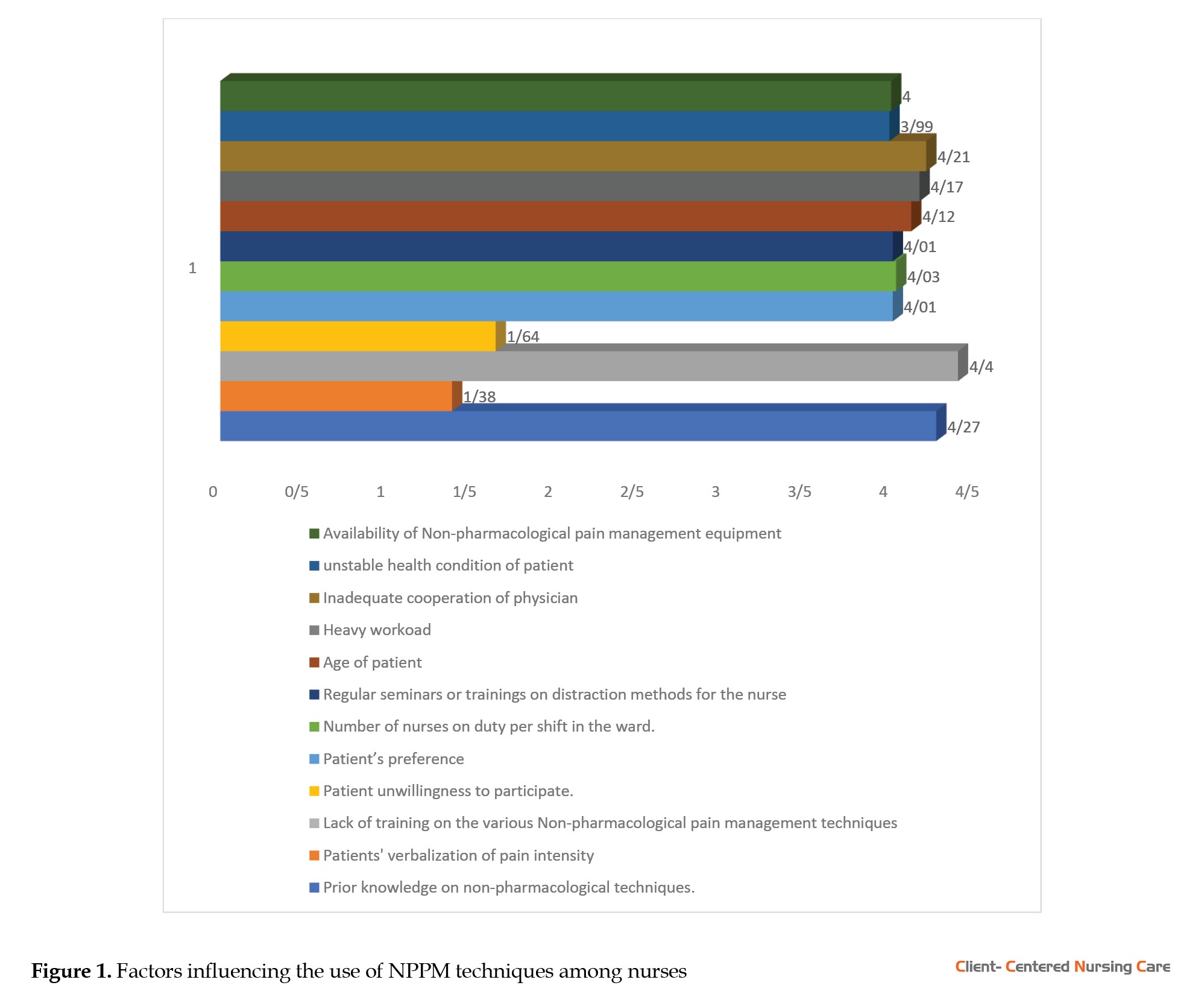
The findings showed that a lack of training, limited prior knowledge, heavy workload, inadequate physician cooperation, and patient age mainly influenced nurses’ use of NPPM methods. Other factors such as staffing levels, equipment availability, and patient preferences also played a role (Figure 1).
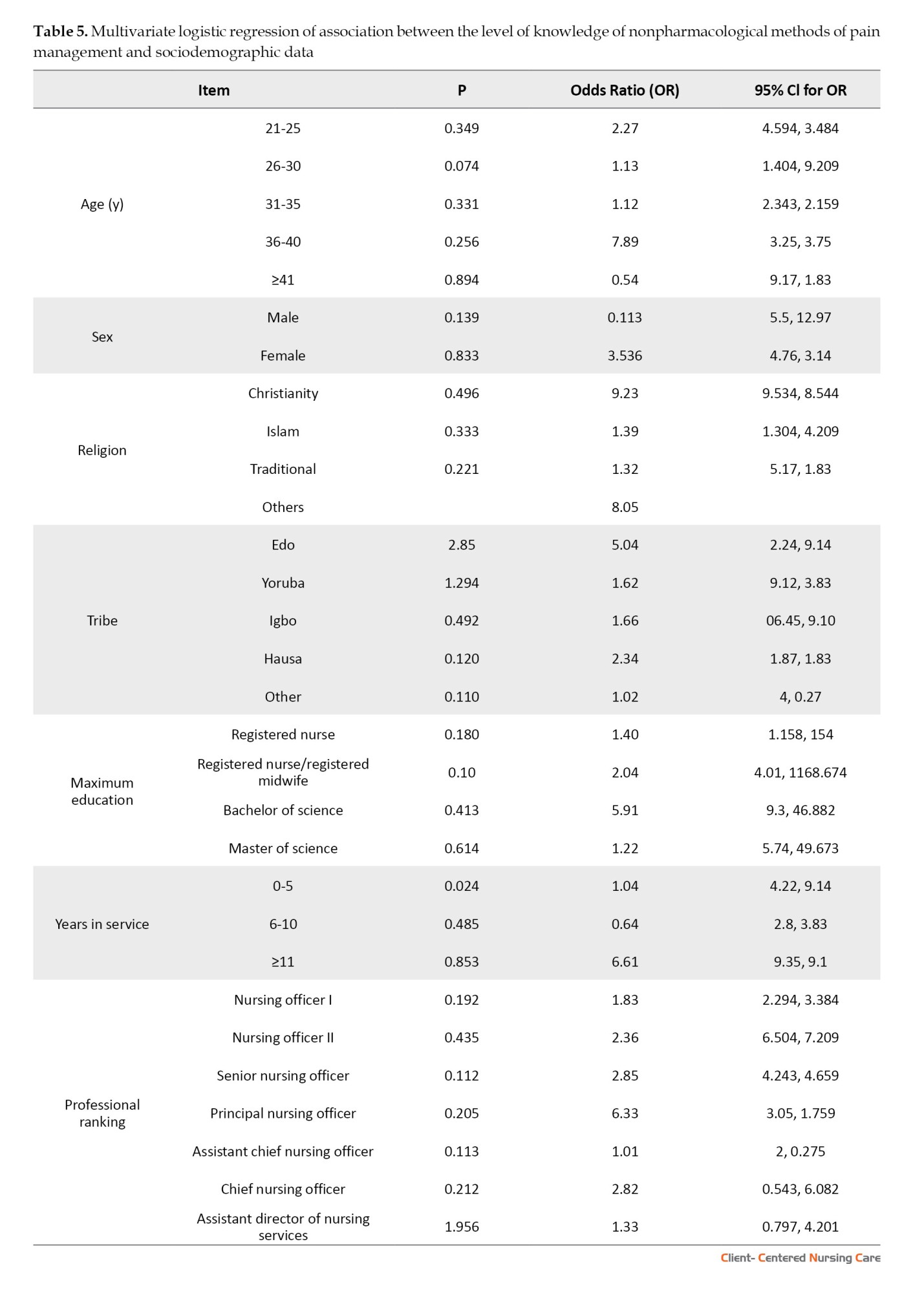
The association between knowledge of nonpharmacological methods of pain management and sociodemographic variables is summarized below. Nurses aged 36-40 years are 7 times more likely to know NPPM methods than others. Females are 4 times more likely than males to have knowledge of NPPM methods. Christians are 9 times more likely to have knowledge about NPPM methods than non-Christians. Nurses from the Edo tribe are 5 times more likely to have knowledge of NPPM methods than others. Nurses with a Bachelor’s degree are 6 times more likely to have knowledge of NPPM methods than those with lower qualifications. Nurses with 11 or more years of service are 7 times more likely to have knowledge about NPPM methods than those with less experience. Principal Nursing Officers are 6 times more likely than other professional ranks to know NPPM methods (Table 5).
