Mon, Apr 27, 2026
[Archive]
Volume 12, Issue 1 (Winter 2026)
JCCNC 2026, 12(1): 99-110 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Fernandez K M, Lazaro L. Development of a Continuous Quality Improvement Program for Hemodialysis Care in a Healthcare Facility in the Philippines: A Delphi Method Approach. JCCNC 2026; 12 (1) :99-110
URL: http://jccnc.iums.ac.ir/article-1-878-en.html
URL: http://jccnc.iums.ac.ir/article-1-878-en.html



1- Department of Nursing, Trinity University of Asia-St. Luke’s School of Nursing-Graduate School, Quezon City, Philippine. , kristinemayrfernandez@tua.edu.ph
2- Department of Nursing, Trinity University of Asia-St. Luke’s School of Nursing-Graduate School, Quezon City, Philippine.
2- Department of Nursing, Trinity University of Asia-St. Luke’s School of Nursing-Graduate School, Quezon City, Philippine.
Full-Text [PDF 682 kb]
(477 Downloads)
| Abstract (HTML) (462 Views)
Full-Text: (15 Views)
Introduction
Healthcare systems are constantly evolving and integrating processes, organizations, resources, and personnel to ensure the delivery of quality care (Kruk et al., 2018; Lukas et al., 2007). Despite advancements in diagnostics, treatments, and technology, healthcare providers face significant strain due to resource constraints and the complexities inherent in these systems, resulting in inefficient patient outcomes (Al-Worafi, 2024). In the context of hemodialysis, resource limitations, data management issues, resistance to change, and adherence to regulatory standards impede the effective implementation of continuous quality improvement (CQI) (Tseng et al., 2021; Zhianfar & Shaghaghi, 2024; Zhianfar et al., 2024). Overcoming these challenges requires stakeholder engagement, continuous education, investment in infrastructure, and the adoption of data-driven strategies.
CQI is fundamental to ensuring the effectiveness and efficiency of healthcare services. It encompasses integrating knowledge, skills, and attitudes to meet the ever-changing demands of the healthcare system (Endalamaw et al., 2024). On a global scale, CQI has been shown to improve dialysis care outcomes, as demonstrated by the United States renal data system (Trenkle, 2001). In the Philippines, the Universal Health Care Act (RA 11223) emphasizes the importance of quality care, underscoring the role of CQI in achieving affordable yet high-quality healthcare (Camacho et al., 2023). The Department of Health (DOH) has implemented CQI programs in hospitals, aligning with the Philippine Health Insurance Corporation Benchbook’s objective of continuous performance enhancement. Despite these initiatives, challenges such as staff resistance and resource constraints impede the implementation of CQI in hemodialysis units (Brown & Green, 2022). Institutionalized in the Philippines through Administrative Order 2006-0002, CQI requires all DOH hospitals to establish CQI programs and committees (Camacho et al., 2023). By 2018, CQI became a licensing requirement under Department Circular No. 2018-0131, “revised licensing assessment tools for hospitals,” and is also included in the dialysis clinic licensing checklist (Ruiz, 2024).
Implementing CQI in hemodialysis requires a systematic approach, leadership commitment, data-driven decision-making, and a culture of continuous learning to ensure standardized healthcare outcomes for patients, especially those with end-stage renal disease (Taylor, 2022), in which hemodialysis nurses play an integral role in life-saving care (Slusaranskaya, 2023). Their expertise, coupled with patient education and emotional support, significantly improves patient outcomes (Lelorain et al., 2019). However, gaps in interdisciplinary collaboration, patient engagement, and regulatory understanding persist, which makes a dedicated focus on CQI in hemodialysis settings imperative (Watnick et al., 2023). Despite the DOH mandate to adopt CQI programs in hospitals, data and standardized tools remain limited for dialysis care (Tamondong-Lachica et al., 2024).
This study aims to address the existing gaps in CQI implementation regarding dialysis nursing care by identifying competencies in the selected private hospitals in Ilocos region, Philippines, and developing a CQI program specifically tailored to hemodialysis settings using the Delphi method, specifically in Ilocos region or region 1, Philippines, where there is a scarcity of data and monitoring tools.
Materials and Methods
Research design
The study employed the Delphi method, a technique designed to gather expert insights on current trends, challenges, and needs among hemodialysis nurses (Brown & Crookes, 2016). This approach utilizes iterative rounds of surveys with selected experts to forecast future developments and establish consensus (Jones, 2018), making it particularly effective for synthesizing perspectives from geographically dispersed individuals with specialized knowledge or experience in each subject (Hsu et al., 2019). Given its capacity to systematically integrate expert opinions while acknowledging individual viewpoints, the Delphi method is well-suited for program development in specialized fields (Smarandache et al., 2020).
In this study, the Delphi method consisted of two rounds. Round 1 focused on identifying initial components of an enhanced training program for quality improvement, as proposed by hemodialysis staff nurses in region 1. At the same time, round 2 refined these findings to finalize the training program. Expertise in nursing, as defined by Benner (1984), refers to practitioners who no longer rely solely on rules or guidelines but instead demonstrate intuitive, experience-based decision-making. Eligible nursing experts who met these criteria were contacted via email and provided with details about the study’s purpose and significance. It was explained to them that the study aims to address problems in the standardization of CQI in hemodialysis nursing care.
Study participants
This descriptive study employed a purposive sampling strategy to recruit 15 senior hemodialysis nurses aged 21 to 58 years from private hospitals in region 1, the Philippines. The number of panelists can range from 4 to several thousand. Typically, the number of Delphi panelists ranges from 8 to 20 (Shang, 2023).
The study specifically targeted nursing experts characterized by their advanced proficiency and adaptability in hemodialysis care. The inclusion criteria for participant selection were as follows: Registration as a nurse under the Philippine Regulation Commission with active membership in local or national Renal Nurses Association of the Philippines chapters, aged between 21 and 58 years, no restrictions regarding gender, possession of nephrology nursing certification, demonstrated clinical experience in hemodialysis settings, and capacity to provide informed consent.
Research setting
This study was conducted in the Ilocos region (region 1), located in northwestern Luzon, the Philippines. Three private hospitals equipped with hemodialysis facilities located in the provinces of Pangasinan, San Fernando (La :union:), and Ilocos Norte, Philippines, were selected.
Research instruments
For the initial phase of data collection, semi-structured interviews were employed as the primary research instrument to explore quality improvement initiatives within hemodialysis facilities. This qualitative approach used open-ended questions designed to elicit comprehensive responses, enabling participants to articulate their professional experiences and perspectives in depth. The development of the interview protocol followed a rigorous process, beginning with a thorough review of existing literature on quality improvement in hemodialysis settings to establish a theoretical foundation. Subsequently, the preliminary questions underwent critical evaluation and refinement through consultations with academic advisors, ensuring both methodological rigor and relevance to the study objectives. This systematic approach to instrument development enhanced the study’s validity while maintaining the necessary flexibility to capture the nuanced realities of hemodialysis nursing practice. To ensure the questionnaire was unambiguous, we conducted pilot testing with a small group through interviews before the main study. The questions were designed using simple, jargon-free language. We employed neutral wording throughout to eliminate potential bias and maintain objectivity in responses. The combination of evidence-based question formulation and expert validation contributed to the robustness of the data collection process, ultimately supporting the credibility of the research findings.
Data collection
Data were collected between August and September 2024 through in-depth interviews with the participants, who were given the flexibility to choose either face-to-face or virtual (via Zoom) modalities based on their convenience regarding time and location. A total of 15 interviews were completed and subsequently included in the final analysis.
Before data collection, institutional approvals were obtained from relevant hospital authorities. All interview sessions were audio-recorded following participant permission and subsequently transcribed verbatim. The interview process continued through two iterative rounds until theoretical saturation was achieved.