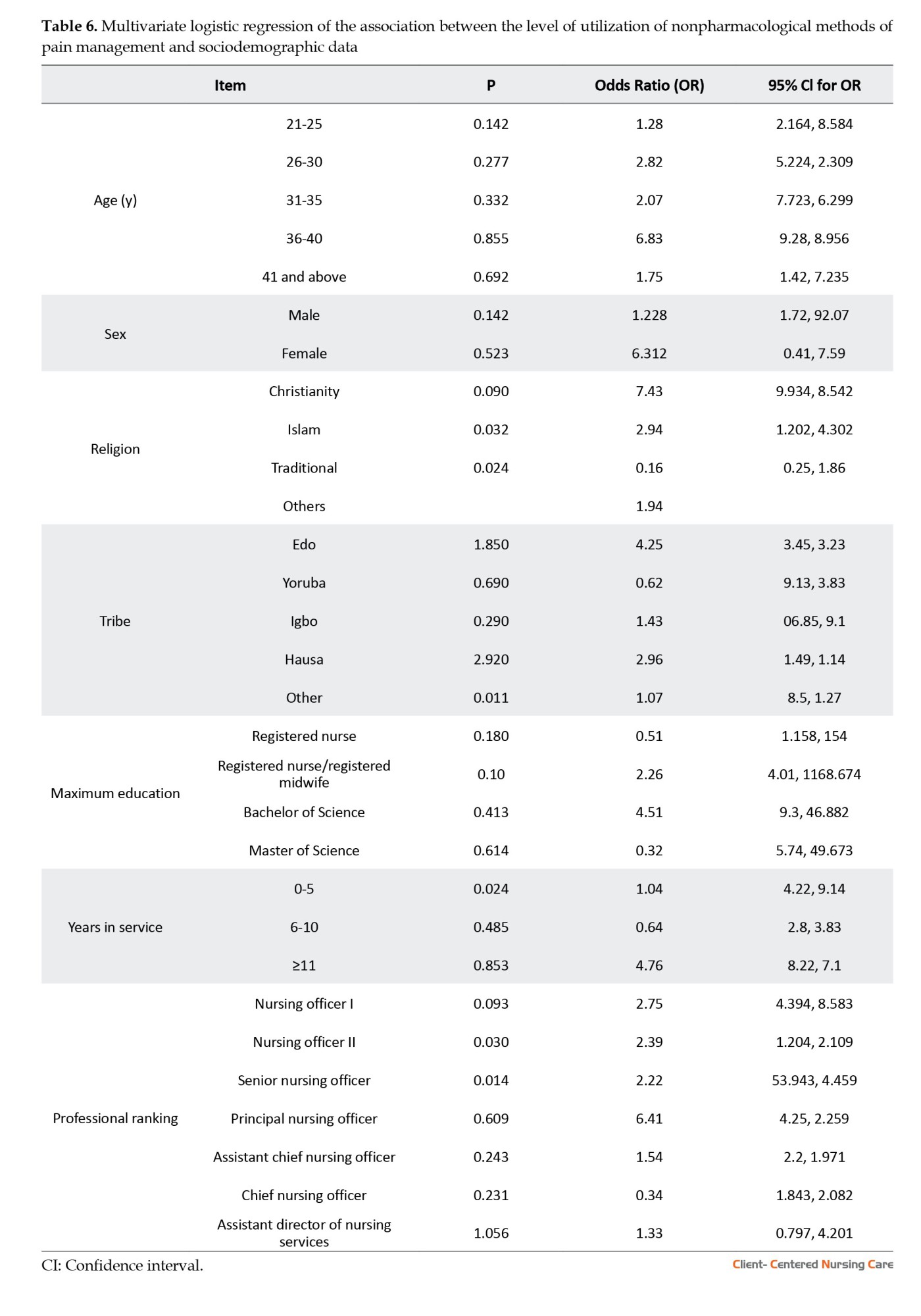
The association between the level of utilisation of NPPM methods and sociodemographic variables is summarized in Table 6. Nurses aged 36-40 years are 7 times more likely to utilise NPPM methods than other age groups. Females are 6 times more likely than males to practice NPPM methods. Christians are 7 times more likely to utilise NPPM methods compared to non-Christians. Nurses who are Edo are 4 times more likely to use NPPM methods than others. Nurses with a Bachelor’s degree are 5 times more likely to utilise NPPM methods than those with lower qualifications. Nurses with 11 or more years of service are 4 times more likely to use NPPM methods than those with less experience. Finally, Principal Nursing Officers are 6 times more likely to utilise NPPM methods than others (Table 6).
Discussion
The findings of this study reveal that the majority of nurses had moderate knowledge of NPPM strategies, suggesting a need to improve understanding and application of these methods. While the majority of nurses could identify specific strategies, such as heat or cold, fewer demonstrated a comprehensive understanding of general principles, relaxation techniques, or the purpose of music therapy. The findings indicate variability in knowledge, with specific techniques such as heat or cold and essential oils being better understood than more complex methods like distraction and biofeedback. The results are consistent with those of Manwere et al. (2015), who found that many nurses agreed on the effectiveness of distraction and other nonpharmacological interventions for mild to moderate pain. However, some gaps persist, as seen in the current study, in which only a minority had strong knowledge of general principles and advanced techniques such as biofeedback. This finding highlights the need for targeted educational interventions.