All digital recordings and transcripts were maintained under strict confidentiality protocols, with access restricted to the research team. Recordings were systematically reviewed to ensure data accuracy before analysis.
For the Delphi component, a structured questionnaire was developed in Google Forms, comprising 6 key sections: Program title, strategic design and rationale, learning objectives, content implementation, evaluation framework, and an open commentary section for expert feedback. The Delphi process was conducted from October to November 2024 across two sequential rounds. The initial questionnaire used a dichotomous/binary rating system, which is appropriate for Filipino participants (Suárez et al., 2024; Grassi et al., 2007; Martin et al., 1974; Paulus, 1991), and concluded with open-ended fields for additional expert commentary. According to Keeney et al. (2000), there has been intense discourse regarding the standardization of the Delphi method in nursing research, and they suggested adopting a simplified first-round question, e.g. binary, to reduce ambiguity and attrition. Lastly, preserving anonymity, individualized electronic links were distributed via secure email channels.
Furthermore, participants were given a 2-week response period for each round, with automated reminders issued at 6-day intervals. Consensus thresholds were established a priori, with items requiring ≥70% expert agreement for retention. Non-consensus items (<70% agreement) were systematically excluded, while retained items and qualitative feedback informed subsequent iterations. The second round presented a revised program version, following identical distribution and evaluation protocols. Final program components were derived exclusively from items achieving consensus across both rounds, thereby ensuring content validity through this rigorous expert validation process (see Figure 1 for the summary of the entire Delphi workflow used in the study).

Results
The participants identified different training components as important for enhancing training programs aimed at achieving quality improvement measures in hemodialysis settings.
Round 1
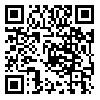
The findings in Table 1 reveal varying levels of agreement among staff regarding different training programs, with some receiving strong support and others indicating room for improvement. Programs such as leadership and management training, infection prevention and control training, and occupational safety and health (OSH) training achieved high agreement levels of 80%, reflecting staff consensus on their importance. Notably, spiritual wellness (86.66%), advanced cardiac life support (ACLS), collaboration and communication training, and adequacy of dialysis also received the highest agreement scores, emphasizing the staff’s desire for more training and organizational support in these areas.
Moderate agreement levels (66.66% to 73.33%) were observed for programs such as healthcare workers’ protection and vaccination, psychosocial support training, and basic life support (BLS), suggesting these topics may require further refinement or additional engagement with staff to address their concerns. Common focus areas across the programs included limited available resources, the need for more training, and the desire for stronger organizational support, highlighting systemic challenges within the facility.
The results underscore the importance of prioritizing high-agreement programs (≥70%) for immediate implementation while addressing underlying issues such as resource constraints and institutional support. Engaging staff in discussions about moderate-agreement programs could help tailor these initiatives to meet their needs better. Overall, the findings provide valuable insights for developing targeted quality improvement strategies in the hemodialysis facility, ensuring alignment with staff priorities and enhancing both patient care and workplace conditions.
The statistical analysis of inter-rater agreement among nursing experts regarding the initial program proposal demonstrated substantial reliability (Table 2). Fleiss’ kappa (κ=0.679), computed across 19 items evaluated by 15 raters, indicates a significant degree of concordance beyond chance expectations (Landis & Koch, 1977). This level of agreement, classified as substantial per conventional benchmarks (McHugh, 2012), was further corroborated by robust inferential statistics (z=17.8, P<0.001), which effectively rejected the null hypothesis of random agreement. The exceptionally low probability value (P<0.001) provides strong evidence that the observed consensus reflects genuine professional alignment rather than stochastic variation (Sim & Wright, 2005).

These psychometric findings carry important implications for program validation. The substantial inter-rater reliability (κ=0.679; 95% CI, 0.62%, 0.74%) suggests that the program components resonate consistently with expert expectations, a critical indicator of content validity in nursing education development (Hallgren, 2019). Such consensus is particularly noteworthy given the multidimensional nature of the evaluation criteria, which typically make perfect agreement challenging to achieve.
Round 2
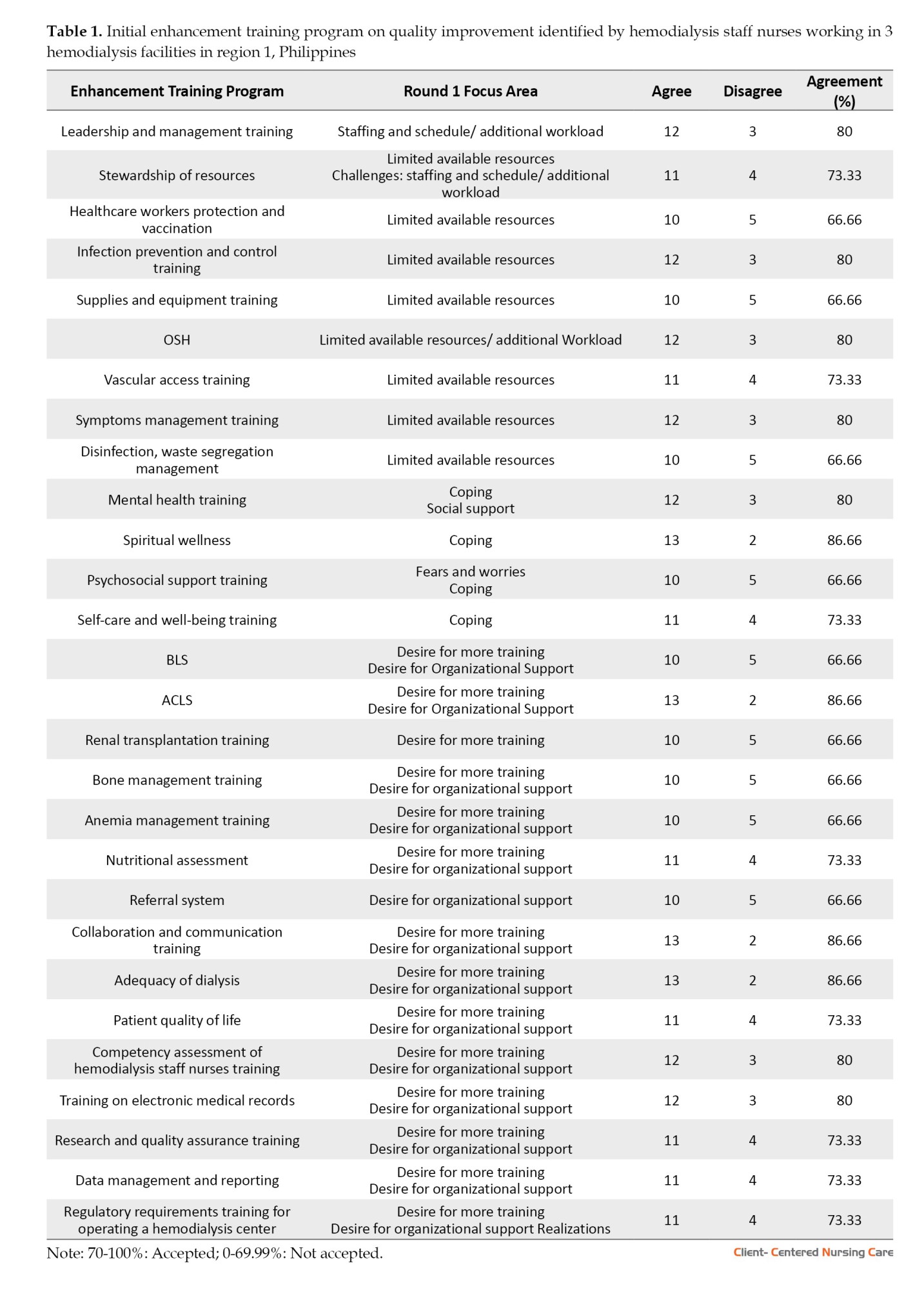
The components accepted during the first round were subject to final quality improvement. According to Table 3, most programs received acceptance, with agreement scores at or above 73.33%, indicating strong staff support. Key areas such as stewardship of resources (80%), vascular access training (80%), spiritual wellness (80%), ACLS (80%), and collaboration and communication training (80%) achieved the highest agreement, emphasizing their perceived importance in improving safety, patient-centered care, and operational efficiency. Programs like leadership and management training (73.33%), infection prevention and control training (73.33%), and OSH training (73.33%) also garnered substantial support, though slightly lower, suggesting their relevance but possibly indicating minor concerns or areas for refinement.
The domains of safety and patient-centered care were frequently associated with high-agreement programs, reinforcing their critical role in hemodialysis nursing. Meanwhile, intervention-focused programs, such as mental health training (73.33%) and self-care and well-being (73.33%), were also accepted, reflecting the staff’s recognition of the need for psychosocial and personal wellness support. Additionally, programs tied to timely, efficient, and equitable care, such as dialysis adequacy (80%), were highly endorsed, underscoring the importance of workflow optimization and equitable patient management.
Despite the overall strong agreement, the consistent presence of a minority of dissenters (3–4 “Disagree” responses across most programs) suggests that some staff may have reservations or specific unmet needs. The findings advocate for prioritizing high-agreement programs while addressing potential gaps through targeted feedback or adjustments. The broad acceptance of these training initiatives signals a collective commitment to enhancing both clinical outcomes and workplace conditions in the hemodialysis facility.
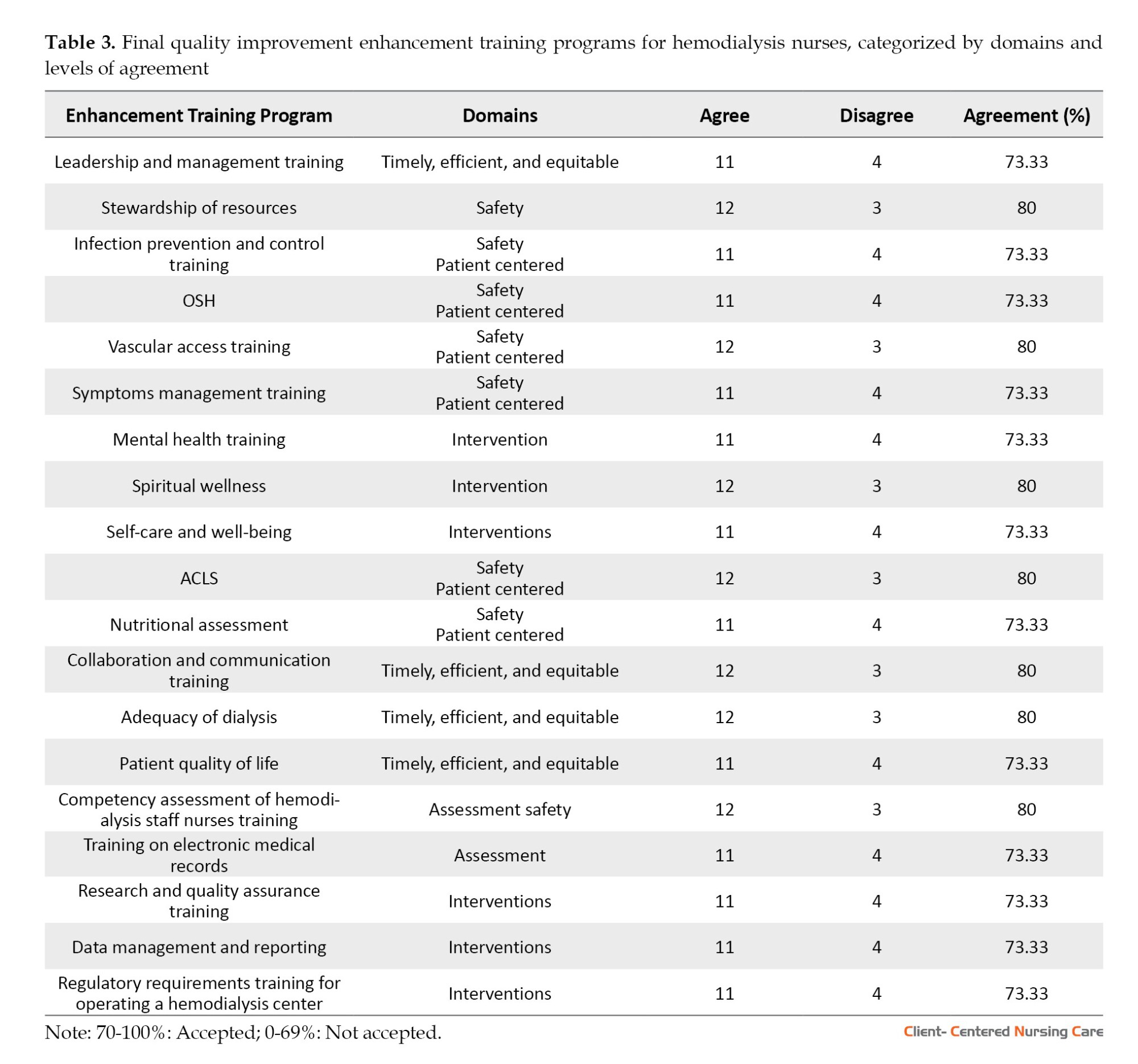
Fleiss’ kappa (κ=0.729), computed across 19 items evaluated by 15 raters, in Table 4, indicates a significant degree of concordance beyond chance expectations (Landis & Koch, 1977). This level of agreement, classified as substantial per conventional benchmarks (McHugh, 2012), was further corroborated by robust inferential statistics (z=17.8, P<0.028), which effectively rejected the null hypothesis of random agreement. The exceptionally low probability value (P<0.028) provides strong evidence that the observed consensus reflects genuine professional alignment rather than stochastic variation (Sim & Wright, 2005). These findings carry important implications for program validation. The substantial inter-rater reliability (κ=0.729; 95% CI, 0.62%, 0.74%) suggests that the program components resonate consistently with expert expectations, a critical indicator of content validity in nursing education development (Hallgren, 2019).
Content validity index (CVI) score
The evaluation of the enhancement training program on quality improvement for hemodialysis nursing practice yielded robust content validity metrics, as shown in Table 5. Quantitative analysis revealed exceptional CVI scores across all program components, with 9 of 19 domains achieving perfect unanimity (CVI=1) among the 10-member expert panel. These domains, unanimously endorsed by the panel, are leadership and management; vascular access training; spiritual wellness; interprofessional collaboration; dialysis adequacy monitoring; clinical competency assessment; electronic health records proficiency; regulatory compliance; and provider well-being. They collectively represent essential competencies for contemporary hemodialysis practice.