Jira et al. (2020) and Geleto et al. (2021) emphasized that factors such as education level, work experience, and nurse-to-patient ratios significantly influence knowledge and attitudes. In this study, moderate knowledge levels may also be attributed to similar factors, suggesting that enhancing educational programs and addressing systemic issues like workload could improve knowledge levels. Geleto’s findings also highlight the importance of income and working conditions in shaping attitudes, pointing to broader systemic reforms that could complement educational initiatives. Notably, studies by Mohamed et al. (2021) in Egypt and Elhusein et al. (2020) in Sudan found lower knowledge levels than this study, with reliance on pharmacological methods prevalent. The higher knowledge levels in this study may reflect differences in regional educational standards or access to resources. However, they still indicate room for growth, particularly in areas such as distraction and music therapy. The findings suggest a need to prioritize training programs focused on the principles and advanced techniques of NPPM. While nurses demonstrated strong knowledge of basic strategies such as heat or cold applications, their understanding of relaxation techniques, music therapy, and distraction as effective methods needs strengthening. Additionally, systemic factors like nurse-to-patient ratios, income, and work conditions, as noted in the literature, should be addressed to create an enabling environment for the adoption of these strategies. Incorporating NPPM into routine nursing curricula and continuing education programs could help bridge knowledge gaps and increase its utilization.
The study reveals moderate use of NPPM methods among nurses, with most using them occasionally and only a few consistently. Common practices, such as providing information to patients, encouraging position changes, teaching breathing techniques, and creating a comfortable environment, are widely used because of their simplicity and effectiveness. However, less frequently used methods, including heat and cold application, distraction, and massage, highlight gaps in training, knowledge, or accessibility. These findings align with those of Karabulut and Yaman (2016), who observed limited use of nonpharmacological techniques such as distraction and massage among Turkish nursing students, underscoring the need for curriculum updates. Similarly, Tirgari et al. (2018) noted moderate repositioning use among Iranian ICU nurses, with barriers, including fatigue, workload, and insufficient staffing. In Ethiopia, Tsegaye et al. (2020) reported that 48.1% of nurses practiced NPPM, emphasizing the role of training and pain assessment tools in improving utilization rates. Comparable barriers, such as time constraints and patient reluctance, were highlighted by Bayoumi (2021) in Egypt, which reflects the low use of distraction techniques in the current study. Systemic challenges, including nurse fatigue, poor interprofessional collaboration, and high nurse-to-patient ratios, were also noted by Tsegaye et al. (2023) in Ethiopia and Tabrizi et al. (2023) in Iran. These issues mirror findings in this study, which found that organizational obstacles hinder the consistent application of advanced techniques. Ojo and Apata (2021) and Nwaneri et al. (2018) in Nigeria, along with Kimbi et al. (2016) in Cameroon, reported moderate use of NPPM methods, with barriers, including a lack of pain assessment tools, insufficient staffing, and limited awareness. Resource availability further impacts implementation, as noted by Ojo and Apata (2021) and Khalil (2018), highlighting the need for investment in specialized equipment. Patient-related barriers, such as preferences for pharmacological methods and reluctance to participate, were also identified, aligning with Sisay’s (2017) findings. Addressing these challenges through targeted training, awareness campaigns, and patient education is critical. Recommendations from Gumus et al. (2020) and Kimbi et al. (2016) emphasize the importance of in-service training and interprofessional collaboration to enhance the adoption of NPPM practices.
The findings reveal that sociodemographic factors, including age, gender, educational qualifications, years of service, and professional rank, significantly influence nurses’ knowledge of NPPM methods. Nurses aged 36–40 years were found to be 7 times more likely to have knowledge of these techniques than their younger or older counterparts. This finding is consistent with findings from Tsegaye et al. (2023), who noted that middle-aged nurses often demonstrate higher knowledge levels due to their cumulative work experience and greater exposure to training opportunities. Female nurses were 4 times more likely than male nurses to know NPPM methods. This finding aligns with the study by Taylor et al. (2018), which highlighted gender differences in healthcare practice, where female nurses often had greater involvement in patient care, potentially increasing their familiarity with such methods. Educational qualifications were another significant factor: Nurses with a Bachelor’s degree were 6 times more likely to possess knowledge than those with lower qualifications. This finding supports those of Soriano et al. (2025) and Tsegaye et al. (2022), who identified higher education as a strong predictor of knowledge, due to more comprehensive training, including exposure to NPPM strategies. Experience also plays a crucial role, as nurses with 11 or more years of service were 7 times more likely to demonstrate knowledge than their less experienced counterparts. This finding aligns with Bayoumi (2021), who observed that longer service durations allow nurses to gain practical exposure and refine their understanding of pain management. Lastly, professional rank was significant, with Principal Nursing Officers being 6 times more likely to know nurses in lower ranks. This finding is consistent with Nwaneri et al. (2018), who noted that senior-ranking nurses are often involved in policy-making and training programs, enhancing their expertise and familiarity with advanced pain management strategies.
This study had some limitations. The cross-sectional nature of the study limits the ability to establish causal relationships between factors such as training, experience, and knowledge. Reliance on self-reported data introduces the potential for bias, as participants may over- or under-estimate their knowledge or use of nonpharmacological methods. A small sample size and limited geographic scope may restrict the generalizability of findings to a broader population of nurses or healthcare settings. The absence of objective assessments, such as patient outcomes or direct observation of practices, reduces the accuracy of nurse practice evaluations.
Implication to nursing
The study’s findings have significant implications for nursing practice. NPPM approaches in nursing curricula and ongoing professional development are essential to equip nurses with the necessary skills and knowledge. Establishing standardized protocols and guidelines can ensure consistent application across healthcare settings. Mentorship programs, where experienced nurses guide less experienced colleagues, can bridge knowledge gaps, particularly for nurses with fewer years of service. Addressing staffing challenges, such as ensuring adequate staff levels and manageable workloads, is critical for enabling nurses to implement these methods effectively. Tailored training programs for less experienced nurses, those in lower professional ranks, or male nurses can improve their familiarity with these methods. Enhanced collaboration between nurses and physicians is also crucial for the wider acceptance and implementation of NPPM strategies. Lastly, patient preferences and conditions should be considered when selecting the most appropriate pain management strategies, ensuring optimal outcomes for each patient.
Conclusion
In conclusion, the study emphasizes the significant role of NPPM approaches and techniques in nursing practice. It highlights that factors such as training, experience, and professional rank influence nurses’ knowledge and utilization of these methods. While experienced nurses tend to demonstrate better knowledge, the study underscores the need for targeted education, mentorship, and the development of standardized protocols to enhance the application of NPPM strategies across all nursing levels. Addressing systemic barriers, such as staffing issues and physician collaboration, is also crucial to improving the consistent use of these methods, ultimately leading to better patient outcomes.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of the University of Benin, Benin City, Nigeria (Code: ADM/22/A/VOL.VII14865502), and consent and permission were obtained from the participants. In addition, formal permission to conduct the study was obtained from the management of the relevant hospitals before data collection commenced. Other ethical principles, such as confidentiality and voluntary withdrawal, were strictly adhered to.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and study design: Timothy Aghogho Ehwarieme; Data collection, data analysis, review and editing: Uzezi Josiah; Writing the original draft: Timothy Aghogho Ehwarieme and Mabel Abote; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors appreciate the University of Benin, the management of the relevant hospitals, and the participants for their contribution to the study.