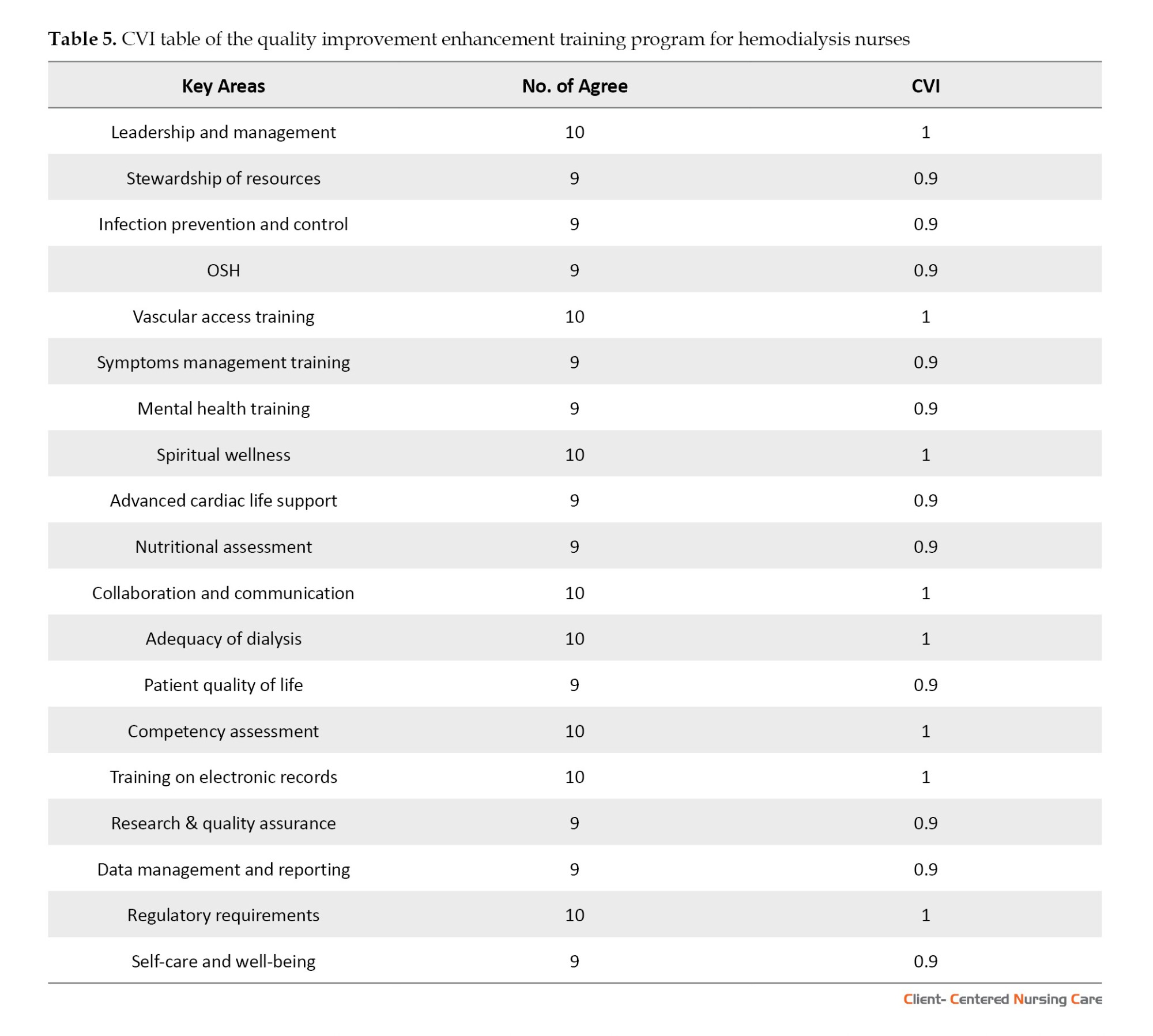
The remaining 10 program elements demonstrated near-perfect validity (CVI=0.9), indicating consensus among 90% of evaluators. These components encompass critical operational and clinical dimensions, including resource utilization efficiency, infection prevention protocols, occupational safety standards, symptom management strategies, mental health integration, advanced cardiac life support, nutritional status evaluation, quality-of-life considerations, research & quality assurance, and data management and reporting. The consistently high validity coefficients across all measured domains (Mean±SD 0.95±0.05) provide strong empirical evidence for the program’s comprehensive coverage of the requisite knowledge and skills (Polit & Beck, 2006).
Furthermore, this validity profile suggests the program successfully balances evidence-based standards with innovative practice elements, addressing both core clinical requirements and contemporary holistic care paradigms (Choi et al., 2022). These findings collectively support the program’s potential to enhance both technical proficiency and organizational outcomes in hemodialysis settings.
Discussion
The systematic refinement process from initial to final training program iterations demonstrates substantive modifications informed by expert consensus metrics. The Delphi methodology facilitated a 32.14% reduction in training domains (from 28 initial to 19 final components), with exclusions primarily affecting lower-agreement areas (below 70% threshold), including healthcare worker vaccination protocols (62%), renal transplantation education (65%), and anemia management training (68%). This strategic prioritization reflects a deliberate focus on high-impact competencies while maintaining comprehensive coverage of essential hemodialysis nursing domains, consistent with contemporary competency frameworks in specialized nursing practice.
The final program architecture reveals 3 dominant competency clusters: Clinical-technical proficiencies (vascular access management, ACLS), safety systems mastery (infection control protocols, occupational health standards), and professional development imperatives (clinical leadership, interprofessional collaboration). Notably, the differential retention rates between ACLS (80%) versus BLS training (excluded at 64%) suggest expert prioritization of higher-acuity emergency interventions, potentially reflecting the complex clinical profiles of contemporary hemodialysis populations (Clancy-Burgess, 2024). The unanimous inclusion of electronic health records training (CVI=1) further underscores the growing imperative of digital health literacy in nephrology practice (Nguyen et al., 2021).
The program’s incorporation of holistic care components, particularly spiritual wellness (CVI=1) and mental health training (CVI=0.9), signifies an important evolution toward patient-centered care paradigms in renal nursing. This dual emphasis on technical and psychosocial competencies aligns with emerging evidence demonstrating improved patient outcomes through integrated care approaches (Kearney et al., 2020), while simultaneously addressing quadruple aim objectives of enhancing both patient experiences and provider well-being (Bodenheimer & Sinsky, 2014).
The robust consensus on research methodology (CVI=0.9) and data analytics training (CVI=0.9) positions frontline nurses as active participants in evidence generation and quality improvement initiatives—a critical competency in value-based care models (Flythe et al., 2021). The program’s structured approach to competency development offers a replicable framework for specialty nursing education. However, periodic reevaluation of excluded components may be warranted as clinical evidence and practice standards evolve.
Implementation of this refined training framework holds significant potential to enhance multiple dimensions of hemodialysis care delivery. Clinically, the emphasis on vascular access competencies directly addresses a predominant complication domain in hemodialysis populations (Ravani et al., 2016). Professionally, the leadership development components empower nurses as change agents in quality improvement initiatives (Mannix et al., 2013). Organizationally, the streamlined scope enhances program adoptability while maintaining comprehensive coverage of critical competencies. However, the findings cannot be generalized to the rest of the Philippines, as the study was conducted only in the Ilocos region and involved three private hospitals. They may yield different results in other parts of the country due to cultural differences and the autonomous nature of medical practices in each region. Moreover, the study was focused on private dialysis centers; it did not include tertiary hospital settings, stand-alone dialysis centers, or dialysis units with ongoing private partnership hemodialysis settings that may have other policies on CQI.
Future directions should incorporate longitudinal evaluation of competency retention, correlation with patient outcomes, and systematic assessment of implementation barriers. This refined training architecture represents a significant advancement in hemodialysis nursing education, effectively balancing evidence-based standards with practical implementation considerations to optimize both patient care and professional practice outcomes.
Conclusion
The study highlights the pressing challenges faced by hemodialysis nurses, including staffing shortages, extended workloads, limited resources, and the complex demands of end-stage renal disease care, which often lead to burnout and compromised patient outcomes. These findings underscore the necessity for systemic reforms and enhanced support mechanisms. The proposed enhancement training program, developed with expert consensus, represents a comprehensive approach to addressing these challenges. By integrating evidence-based practices, advanced clinical training, and holistic care components, the program seeks to empower nurses with the skills and resilience needed for quality improvement in hemodialysis settings.
The final program includes 19 components with substantial expert consensus, as indicated by a Fleiss’ kappa score of 0.729. Training priorities such as infection prevention, vascular access management, mental health, and advanced clinical competencies reflect a balance between technical skills and nurses’ holistic well-being. These areas are critical for ensuring patient safety, improving outcomes, and fostering a supportive work environment. The inclusion of mental health, spiritual wellness, and professional development components underscores the importance of sustaining nurse resilience and job satisfaction, which are integral to sustaining quality improvement initiatives.
In sum, the program addresses the identified gaps in hemodialysis care through a structured, evidence-based framework. It prioritizes continuous professional growth, interdisciplinary collaboration, and a patient-centered approach to care. By equipping nurses with the necessary tools and support systems, this training initiative promises to improve care quality, enhance patient outcomes, and ensure the well-being of both patients and nurses in hemodialysis settings.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by Ethics Review Committee (ERC) of Trinity University of Asia, Quezon City, Philippine (Code: 2024-1st-CNU-Fernandez-V1). The research ensured compliance with ethical safeguards. It followed guidelines to ensure that participants took part willingly and voluntarily in a safe environment. The data were handled in a manner that ensured anonymity, confidentiality, and privacy. The respondents had the right to withdraw from the study at any time. A cover letter was attached to each informed consent form, explaining the study details. Stringent measures were implemented to protect participant confidentiality, including the use of pseudonyms derived from common hemodialysis medications to anonymize individual identities throughout the study. Furthermore, the study findings were made available to a selected research locale and its participants upon request for future research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interception of the results and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors sincerely thank all nurses who participated in this study. The authors also appreciates the institution Trinity University of Asia, Quezon City, Philippine.
References
Healthcare systems are constantly evolving and integrating processes, organizations, resources, and personnel to ensure the delivery of quality care (Kruk et al., 2018; Lukas et al., 2007). Despite advancements in diagnostics, treatments, and technology, healthcare providers face significant strain due to resource constraints and the complexities inherent in these systems, resulting in inefficient patient outcomes (Al-Worafi, 2024). In the context of hemodialysis, resource limitations, data management issues, resistance to change, and adherence to regulatory standards impede the effective implementation of continuous quality improvement (CQI) (Tseng et al., 2021; Zhianfar & Shaghaghi, 2024; Zhianfar et al., 2024). Overcoming these challenges requires stakeholder engagement, continuous education, investment in infrastructure, and the adoption of data-driven strategies.
CQI is fundamental to ensuring the effectiveness and efficiency of healthcare services. It encompasses integrating knowledge, skills, and attitudes to meet the ever-changing demands of the healthcare system (Endalamaw et al., 2024). On a global scale, CQI has been shown to improve dialysis care outcomes, as demonstrated by the United States renal data system (Trenkle, 2001). In the Philippines, the Universal Health Care Act (RA 11223) emphasizes the importance of quality care, underscoring the role of CQI in achieving affordable yet high-quality healthcare (Camacho et al., 2023). The Department of Health (DOH) has implemented CQI programs in hospitals, aligning with the Philippine Health Insurance Corporation Benchbook’s objective of continuous performance enhancement. Despite these initiatives, challenges such as staff resistance and resource constraints impede the implementation of CQI in hemodialysis units (Brown & Green, 2022). Institutionalized in the Philippines through Administrative Order 2006-0002, CQI requires all DOH hospitals to establish CQI programs and committees (Camacho et al., 2023). By 2018, CQI became a licensing requirement under Department Circular No. 2018-0131, “revised licensing assessment tools for hospitals,” and is also included in the dialysis clinic licensing checklist (Ruiz, 2024).
Implementing CQI in hemodialysis requires a systematic approach, leadership commitment, data-driven decision-making, and a culture of continuous learning to ensure standardized healthcare outcomes for patients, especially those with end-stage renal disease (Taylor, 2022), in which hemodialysis nurses play an integral role in life-saving care (Slusaranskaya, 2023). Their expertise, coupled with patient education and emotional support, significantly improves patient outcomes (Lelorain et al., 2019). However, gaps in interdisciplinary collaboration, patient engagement, and regulatory understanding persist, which makes a dedicated focus on CQI in hemodialysis settings imperative (Watnick et al., 2023). Despite the DOH mandate to adopt CQI programs in hospitals, data and standardized tools remain limited for dialysis care (Tamondong-Lachica et al., 2024).
This study aims to address the existing gaps in CQI implementation regarding dialysis nursing care by identifying competencies in the selected private hospitals in Ilocos region, Philippines, and developing a CQI program specifically tailored to hemodialysis settings using the Delphi method, specifically in Ilocos region or region 1, Philippines, where there is a scarcity of data and monitoring tools.
Materials and Methods
Research design
The study employed the Delphi method, a technique designed to gather expert insights on current trends, challenges, and needs among hemodialysis nurses (Brown & Crookes, 2016). This approach utilizes iterative rounds of surveys with selected experts to forecast future developments and establish consensus (Jones, 2018), making it particularly effective for synthesizing perspectives from geographically dispersed individuals with specialized knowledge or experience in each subject (Hsu et al., 2019). Given its capacity to systematically integrate expert opinions while acknowledging individual viewpoints, the Delphi method is well-suited for program development in specialized fields (Smarandache et al., 2020).
In this study, the Delphi method consisted of two rounds. Round 1 focused on identifying initial components of an enhanced training program for quality improvement, as proposed by hemodialysis staff nurses in region 1. At the same time, round 2 refined these findings to finalize the training program. Expertise in nursing, as defined by Benner (1984), refers to practitioners who no longer rely solely on rules or guidelines but instead demonstrate intuitive, experience-based decision-making. Eligible nursing experts who met these criteria were contacted via email and provided with details about the study’s purpose and significance. It was explained to them that the study aims to address problems in the standardization of CQI in hemodialysis nursing care.
Study participants
This descriptive study employed a purposive sampling strategy to recruit 15 senior hemodialysis nurses aged 21 to 58 years from private hospitals in region 1, the Philippines. The number of panelists can range from 4 to several thousand. Typically, the number of Delphi panelists ranges from 8 to 20 (Shang, 2023).
The study specifically targeted nursing experts characterized by their advanced proficiency and adaptability in hemodialysis care. The inclusion criteria for participant selection were as follows: Registration as a nurse under the Philippine Regulation Commission with active membership in local or national Renal Nurses Association of the Philippines chapters, aged between 21 and 58 years, no restrictions regarding gender, possession of nephrology nursing certification, demonstrated clinical experience in hemodialysis settings, and capacity to provide informed consent.
Research setting
This study was conducted in the Ilocos region (region 1), located in northwestern Luzon, the Philippines. Three private hospitals equipped with hemodialysis facilities located in the provinces of Pangasinan, San Fernando (La :union:), and Ilocos Norte, Philippines, were selected.
Research instruments
For the initial phase of data collection, semi-structured interviews were employed as the primary research instrument to explore quality improvement initiatives within hemodialysis facilities. This qualitative approach used open-ended questions designed to elicit comprehensive responses, enabling participants to articulate their professional experiences and perspectives in depth. The development of the interview protocol followed a rigorous process, beginning with a thorough review of existing literature on quality improvement in hemodialysis settings to establish a theoretical foundation. Subsequently, the preliminary questions underwent critical evaluation and refinement through consultations with academic advisors, ensuring both methodological rigor and relevance to the study objectives. This systematic approach to instrument development enhanced the study’s validity while maintaining the necessary flexibility to capture the nuanced realities of hemodialysis nursing practice. To ensure the questionnaire was unambiguous, we conducted pilot testing with a small group through interviews before the main study. The questions were designed using simple, jargon-free language. We employed neutral wording throughout to eliminate potential bias and maintain objectivity in responses. The combination of evidence-based question formulation and expert validation contributed to the robustness of the data collection process, ultimately supporting the credibility of the research findings.