References
Pain is a leading cause of hospital visits and hospitalization (Swartzentruber, 2021), and it can significantly affect a person’s quality of life (QoL) and hinder recovery from illness or injury. When unrelieved, pain can lead to a cycle of deterioration in health and outlook. Proper pain management not only supports rehabilitation but also reduces health risks and enhances overall QoL (Mohiuddin, 2019). Pain management is a critical component of patient care in orthopedic wards, particularly given the prevalence of postoperative pain and traumatic injuries (WHO, 2019). While pharmacological interventions are essential, nonpharmacological pain management (NPPM) techniques have gained recognition as effective complementary approaches (Smith et al., 2020). These methods help improve patient outcomes, reduce reliance on opioids and other analgesics, and promote overall wellbeing. Techniques such as relaxation therapy, distraction, massage, and guided imagery have been shown to alleviate pain and improve patient satisfaction (Kidanemariam et al., 2020).
Recent studies have underscored the benefits and challenges of such methods. Niyonkuru et al. (2025) demonstrated that interventions like preoperative education, mind-body techniques, and physical therapies effectively reduce postoperative pain, minimize opioid use, and enhance recovery outcomes. However, workload pressures and insufficient training remain barriers to consistent application. Similarly, Bhoi et al. (2021) noted that musculoskeletal diseases are a common source of chronic pain and disability. While complementary and alternative medicine (CAM) modalities, such as acupuncture, yoga, and herbal remedies, improve daily functioning when combined with conventional care, their effectiveness is variable and largely supportive rather than curative. In a systematic review, Bakker et al. (2020) reported mixed evidence, with some studies showing reduced pain and opioid use following CAM interventions. Nonetheless, heterogeneity and methodological limitations meant there was insufficient evidence to firmly establish CAM as a postoperative pain management alternative.
From the nursing perspective, Tsegaye et al. (2023) found that less than half (48.1%) of nurses in Ethiopia demonstrated good practice in NPPM, with utilization influenced by access to pain assessment tools, favorable attitudes, and younger age groups. Likewise, Kia et al. (2021) observed moderate use (55.8%) of such methods among intensive care unite (ICU) nurses in Iran, with repositioning being the most common. Barriers such as nurse fatigue, multiple responsibilities, and inadequate staffing limited broader use, while demographic factors showed little influence. A qualitative inquiry by Abuijlan et al. (2023) further highlighted nurses’ lived experiences, revealing that NPPM requires constant monitoring, careful selection of techniques, and collaboration across healthcare teams. Nurses also identified barriers stemming from both patient-related and organizational factors, calling for inter-professional teamwork and clearer role definitions to improve practice.
In Ethiopia, a 2018 study found that most nurses rely heavily on pharmacological approaches for pain management (Zeleke et al., 2018). In Nigeria, similar trends have been documented. At two hospitals in Ibadan, nurses displayed awareness of nonpharmacological methods, yet this awareness did not consistently translate into practice. The study found that limited knowledge of NPPM’s importance and effectiveness, coupled with attitude gaps, hindered its actual use (Ogunfowokan & Taiwo, 2021). In Benin City, an evaluation of nurses revealed that while relaxation techniques were the most commonly used nonpharmacological intervention, prescription medications remained the predominant method of pain management (Akpojaro et al., 2024).
Additionally, at Aminu Kano Teaching Hospital in the north, even though 94% of nurses were aware of nonpharmacological strategies, their adoption was not widespread. Many continued to rely heavily on pharmacological approaches, indicating a disconnect between knowledge and routine practice (Umar et al., 2023). Overall, these studies consistently show that nonpharmacological interventions are beneficial in reducing pain, limiting opioid reliance, and improving patient outcomes. However, their utilization remains suboptimal due to inadequate training, workload pressures, limited awareness, and organizational barriers (Zeleke et. al., 2021).
Building on this, further evidence highlights a persistent gap in nurses’ knowledge and utilization of NPPM strategies, particularly in orthopedic wards. A systematic review by Rasheed et al. (2019) found that nurses often lack awareness and understanding of these methods, which hinders their effective integration into patient care. Furthermore, a survey by Smith et al. (2020) found that nurses often reported limited training and education on nonpharmacological strategies, leading to low confidence in their use. Several studies have emphasized the importance of education and training in enhancing nurses’ practices concerning NPPM. For instance, Simsek and Gozen (2021) revealed that 60.5% of nurses had average knowledge of these methods, and 51.7% exhibited a positive attitude, suggesting room for improvement through training. Geleto et al. (2021) found that 54.2% of nurses in Ethiopia had adequate knowledge, and 49.8% had a favorable attitude. Factors such as education, years of experience, and nurse-patient ratios were significantly associated with knowledge and attitudes. Jira (2020) reported that 51.2% of nurses had adequate knowledge, and 47% had a positive attitude, with work experience, education level, and training courses being key contributors to improved practices. Studies from other regions have also highlighted challenges in utilizing nonpharmacological methods. Bayoumi (2021) found that, while cognitive-behavioral techniques such as distraction were frequently used in Egypt, barriers, including insufficient time, patient reluctance, and patient health beliefs, hindered broader adoption. Zeleke (2021) noted that in Ethiopia, many nurses reported poor adherence to NPPM, citing obstacles such as fatigue, insufficient physician collaboration, and inadequate nurse-patient ratios. Similarly, Ojo and Apata (2021) and Kimbi et al. (2016) found that nurses in Nigeria and Cameroon faced challenges, such as the lack of pain assessment tools and unfavorable attitudes, despite moderate rates of NPPM practice.
These similarities suggest that Nigeria mirrors the challenges of other African countries, such as Ethiopia, where, despite familiarity with and theoretical knowledge of nonpharmacological approaches, practical practices often skew towards pharmacological interventions. This condition underscores the need for enhanced training and education to deepen nurses’ understanding of nonpharmacological techniques, attitude-focused interventions to shift nursing perceptions and confidence toward these approaches, and practical implementation strategies that bridge the gap between knowledge and consistent utilization. Bringing in the knowledge-to-action (KTA) framework here could be particularly powerful, guiding transformation from knowledge awareness to sustained clinical change within Nigerian orthopedic wards.
The bio-psychosocial model by Engel (1977) highlights the multidimensional nature of pain and underscores the importance of addressing psychological and social aspects through non-drug approaches. In addition, Kolcaba’s Comfort Theory (1994) aligns with nursing practice by emphasizing holistic care and comfort promotion, thereby justifying nurses’ central role in applying these strategies in orthopedic wards. Building on these perspectives, this study was anchored in the KTA framework developed by Graham et al. (2006), which provides a practical lens for understanding and addressing persistent gaps in nurses’ knowledge, and the framework emphasizes a cyclical process that begins with knowledge creation. In this context, knowledge of evidence-based NPPM techniques progresses through the action cycle, which involves adapting this knowledge to the clinical setting, implementing it in practice, monitoring its use, and sustaining its application over time. Applying the KTA framework to this study allows for the examination not only of nurses’ knowledge levels but also of the extent to which this knowledge is translated into actual use in orthopedic wards. It also highlights the importance of identifying barriers and facilitators within the healthcare environment that influence the movement from knowledge to sustained practice.