Data collection
Data were collected between August and September 2024 through in-depth interviews with the participants, who were given the flexibility to choose either face-to-face or virtual (via Zoom) modalities based on their convenience regarding time and location. A total of 15 interviews were completed and subsequently included in the final analysis.
Before data collection, institutional approvals were obtained from relevant hospital authorities. All interview sessions were audio-recorded following participant permission and subsequently transcribed verbatim. The interview process continued through two iterative rounds until theoretical saturation was achieved.
All digital recordings and transcripts were maintained under strict confidentiality protocols, with access restricted to the research team. Recordings were systematically reviewed to ensure data accuracy before analysis.
For the Delphi component, a structured questionnaire was developed in Google Forms, comprising 6 key sections: Program title, strategic design and rationale, learning objectives, content implementation, evaluation framework, and an open commentary section for expert feedback. The Delphi process was conducted from October to November 2024 across two sequential rounds. The initial questionnaire used a dichotomous/binary rating system, which is appropriate for Filipino participants (Suárez et al., 2024; Grassi et al., 2007; Martin et al., 1974; Paulus, 1991), and concluded with open-ended fields for additional expert commentary. According to Keeney et al. (2000), there has been intense discourse regarding the standardization of the Delphi method in nursing research, and they suggested adopting a simplified first-round question, e.g. binary, to reduce ambiguity and attrition. Lastly, preserving anonymity, individualized electronic links were distributed via secure email channels.
Furthermore, participants were given a 2-week response period for each round, with automated reminders issued at 6-day intervals. Consensus thresholds were established a priori, with items requiring ≥70% expert agreement for retention. Non-consensus items (<70% agreement) were systematically excluded, while retained items and qualitative feedback informed subsequent iterations. The second round presented a revised program version, following identical distribution and evaluation protocols. Final program components were derived exclusively from items achieving consensus across both rounds, thereby ensuring content validity through this rigorous expert validation process (see Figure 1 for the summary of the entire Delphi workflow used in the study).
Results
The participants identified different training components as important for enhancing training programs aimed at achieving quality improvement measures in hemodialysis settings.
Round 1
The findings in Table 1 reveal varying levels of agreement among staff regarding different training programs, with some receiving strong support and others indicating room for improvement. Programs such as leadership and management training, infection prevention and control training, and occupational safety and health (OSH) training achieved high agreement levels of 80%, reflecting staff consensus on their importance. Notably, spiritual wellness (86.66%), advanced cardiac life support (ACLS), collaboration and communication training, and adequacy of dialysis also received the highest agreement scores, emphasizing the staff’s desire for more training and organizational support in these areas.
Moderate agreement levels (66.66% to 73.33%) were observed for programs such as healthcare workers’ protection and vaccination, psychosocial support training, and basic life support (BLS), suggesting these topics may require further refinement or additional engagement with staff to address their concerns. Common focus areas across the programs included limited available resources, the need for more training, and the desire for stronger organizational support, highlighting systemic challenges within the facility.
The results underscore the importance of prioritizing high-agreement programs (≥70%) for immediate implementation while addressing underlying issues such as resource constraints and institutional support. Engaging staff in discussions about moderate-agreement programs could help tailor these initiatives to meet their needs better. Overall, the findings provide valuable insights for developing targeted quality improvement strategies in the hemodialysis facility, ensuring alignment with staff priorities and enhancing both patient care and workplace conditions.
The statistical analysis of inter-rater agreement among nursing experts regarding the initial program proposal demonstrated substantial reliability (Table 2). Fleiss’ kappa (κ=0.679), computed across 19 items evaluated by 15 raters, indicates a significant degree of concordance beyond chance expectations (Landis & Koch, 1977). This level of agreement, classified as substantial per conventional benchmarks (McHugh, 2012), was further corroborated by robust inferential statistics (z=17.8, P<0.001), which effectively rejected the null hypothesis of random agreement. The exceptionally low probability value (P<0.001) provides strong evidence that the observed consensus reflects genuine professional alignment rather than stochastic variation (Sim & Wright, 2005).
These psychometric findings carry important implications for program validation. The substantial inter-rater reliability (κ=0.679; 95% CI, 0.62%, 0.74%) suggests that the program components resonate consistently with expert expectations, a critical indicator of content validity in nursing education development (Hallgren, 2019). Such consensus is particularly noteworthy given the multidimensional nature of the evaluation criteria, which typically make perfect agreement challenging to achieve.
Round 2
The components accepted during the first round were subject to final quality improvement. According to Table 3, most programs received acceptance, with agreement scores at or above 73.33%, indicating strong staff support. Key areas such as stewardship of resources (80%), vascular access training (80%), spiritual wellness (80%), ACLS (80%), and collaboration and communication training (80%) achieved the highest agreement, emphasizing their perceived importance in improving safety, patient-centered care, and operational efficiency. Programs like leadership and management training (73.33%), infection prevention and control training (73.33%), and OSH training (73.33%) also garnered substantial support, though slightly lower, suggesting their relevance but possibly indicating minor concerns or areas for refinement.
The domains of safety and patient-centered care were frequently associated with high-agreement programs, reinforcing their critical role in hemodialysis nursing. Meanwhile, intervention-focused programs, such as mental health training (73.33%) and self-care and well-being (73.33%), were also accepted, reflecting the staff’s recognition of the need for psychosocial and personal wellness support. Additionally, programs tied to timely, efficient, and equitable care, such as dialysis adequacy (80%), were highly endorsed, underscoring the importance of workflow optimization and equitable patient management.
Despite the overall strong agreement, the consistent presence of a minority of dissenters (3–4 “Disagree” responses across most programs) suggests that some staff may have reservations or specific unmet needs. The findings advocate for prioritizing high-agreement programs while addressing potential gaps through targeted feedback or adjustments. The broad acceptance of these training initiatives signals a collective commitment to enhancing both clinical outcomes and workplace conditions in the hemodialysis facility.
Fleiss’ kappa (κ=0.729), computed across 19 items evaluated by 15 raters, in Table 4, indicates a significant degree of concordance beyond chance expectations (Landis & Koch, 1977). This level of agreement, classified as substantial per conventional benchmarks (McHugh, 2012), was further corroborated by robust inferential statistics (z=17.8, P<0.028), which effectively rejected the null hypothesis of random agreement. The exceptionally low probability value (P<0.028) provides strong evidence that the observed consensus reflects genuine professional alignment rather than stochastic variation (Sim & Wright, 2005). These findings carry important implications for program validation. The substantial inter-rater reliability (κ=0.729; 95% CI, 0.62%, 0.74%) suggests that the program components resonate consistently with expert expectations, a critical indicator of content validity in nursing education development (Hallgren, 2019).
Content validity index (CVI) score
The evaluation of the enhancement training program on quality improvement for hemodialysis nursing practice yielded robust content validity metrics, as shown in Table 5. Quantitative analysis revealed exceptional CVI scores across all program components, with 9 of 19 domains achieving perfect unanimity (CVI=1) among the 10-member expert panel. These domains, unanimously endorsed by the panel, are leadership and management; vascular access training; spiritual wellness; interprofessional collaboration; dialysis adequacy monitoring; clinical competency assessment; electronic health records proficiency; regulatory compliance; and provider well-being. They collectively represent essential competencies for contemporary hemodialysis practice.
The remaining 10 program elements demonstrated near-perfect validity (CVI=0.9), indicating consensus among 90% of evaluators. These components encompass critical operational and clinical dimensions, including resource utilization efficiency, infection prevention protocols, occupational safety standards, symptom management strategies, mental health integration, advanced cardiac life support, nutritional status evaluation, quality-of-life considerations, research & quality assurance, and data management and reporting. The consistently high validity coefficients across all measured domains (Mean±SD 0.95±0.05) provide strong empirical evidence for the program’s comprehensive coverage of the requisite knowledge and skills (Polit & Beck, 2006).
Furthermore, this validity profile suggests the program successfully balances evidence-based standards with innovative practice elements, addressing both core clinical requirements and contemporary holistic care paradigms (Choi et al., 2022). These findings collectively support the program’s potential to enhance both technical proficiency and organizational outcomes in hemodialysis settings.
Discussion
The systematic refinement process from initial to final training program iterations demonstrates substantive modifications informed by expert consensus metrics. The Delphi methodology facilitated a 32.14% reduction in training domains (from 28 initial to 19 final components), with exclusions primarily affecting lower-agreement areas (below 70% threshold), including healthcare worker vaccination protocols (62%), renal transplantation education (65%), and anemia management training (68%). This strategic prioritization reflects a deliberate focus on high-impact competencies while maintaining comprehensive coverage of essential hemodialysis nursing domains, consistent with contemporary competency frameworks in specialized nursing practice.
The final program architecture reveals 3 dominant competency clusters: Clinical-technical proficiencies (vascular access management, ACLS), safety systems mastery (infection control protocols, occupational health standards), and professional development imperatives (clinical leadership, interprofessional collaboration). Notably, the differential retention rates between ACLS (80%) versus BLS training (excluded at 64%) suggest expert prioritization of higher-acuity emergency interventions, potentially reflecting the complex clinical profiles of contemporary hemodialysis populations (Clancy-Burgess, 2024). The unanimous inclusion of electronic health records training (CVI=1) further underscores the growing imperative of digital health literacy in nephrology practice (Nguyen et al., 2021).
The program’s incorporation of holistic care components, particularly spiritual wellness (CVI=1) and mental health training (CVI=0.9), signifies an important evolution toward patient-centered care paradigms in renal nursing. This dual emphasis on technical and psychosocial competencies aligns with emerging evidence demonstrating improved patient outcomes through integrated care approaches (Kearney et al., 2020), while simultaneously addressing quadruple aim objectives of enhancing both patient experiences and provider well-being (Bodenheimer & Sinsky, 2014).
The robust consensus on research methodology (CVI=0.9) and data analytics training (CVI=0.9) positions frontline nurses as active participants in evidence generation and quality improvement initiatives—a critical competency in value-based care models (Flythe et al., 2021). The program’s structured approach to competency development offers a replicable framework for specialty nursing education. However, periodic reevaluation of excluded components may be warranted as clinical evidence and practice standards evolve.
Implementation of this refined training framework holds significant potential to enhance multiple dimensions of hemodialysis care delivery. Clinically, the emphasis on vascular access competencies directly addresses a predominant complication domain in hemodialysis populations (Ravani et al., 2016). Professionally, the leadership development components empower nurses as change agents in quality improvement initiatives (Mannix et al., 2013). Organizationally, the streamlined scope enhances program adoptability while maintaining comprehensive coverage of critical competencies. However, the findings cannot be generalized to the rest of the Philippines, as the study was conducted only in the Ilocos region and involved three private hospitals. They may yield different results in other parts of the country due to cultural differences and the autonomous nature of medical practices in each region. Moreover, the study was focused on private dialysis centers; it did not include tertiary hospital settings, stand-alone dialysis centers, or dialysis units with ongoing private partnership hemodialysis settings that may have other policies on CQI.
Future directions should incorporate longitudinal evaluation of competency retention, correlation with patient outcomes, and systematic assessment of implementation barriers. This refined training architecture represents a significant advancement in hemodialysis nursing education, effectively balancing evidence-based standards with practical implementation considerations to optimize both patient care and professional practice outcomes.
Conclusion
The study highlights the pressing challenges faced by hemodialysis nurses, including staffing shortages, extended workloads, limited resources, and the complex demands of end-stage renal disease care, which often lead to burnout and compromised patient outcomes. These findings underscore the necessity for systemic reforms and enhanced support mechanisms. The proposed enhancement training program, developed with expert consensus, represents a comprehensive approach to addressing these challenges. By integrating evidence-based practices, advanced clinical training, and holistic care components, the program seeks to empower nurses with the skills and resilience needed for quality improvement in hemodialysis settings.
The final program includes 19 components with substantial expert consensus, as indicated by a Fleiss’ kappa score of 0.729. Training priorities such as infection prevention, vascular access management, mental health, and advanced clinical competencies reflect a balance between technical skills and nurses’ holistic well-being. These areas are critical for ensuring patient safety, improving outcomes, and fostering a supportive work environment. The inclusion of mental health, spiritual wellness, and professional development components underscores the importance of sustaining nurse resilience and job satisfaction, which are integral to sustaining quality improvement initiatives.
In sum, the program addresses the identified gaps in hemodialysis care through a structured, evidence-based framework. It prioritizes continuous professional growth, interdisciplinary collaboration, and a patient-centered approach to care. By equipping nurses with the necessary tools and support systems, this training initiative promises to improve care quality, enhance patient outcomes, and ensure the well-being of both patients and nurses in hemodialysis settings.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by Ethics Review Committee (ERC) of Trinity University of Asia, Quezon City, Philippine (Code: 2024-1st-CNU-Fernandez-V1). The research ensured compliance with ethical safeguards. It followed guidelines to ensure that participants took part willingly and voluntarily in a safe environment. The data were handled in a manner that ensured anonymity, confidentiality, and privacy. The respondents had the right to withdraw from the study at any time. A cover letter was attached to each informed consent form, explaining the study details. Stringent measures were implemented to protect participant confidentiality, including the use of pseudonyms derived from common hemodialysis medications to anonymize individual identities throughout the study. Furthermore, the study findings were made available to a selected research locale and its participants upon request for future research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interception of the results and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors sincerely thank all nurses who participated in this study. The authors also appreciates the institution Trinity University of Asia, Quezon City, Philippine.
References
Al-Worafi, Y. M., Ming, L. C. & Alseragi, W. M., 2024. Patient care-related issues in the developing countries: Patient education and counseling. In: Y. M. Al-Worafi (Ed.), Handbook of Medical and Health Sciences in Developing Countries (pp. 1-19). Berlin: Springer International Publishing. [DOI:10.1007/978-3-030-74786-2_245-1]
Benner, P., 1984. From novice to expert: Excellence and power in clinical nursing practice. Menlo Park: Addison-Wesley. [DOI:10.1097/00000446-198412000-00025]
Brown, R. A. & Crookes, P. A., 2016. What level of competency do experienced nurses expect from newly graduated registered nurses? Results of an Australian modified Delphi study. Bmc Nursing, 15, pp. 45. [DOI:10.1186/s12912-016-0166-2] [PMID]
Bodenheimer, T. & Sinsky, C., 2014. From triple to quadruple aim: Care of the patient requires care of the provider. The Annals of Family Medicine, 12(6), pp. 573-6. [DOI:10.1370/afm.1713] [PMID]
Brown, E. & Green, M., 2022. Enhancing Hemodialysis Outcomes Through Continuous Quality Improvement: Strategies and Results. Renal Care Advances, 40(2), pp. 78-90.