Within this content, despite growing recognition of the benefits of NPPM, there remains a significant knowledge and implementation gap among nurses in orthopedic wards. Addressing this gap is crucial for improving patient outcomes and promoting holistic pain management; therefore, guided by the KTA framework, this research aims to assess the current state of knowledge and utilization of NPPM strategies, along with associated factors, among nurses in orthopedic wards at selected hospitals in Benin City.
Materials and Methods
Design, setting, and sample
This study used a cross-sectional descriptive design to gather and analyze data, allowing respondents to express their feelings freely. The study was conducted among registered nurses working in orthopedic wards at the University of Benin Teaching Hospital (UBTH)and Edo Specialist Hospital, both located in Benin City, Edo State, Nigeria. UBTH is a tertiary healthcare facility that provides both secondary and tertiary care, and also serves as a training center for health professionals and researchers. It has three orthopedic wards (male, female, and pediatric) with a total of 96 nurses assigned to these units. Edo Specialist Hospital, a central hospital with over 200 beds, is managed by a private healthcare consultant. It offers a broad range of services, including intensive care, cardiology, dermatology, and orthopedic care. The hospital also has three orthopedic wards: Male, female, and pediatric, with a total of 104 nurses. In total, 200 nurses work in the orthopedic wards at both facilities.
The sample size was determined using Yamane’s Equation (1967) (Equation 1) at a confidence level of 95% and margin of error of 0.05 as cited by Althubaiti (2022):
1. n=N/1+N(e)2
, with a 10% attrition rate, the total sample size was estimated at 146 nurses.
Proportional to size sampling was used. This sampling method is used in survey research where the probability of selecting a unit (e.g. a hospital, ward, or community) is proportional to its size in the population. Accordingly, 70 and 76 nurses were recruited from UBTH and Edo Specialist Hospital, respectively.
Inclusion criteria
The study included registered nurses with valid licenses who had at least 6 months of experience working in orthopedic wards, were currently employed in the orthopedic units of the UBTH or Edo Specialist Hospital, and willingly consented to participate.
Instrument for data collection
The research tools were developed through a combination of literature review, adaptation of validated instruments, and expert input to ensure contextual relevance to the study setting.
Literature review and source instruments
A comprehensive literature review was conducted using databases such as PubMed, CINAHL, and Google Scholar to identify previously validated tools related to nurses’ knowledge, practices, and perceived barriers in pain management. The knowledge assessment questionnaire (section B) drew on items from the nurses’ knowledge and attitudes survey regarding pain developed by Ferrell and McCaffery (2014), with modifications to reflect orthopedic-specific pain management scenarios. The pain management practice checklist (section c) was informed by clinical audit tools and observational checklists used in studies on pain management in surgical and orthopaedic settings (Bernardi et al., 2007; Chatchumni et al., 2016a; Chatchumni et al., 2016b). The barriers to pain management questionnaire (section D) was adapted from barrier-assessment frameworks used in previous studies on institutional, patient-related, and nurse-related obstacles to optimal pain control (Al Qadire & Al Khalaileh, 2014).
Contextual adaptation
Items from source instruments were reviewed and adapted to match the Nigerian healthcare setting, with particular attention to the realities of the University of Benin Teaching Hospital and Edo Specialist Hospital. Terminology was localized, examples were drawn from experiences in the orthopedic ward, and questions were adjusted to account for available medications, resources, and common cultural attitudes toward pain. This condition gives rise to the following, as described below.
Section A collects demographic data, including age, sex, tribe, highest level of education, years of service, and professional ranking and ward. It consists of 8 closed-ended questions. Section B evaluates participants’ knowledge of NPPM strategies through 15 closed-ended multiple-choice questions. Each correct answer earns 2 marks. Results are categorized as poor (0-9), moderate (10-20), or good (21-30). Section C assesses the use of NPPM strategies, consisting of 15 closed-ended questions. A 4-point Likert scale (always, sometimes, rarely, never) is used, with scores ranging from 1 (never) to 4 (always). Higher scores indicate greater use of NPPM strategies. Section D identifies barriers to the use of NPPM strategies in the wards, comprising 12 closed-ended questions. A 5-point Likert scale (1-5) is used to assess the importance of various barriers, with 5 indicating the highest importance.
Validity and reliability
The research instruments underwent a thorough validation process. Face validity was assessed by experts in Orthopedics/Trauma and Orthopedics Nursing, who reviewed the instruments for clarity and relevance and suggested corrections, which the researcher subsequently implemented. The content validity of the tools was reviewed by a panel of 5 experts, including 2 orthopedic nursing specialists, 1 pain management consultant, and 2 nursing educators. The panel evaluated the tools for relevance, clarity, comprehensiveness, and alignment with the study objectives. The content validity index (CVI) was used, and items with a score ≥0.8 were retained. A split-half reliability test was conducted with 15 nurses (10% of the sample) at another hospital using the research instrument. Internal consistency was assessed using the Cronbach α to compute the reliability coefficient. The reliability scores obtained for sections B, C, and D were 0.85, 0.88, and 0.75, respectively, indicating satisfactory consistency
Data collection procedure
Nurses who met the inclusion criteria were identified and approached personally at their respective hospital wards. The purpose of the study was explained to each participant, and they were shown the consent form before being invited to participate. Nurses who agreed to take part were provided with a questionnaire to complete privately. Data were collected at times that did not interfere with the nurses’ routine duties, such as during shift changes, break periods, or immediately after duty hours. The researcher personally retrieved the completed questionnaires and stored them in sealed envelopes to ensure confidentiality. Data collection lasted for one month.
Data analysis
Data were collated, entered into a Microsoft Excel spreadsheet, and analyzed using SPSS software, version 24.0. The normality of the variables was assessed using the Shapiro-Wilk test, as it is suitable for small to medium sample sizes. A P value greater than 0.05 indicated that the data were normally distributed (in this study, the P value was 0.067). Descriptive and inferential statistical analyses were employed. Multivariate logistic regression was used to assess the significance of the variables at the 5% level.
Results
The demographic characteristics of the study participants revealed that the majority were aged 36 to 40 years (51.4%), with a larger proportion being female (76.7%). Most participants identified as Christians (82.9%) and were from the Edo tribe (74.7%). Regarding education, 67.1% had a Bachelor’s degree, while 53.4% had 11 or more years of experience. In terms of professional ranking, 47.3% were principal nursing officers, and 41.8% worked in the Female Orthopedic Department (Table 1).
The findings revealed varying levels of knowledge among nurses regarding NPPM. While most nurses recognized the primary goal of these methods, only about half understood key techniques like relaxation and distraction. Knowledge was higher for methods such as heat/cold therapy and meditation, but moderate for biofeedback, music therapy, and essential oils. Although many nurses acknowledged the importance of patient preferences, fewer understood how meditation aids pain relief. Overall, 24% had poor knowledge, 63% had moderate knowledge, and only 13% had good knowledge of NPPM (Table 2).