Camacho, J. C. M., Garcia, G. & Sales, R. K., 2023. Rapid Landscape Assessment of the Current Systems and Capacities to Purchase for Quality at the Primary Care Level in the Philippines. [Link]
Choi, T. M., et al., 2022. Disruptive technologies and operations management in the Industry 4.0 era and beyond. Production and Operations Management. [DOI:10.1111/poms.13622]
Clancy-Burgess, S. C., 2024. Implementing Change: Training for Adult Emergency Assessment, Recognition, and Stabilization for Novice and Non-Critical Care Nurses [MA thesis]. Durham: University of New Hampshire. [Link]
Endalamaw, A., et al., 2024. A scoping review of continuous quality improvement in healthcare system: Conceptualization, models and tools, barriers and facilitators, and impact. BMC Health Services Research, 24(1), pp. 487. [DOI:10.1186/s12913-024-10828-0] [PMID]
Flythe, J. E., et al., 2021. Development of a preliminary conceptual model of the patient experience of chronic kidney disease: A targeted literature review and analysis. BMC Nephrology, 22(1), pp. 233. [DOI:10.1186/s12882-021-02440-9] [PMID]
Grassi, M., et al., 2007. Performance comparison of Likert and binary formats of SF-36 version 1.6 across ECRHS II adults populations. Value in Health, 10(6), pp. 478-88. [DOI:10.1111/j.1524-4733.2007.00203.x] [PMID]
Hallgren, K. A., 2019. Computing inter-rater reliability for observational data: An overview and tutorial. Tutorials in Quantitative Methods for Psychology, 8(1), pp. 23-34. [DOI:10.20982/tqmp.08.1.p023] [PMID]
Hsu, C. C. & Sandford, B. A., 2007. The Delphi technique: Making sense of consensus. Practical Assessment, Research, and Evaluation, 12, pp. 1-8. [DOI:10.7275/pdz9-th90]
Jones, J., 2018. Research Methods for Librarians and Educators: Practical Applications in Formal and Informal Learning Environments. Bloomsbury: Bloomsbury Publishing. [Link]
Kearney, L. K., et al., 2020. Global approaches to integrated care: Best practices and ongoing innovation. American Psychologist, 75(5), pp. 668. [DOI:10.1037/amp0000490] [PMID]
Keeney, S., Hasson, F. & McKenna, H. P., 2001. A critical review of the Delphi technique as a research methodology for nursing. International Journal of Nursing Studies, 38(2), pp.195-200. [DOI:10.1016/S0020-7489(00)00044-4] [PMID]
Kruk, M. E., et al., 2018. High-quality health systems in the Sustainable Development Goals era: Time for a revolution. The Lancet Global Health, 6(11), pp. e1196-252 [DOI:10.1016/S2214-109X(18)30386-3] [PMID]
Landis, J. R. & Koch, G. G., 1977. The measurement of observer agreement for categorical data. Biometrics, 33(1), pp. 159-74. [DOI:10.2307/2529310] [PMID]
Lelorain, S., et al., 2019. Nurses’ and nursing assistants’ emotional skills: A major determinant of motivation for patient education. Journal of Advanced Nursing, 75(11), pp. 2616-26. [DOI:10.1111/jan.14033] [PMID]
Lukas, C. V., et al., 2007. Transformational change in health care systems: an organizational model. Health Care Management Review, 32(4), pp. 309-20. [DOI:10.1097/01.HMR.0000296785.29718.5d] [PMID]
Mannix, J., Wilkes, L. & Daly, J., 2013. Attributes of clinical leadership in contemporary nursing: An integrative review. Contemporary Nurse, 45(1), pp. 10-21. [DOI:10.5172/conu.2013.45.1.10] [PMID]
Martin, W. S., Fruchter, B. & Mathis, W. J., 1974. An investigation of the effect of the number of scale intervals on principal components factor analysis. Educational and Psychological Measurement, 34(3), pp. 537-45. [DOI:10.1177/001316447403400307]
McHugh, M. L., 2012. Interrater reliability: The kappa statistic. Biochemia Medica, 22(3), pp. 276-82. [DOI:10.11613/BM.2012.031] [PMID]
Nguyen, M. H., et al., 2021. Negative impact of fear of COVID-19 on health-related quality of life Was modified by health literacy, eHealth literacy, and digital healthy diet literacy: A multi-hospital survey. International Journal of Environmental Research and Public Health, 18(9). [DOI:10.3390/ijerph18094929] [PMID]
Paulhus, D. L., 1991. Measurement and control of response bias. [Link]
Polit, D. F. & Beck, C. T., 2006. The content validity index: are you sure you know what’s being reported? Critique and recommendations. Research in Nursing & Health, 29(5), pp. 489-97. [DOI:10.1002/nur.20147] [PMID]
Ravani, P., et al., 2016. Pre‐emptive correction for haemodialysis arteriovenous access stenosis. Cochrane Database of Systematic Reviews, (1). [DOI:10.1002/14651858.CD010709.pub2] [PMID]
Ruiz, Engr., 2024. Observance of Health Care Waste Management Performance Standards in Selected Hospitals. Journal of Waste Management & Recycling Technology. pp. 1-3. [DOI:10.47363/JWMRT/2024(2)133]
Shang, Z., 2023. Use of Delphi in health sciences research: A narrative review. Medicine (Baltimore), 102(7), pp. e32829. [DOI:10.1097/MD.0000000000032829] [PMID]
Sim, J. & Wright, C. C., 2020. The kappa statistic in reliability studies: Use, interpretation, and sample size requirements. Physical Therapy, 85(3), pp. 257-68. [DOI:10.1093/ptj/85.3.257] [PMID]
Slusaranskaya, M., 2023. Nursing aspects of hemodialysis, its significance and special features of its nephrological applications [PhD dissertation]. Ternopil. [Link]
Smarandache, F., et al., 2020. Delphi method for evaluating scientific research proposals in a neutrosophic environment. Infinite Study. [Link]
Suárez-García, A., et al., 2024. Exploring the efficacy of binary surveys versus likert scales in assessing student perspectives using bayesian analysis. Applied Sciences, 14(10), pp. 4189. [DOI:10.3390/app14104189]
Tamondong-Lachica, D. R., et al., 2024. Description of core performance measures and indicators of patient safety used by select government and private hospitals in the Philippines. Acta Medica Philippina, 58(1), pp. 15-24. [DOI:10.47895/amp.vi0.6931] [PMID]
Taylor, K. S., 2022. Contextual predictors of hospitalization and quality of life among people on hemodialysis [PhD dissertation]. Johns Hopkins University. [Link]
Trenkle, J. A., 2001. Implementing continuous quality improvement strategies for improving iron replacement in hemodialysis patients. Nephrology Nursing Journal: Journal of The American Nephrology Nurses' Association, 28(5), pp. 561–5. [PMID]
Tseng, P. L., et al, 2021. Overcoming barriers to maintain hemodialysis adequacy amongst hemodialysis patients in hospital: A best practice implementation project. JBI Evidence Implementation, 19(3), pp. 315-26. [DOI:10.1097/XEB.0000000000000280] [PMID]
Watnick, S., et al., 2023. System-level strategies to improve home dialysis: policy levers and quality initiatives. Clinical Journal of the American Society of Nephrology, 18(12), pp. 1616-25. [DOI:10.2215/CJN.0000000000000299] [PMID]
Zhianfar, L., Nadrian, H. & Shaghaghi, A., 2024. A benchmarking and evidence-informed gap analysis of the hemodialysis care provision in Iran. BMC Health Services Research, 24(1), pp. 1608. [DOI:10.1186/s12913-024-12054-0] [PMID]
Type of Study: Research |
Subject:
Special
Received: 2025/04/22 | Accepted: 2025/07/13 | Published: 2026/02/1
Received: 2025/04/22 | Accepted: 2025/07/13 | Published: 2026/02/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright © The Author(s);
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