The findings showed varying levels of utilization of NPPM methods among nurses. Frequently used strategies included patient education, position changes, breathing techniques to ensure comfort, and involving relatives. Moderately used methods included relaxation, therapeutic touch, and electrical nerve stimulation. Less commonly practiced techniques included heat and cold application, distraction, and massage. While most nurses (76.7%) used these methods occasionally, only 15.1% applied them consistently. Considering that the instrument items range from 1 to 4 and the average total response is 2.94, the use of non-NPPM methods was generally moderate (Table 3).
The findings showed that a lack of training, limited prior knowledge, heavy workload, inadequate physician cooperation, and patient age mainly influenced nurses’ use of NPPM methods. Other factors such as staffing levels, equipment availability, and patient preferences also played a role (Figure 1).
The association between knowledge of nonpharmacological methods of pain management and sociodemographic variables is summarized below. Nurses aged 36-40 years are 7 times more likely to know NPPM methods than others. Females are 4 times more likely than males to have knowledge of NPPM methods. Christians are 9 times more likely to have knowledge about NPPM methods than non-Christians. Nurses from the Edo tribe are 5 times more likely to have knowledge of NPPM methods than others. Nurses with a Bachelor’s degree are 6 times more likely to have knowledge of NPPM methods than those with lower qualifications. Nurses with 11 or more years of service are 7 times more likely to have knowledge about NPPM methods than those with less experience. Principal Nursing Officers are 6 times more likely than other professional ranks to know NPPM methods (Table 5).
The association between the level of utilisation of NPPM methods and sociodemographic variables is summarized in Table 6. Nurses aged 36-40 years are 7 times more likely to utilise NPPM methods than other age groups. Females are 6 times more likely than males to practice NPPM methods. Christians are 7 times more likely to utilise NPPM methods compared to non-Christians. Nurses who are Edo are 4 times more likely to use NPPM methods than others. Nurses with a Bachelor’s degree are 5 times more likely to utilise NPPM methods than those with lower qualifications. Nurses with 11 or more years of service are 4 times more likely to use NPPM methods than those with less experience. Finally, Principal Nursing Officers are 6 times more likely to utilise NPPM methods than others (Table 6).
Discussion
The findings of this study reveal that the majority of nurses had moderate knowledge of NPPM strategies, suggesting a need to improve understanding and application of these methods. While the majority of nurses could identify specific strategies, such as heat or cold, fewer demonstrated a comprehensive understanding of general principles, relaxation techniques, or the purpose of music therapy. The findings indicate variability in knowledge, with specific techniques such as heat or cold and essential oils being better understood than more complex methods like distraction and biofeedback. The results are consistent with those of Manwere et al. (2015), who found that many nurses agreed on the effectiveness of distraction and other nonpharmacological interventions for mild to moderate pain. However, some gaps persist, as seen in the current study, in which only a minority had strong knowledge of general principles and advanced techniques such as biofeedback. This finding highlights the need for targeted educational interventions.
Jira et al. (2020) and Geleto et al. (2021) emphasized that factors such as education level, work experience, and nurse-to-patient ratios significantly influence knowledge and attitudes. In this study, moderate knowledge levels may also be attributed to similar factors, suggesting that enhancing educational programs and addressing systemic issues like workload could improve knowledge levels. Geleto’s findings also highlight the importance of income and working conditions in shaping attitudes, pointing to broader systemic reforms that could complement educational initiatives. Notably, studies by Mohamed et al. (2021) in Egypt and Elhusein et al. (2020) in Sudan found lower knowledge levels than this study, with reliance on pharmacological methods prevalent. The higher knowledge levels in this study may reflect differences in regional educational standards or access to resources. However, they still indicate room for growth, particularly in areas such as distraction and music therapy. The findings suggest a need to prioritize training programs focused on the principles and advanced techniques of NPPM. While nurses demonstrated strong knowledge of basic strategies such as heat or cold applications, their understanding of relaxation techniques, music therapy, and distraction as effective methods needs strengthening. Additionally, systemic factors like nurse-to-patient ratios, income, and work conditions, as noted in the literature, should be addressed to create an enabling environment for the adoption of these strategies. Incorporating NPPM into routine nursing curricula and continuing education programs could help bridge knowledge gaps and increase its utilization.
The study reveals moderate use of NPPM methods among nurses, with most using them occasionally and only a few consistently. Common practices, such as providing information to patients, encouraging position changes, teaching breathing techniques, and creating a comfortable environment, are widely used because of their simplicity and effectiveness. However, less frequently used methods, including heat and cold application, distraction, and massage, highlight gaps in training, knowledge, or accessibility. These findings align with those of Karabulut and Yaman (2016), who observed limited use of nonpharmacological techniques such as distraction and massage among Turkish nursing students, underscoring the need for curriculum updates. Similarly, Tirgari et al. (2018) noted moderate repositioning use among Iranian ICU nurses, with barriers, including fatigue, workload, and insufficient staffing. In Ethiopia, Tsegaye et al. (2020) reported that 48.1% of nurses practiced NPPM, emphasizing the role of training and pain assessment tools in improving utilization rates. Comparable barriers, such as time constraints and patient reluctance, were highlighted by Bayoumi (2021) in Egypt, which reflects the low use of distraction techniques in the current study. Systemic challenges, including nurse fatigue, poor interprofessional collaboration, and high nurse-to-patient ratios, were also noted by Tsegaye et al. (2023) in Ethiopia and Tabrizi et al. (2023) in Iran. These issues mirror findings in this study, which found that organizational obstacles hinder the consistent application of advanced techniques. Ojo and Apata (2021) and Nwaneri et al. (2018) in Nigeria, along with Kimbi et al. (2016) in Cameroon, reported moderate use of NPPM methods, with barriers, including a lack of pain assessment tools, insufficient staffing, and limited awareness. Resource availability further impacts implementation, as noted by Ojo and Apata (2021) and Khalil (2018), highlighting the need for investment in specialized equipment. Patient-related barriers, such as preferences for pharmacological methods and reluctance to participate, were also identified, aligning with Sisay’s (2017) findings. Addressing these challenges through targeted training, awareness campaigns, and patient education is critical. Recommendations from Gumus et al. (2020) and Kimbi et al. (2016) emphasize the importance of in-service training and interprofessional collaboration to enhance the adoption of NPPM practices.
The findings reveal that sociodemographic factors, including age, gender, educational qualifications, years of service, and professional rank, significantly influence nurses’ knowledge of NPPM methods. Nurses aged 36–40 years were found to be 7 times more likely to have knowledge of these techniques than their younger or older counterparts. This finding is consistent with findings from Tsegaye et al. (2023), who noted that middle-aged nurses often demonstrate higher knowledge levels due to their cumulative work experience and greater exposure to training opportunities. Female nurses were 4 times more likely than male nurses to know NPPM methods. This finding aligns with the study by Taylor et al. (2018), which highlighted gender differences in healthcare practice, where female nurses often had greater involvement in patient care, potentially increasing their familiarity with such methods. Educational qualifications were another significant factor: Nurses with a Bachelor’s degree were 6 times more likely to possess knowledge than those with lower qualifications. This finding supports those of Soriano et al. (2025) and Tsegaye et al. (2022), who identified higher education as a strong predictor of knowledge, due to more comprehensive training, including exposure to NPPM strategies. Experience also plays a crucial role, as nurses with 11 or more years of service were 7 times more likely to demonstrate knowledge than their less experienced counterparts. This finding aligns with Bayoumi (2021), who observed that longer service durations allow nurses to gain practical exposure and refine their understanding of pain management. Lastly, professional rank was significant, with Principal Nursing Officers being 6 times more likely to know nurses in lower ranks. This finding is consistent with Nwaneri et al. (2018), who noted that senior-ranking nurses are often involved in policy-making and training programs, enhancing their expertise and familiarity with advanced pain management strategies.
This study had some limitations. The cross-sectional nature of the study limits the ability to establish causal relationships between factors such as training, experience, and knowledge. Reliance on self-reported data introduces the potential for bias, as participants may over- or under-estimate their knowledge or use of nonpharmacological methods. A small sample size and limited geographic scope may restrict the generalizability of findings to a broader population of nurses or healthcare settings. The absence of objective assessments, such as patient outcomes or direct observation of practices, reduces the accuracy of nurse practice evaluations.
Implication to nursing
The study’s findings have significant implications for nursing practice. NPPM approaches in nursing curricula and ongoing professional development are essential to equip nurses with the necessary skills and knowledge. Establishing standardized protocols and guidelines can ensure consistent application across healthcare settings. Mentorship programs, where experienced nurses guide less experienced colleagues, can bridge knowledge gaps, particularly for nurses with fewer years of service. Addressing staffing challenges, such as ensuring adequate staff levels and manageable workloads, is critical for enabling nurses to implement these methods effectively. Tailored training programs for less experienced nurses, those in lower professional ranks, or male nurses can improve their familiarity with these methods. Enhanced collaboration between nurses and physicians is also crucial for the wider acceptance and implementation of NPPM strategies. Lastly, patient preferences and conditions should be considered when selecting the most appropriate pain management strategies, ensuring optimal outcomes for each patient.
Conclusion
In conclusion, the study emphasizes the significant role of NPPM approaches and techniques in nursing practice. It highlights that factors such as training, experience, and professional rank influence nurses’ knowledge and utilization of these methods. While experienced nurses tend to demonstrate better knowledge, the study underscores the need for targeted education, mentorship, and the development of standardized protocols to enhance the application of NPPM strategies across all nursing levels. Addressing systemic barriers, such as staffing issues and physician collaboration, is also crucial to improving the consistent use of these methods, ultimately leading to better patient outcomes.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of the University of Benin, Benin City, Nigeria (Code: ADM/22/A/VOL.VII14865502), and consent and permission were obtained from the participants. In addition, formal permission to conduct the study was obtained from the management of the relevant hospitals before data collection commenced. Other ethical principles, such as confidentiality and voluntary withdrawal, were strictly adhered to.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization and study design: Timothy Aghogho Ehwarieme; Data collection, data analysis, review and editing: Uzezi Josiah; Writing the original draft: Timothy Aghogho Ehwarieme and Mabel Abote; Final approval: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors appreciate the University of Benin, the management of the relevant hospitals, and the participants for their contribution to the study.
References
Abuijlan, I. A. M., Muthu, P. & Avinash, M. N., 2023. Nurses’ experience and perceived challenges of using nonpharmacological pain interventions for musculoskeletal pain: A qualitative study. SAGE Open Nursing, 9, pp. 23779608231215600. [DOI:10.1177/23779608231215600] [PMID]
Akpojaro, E., et al., 2024. An evaluation of pain assessment knowledge and management among nurses in selected hospitals in Benin-City, Edo State, Nigeria. International Journal of Research and Scientific Innovation, 11(9), pp. 300. [DOI:10.51244/IJRSI.2024.1109025]
Al Qadire M. & Al Khalaileh M., 2014. Jordanian Nurses Knowledge and Attitude Regarding Pain Management. Pain Management Nursing, 15(1), pp. 220-8. [DOI:10.1016/j.pmn.2012.08.006] [PMID]
Althubaiti, A., 2022. Sample size determination: A practical guide for health researchers. Journal of General and Family Medicine, 24(2), pp. 72-8. [DOI:10.1002/jgf2.600] [PMID]
Bayoumi, M. M. M., Khonji, L. M. A. & Gabr, W. F. M., 2021. Are nurses utilizing the nonpharmacological pain management techniques in surgical wards? Plos One, 16(10), pp. e0258668. [DOI:10.1371/journal.pone.0258668] [PMID]
Bakker, C. J., et al., 2020. Complementary and alternative medicine for postoperative pain: A systematic review. The Journal of Bone and Joint Surgery. American Volume, 102(Suppl 1), pp. 36-46. [DOI:10.2106/JBJS.19.01439] [PMID]
Bernardi, M., et al., 2007. Knowledge and attitudes about cancer pain management: A national survey of Italian oncology nurses. European Journal of Oncology Nursing, 11(3), pp. 272-9. [DOI:10.1016/j.ejon.2006.09.003] [PMID]
Bhoi, D., et al., 2021. Complementary and alternative modalities (CAM) for pain management in musculoskeletal diseases (MSDs). Journal of Clinical Orthopaedics and Trauma, 18, pp. 171-80. [DOI:10.1016/j.jcot.2021.04.021] [PMID]
Chatchumni, M., et al., 2016. Treating without Seeing: Pain Management Practice in a Thai Context. Pain Research and Management, 2016. [DOI:10.1155/2016/9580626] [PMID]
Chatchumni, M., et al., 2016. Thai Nurses’ experiences of postoperative pain assessment and its’ influence on pain management decisions. BMC Nursing, 15, pp. 12. [DOI:10.1186/s12912-016-0136-8] [PMID]
Elhusein, T., Shams, S. & Fadlallah, S., 2020. Knowledge, attitude, and practice regarding nonpharmacological pain management techniques among nurses in Sudan. Journal of Nursing Research, 28(2), pp. e102. [DOI:10.1097/jnr.0000000000000424] [PMID]
Engel, G. L., 1977. The need for a new medical model: A challenge for biomedicine. Science, 196(4286), pp. 129-36. [DOI:10.1126/science.847460] [PMID]
Ferrell, B. & McCaffery, M., 2014. Knowledge and attitudes survey regarding pain (KASRP). City of Hope Pain & Palliative Care Resource Center. [Link]
Graham, I. D., et al., 2006. Lost in knowledge translation: Time for a map? Journal of Continuing Education in the Health Professions, 26(1), pp. 13-24. [DOI:10.1002/chp.47] [PMID]
Geleto, A., et al., 2021. Knowledge, attitude, and factors associated with nurses’ use of nonpharmacological pain management in Ethiopia: A cross-sectional study. Journal of Pain Research, 14, pp. 3481-92. [DOI:10.2147/JPR.S338226]
Gumus, A., Yildirim, S. & Yildirim, G., 2020. Nonpharmacologic pain management: What it is and how it works. Liberty University Honors Theses, 1-10. [Link]
JIRA, L., Weyessa, N., Mulatu, S. & Alemayehu, A., 2020. Knowledge and attitude towards nonpharmacological pain management and associated factors among nurses working in Benishangul Gumuz Regional State Hospitals in Western Ethiopia, 2018. Journal of Pain Research, 13, pp. 2917-27. [DOI:10.2147/JPR.S265544] [PMID]
Karabulut, N., Yaman, M. & Öztürk, H., 2016. Application of nonpharmacological pain management techniques among nursing students in Eastern Turkey. Journal of Pain Management, 9(2), pp. 59-65. [DOI:10.1016/j.jpain.2016.01.004]
Khalil, N. S., 2018. Critical care nurses’ use of nonpharmacological pain management methods in Egypt. Applied Nursing Research, 44, pp. 33-8. [DOI:10.1016/j.apnr.2018.09.001] [PMID]
Kia, Z., et al., 2021. Nurses’ use of nonpharmacological pain management methods in intensive care units: A descriptive cross-sectional study. Complementary Therapies in Medicine, 58, pp. 102705. [DOI:10.1016/j.ctim.2021.102705] [PMID]
Kidanemariam, B. Y., et al., 2020. Utilization of nonpharmacological methods and the perceived barriers for adult postoperative pain management by the nurses at selectednational hospitals in Asmara, Eritrea. BMC Nursing, 19(1), pp. 1-10. [DOI:10.1186/s12912-020-00492-0] [PMID]
Kimbi, A. R. B., Ajong, N. V. S. & Tufon, E. N., 2016. Nonpharmacological interventions for pain management used by nurses at the Mezam Polyclinic Bamenda, Cameroon. Research Journal of Pharmacology and Pharmacodynamics, 8(4), pp. 157-60. [DOI:10.5958/2321-5836.2016.00028.8]
Kolcaba, K., 1994. A theory of holistic comfort for nursing. Journal of Advanced Nursing, 19(6), pp. 1178-84. [DOI:10.1111/j.1365-2648.1994.tb01202.x] [PMID]
Manwere, A., et al., 2015. Nonpharmacological pain management: Nurses’ knowledge, attitudes, and practices in selected hospitals at Makkah El-Mukarramah. Journal of Medical Research and Health Education, 4(3), pp. 1-8.
Mohamed, A. A., Elshamy, M. A. & Fayed, S. A., 2021. Nonpharmacological pain management practices among nurses in Egypt: A cross-sectional study. Journal of Pain Management Nursing, 22(3), pp. 239-46. [DOI:10.1016/j.jpain.2021.03.004]
Mohiuddin, A. K., 2019. Non-drug pain management: Opportunities to explore. United States: BiomedGrid LLC. [Link]
Niyonkuru, E., et al., 2025. Complementary approaches to postoperative pain management: A review of nonpharmacological interventions. Pain and Therapy, 14(1), pp. 121-44. [DOI:10.1007/s40122-024-00688-1] [PMID]
Nwaneri, A., et al., 2018. Nurses’ knowledge and level of utilisation of non-pharmacological pain control for orthopaedic patients in Enugu, Nigeria. International Journal of Nursing Science, 8(4), pp. 61-6. [DOI:10.5923/j.nursing.20180804.01]
Ogunfowokan, A. A. & Taiwo, O. A., 2021. A survey of nurses’ knowledge and utilization of nonpharmacological methods of pain control at two selected hospitals in Ibadan, Oyo State. International Journal of Medicine, Nursing & Health Sciences, 1(1), pp. 23-34. [Link]
Ojo, E. A. & Apata, H. O., 2021. A survey of nurses’ knowledge and utilization of nonpharmacological methods of pain control at two selected hospitals in Ibadan, Oyo State. International Journal of Medicine, Nursing & Health Sciences, 2(3), pp. 5-19. [DOI:10.5281/zenodo.5029717]
Rasheed, S. P., Sundus, A. & Younas, A., 2019. Self‐awareness in nursing: A scoping review. Journal of Clinical Nursing, 28(5-6), pp. 762-74. [DOI:10.1111/jocn.14708] [PMID]
Sisay, T., 2017. Patient-related barriers to nonpharmacological pain management: A study in Ethiopia. Journal of Pain Management, 12(3), pp. 143-50.
Şimşek, A. & Gözen, D., 2021. A study on pediatric nurses' pain management knowledge and practices in Turkey. Trends in Pediatrics, 2(4), pp. 159–64. [DOI:10.4274/TP.galenos.2021.35229]
Smith, J., Brown, K. & Williams, R., 2020. Nonpharmacological pain management in orthopedic care: A review of evidence-based practices. Journal of Pain Management, 15(3), pp. 112-25.
Soriano, G., et al., 2025. Knowledge, Attitude, and Self-Efficacy Toward Pain Management Among Filipino Nurses. Journal of Client-Centered Nursing Care, 11(3), pp. 219-28. [DOI:10.32598/JCCNC.11.3.808.1]
Swartzentruber, M., 2021. The importance of providing multimodal analgesia: A literature review of nonpharmacologic pain treatments. Liberty University Nursing Journal, pp. 1-15. [Link]
Tabrizi, F., Sadeghi, N. & Sadeghi, N., 2023. Inter-professional collaboration and associated factors among nurses and physicians working in referral and teaching hospitals in Iran. BMC Health Services Research, 23(1), pp. 1-9. [DOI:10.1186/s12913-023-09200-5] [PMID]
Taylor, S. L., et al., 2018. Gender differences in the use of complementary and integrative health therapies among veterans with chronic musculoskeletal pain. Women’s Health Issues, 28(6), pp. 497-504. [DOI:10.1016/j.whi.2018.07.004] [PMID]
Tirgari, B., Mirshekari, L. & Forouzi, A. M., 2018. Pressure injury prevention: Knowledge and attitudes of Iranian intensive care nurses. Advances in Skin & Wound Care, 31(4), pp. 1-8. [DOI:10.1097/01.ASW.0000530848.50085.ef] [PMID]
Tsegaye, D., et al., 2023. Nonpharmacological pain management practice and associated factors among nurses working at comprehensive specialized hospitals. SAGE Open Nursing, 9, pp. 23779608231158979. [DOI:10.1177/23779608231158979] [PMID]
Umar, L. B., et al., 2023. Knowledge and practice of nonpharmacological pain management techniques among nurses and midwives in Aminu Kano Teaching Hospital. Bayero Journal of Medical Laboratory Science, 8(1), pp. 104-14.
World Health Organization., 2019. Guidelines on nonpharmacological interventions for pain management. Geneva:World Health Organization.
Yamane, Y. (1967). Mathematical formulae for sample size determination.
Zeleke, S., Kassaw, A. & Eshetie, Y., 2021. Nonpharmacological pain management practice and barriers among nurses working in Debre Tabor Comprehensive Specialized Hospital, Ethiopia. Plos One, 16(6), pp. e0253086. [DOI:10.1371/journal.pone.0253086] [PMID]
Type of Study: Research |
Subject:
General
Received: 2025/02/1 | Accepted: 2025/08/31 | Published: 2026/02/1
Received: 2025/02/1 | Accepted: 2025/08/31 | Published: 2026/02/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
